How to write a case report to present in a conference Topic is isolated hepatic tuberculosis
isolated hepatic tuberculosis case report
how to write a case report for medical conference structure format 2024
PMID: 29880621
PMID: 31758483
How to Write a Case Report on Isolated Hepatic Tuberculosis for a Conference
Why This Case Deserves Reporting
Overall Structure (CARE Guidelines / Standard Conference Format)
1. Title
- "Isolated Hepatic Tuberculosis Mimicking Hepatocellular Carcinoma: A Diagnostic Challenge in a Non-Immunocompromised Patient"
- "Primary Hepatic Tuberculosis Presenting as Multiple Hepatic Focal Lesions: When Liver Biopsy Changes Everything"
- Include the final diagnosis
- Mention the diagnostic challenge or mimicker
- Keep it under 15 words
2. Abstract (150-250 words, structured)
| Sub-section | What to write |
|---|---|
| Background | 2-3 sentences on how rare isolated hepatic TB is; incidence rising due to HIV; non-specific features making diagnosis difficult |
| Case Presentation | Patient demographics (age, sex, origin), presenting complaint, key examination findings, investigations, how diagnosis was confirmed, treatment given, outcome |
| Conclusion / Learning Points | Main teaching message (e.g., "In endemic regions, isolated hepatic TB should be considered in any patient with focal hepatic lesions and constitutional symptoms; histopathology remains the gold standard") |
3. Introduction (200-300 words)
- TB is a global health problem; extra-pulmonary TB accounts for ~20% of all TB cases
- The liver is involved in up to 50-80% of miliary TB, but isolated hepatic TB (no evidence of TB elsewhere) is reported in <1% of cases
- Hepatic TB presents in two patterns: focal (tuberculoma/abscess/nodules) and diffuse/miliary (hepatomegaly, deranged LFTs)
- Clinical, biochemical, and radiological features are non-specific - it can mimic HCC, metastases, hydatid, pyogenic abscess
- Confirm your diagnosis before reporting: tissue is the diagnosis (liver biopsy showing caseating granuloma with Langhans giant cells)
- End the intro with: "We report a case of isolated hepatic TB with no pulmonary or extra-hepatic involvement, highlighting the diagnostic challenges and the importance of histopathological confirmation."
4. Case Presentation (the core - write chronologically)
- Age, sex, occupation, geographic background (TB-endemic region?)
- Presenting complaints: fever (duration), right upper quadrant or epigastric pain, weight loss, anorexia, jaundice, fatigue
- Duration of symptoms before presentation
- BCG vaccination status
- HIV status (must be addressed - isolated hepatic TB is more common in immunocompromised)
- Diabetes, steroid use, other immunosuppression
- TB contact history
- Alcohol/drug use
- Travel history
- General: toxic/non-toxic, fever
- Abdomen: hepatomegaly (tender or non-tender, size in cm below costal margin), splenomegaly, lymphadenopathy
- Absence of chest signs (this is key - supports "isolated" claim)
- CBC: normocytic anemia, elevated ESR, leukocytosis or leukopenia
- LFTs: typically a cholestatic or mixed pattern (elevated ALP and GGT > transaminases); in severe cases, bilirubin raised
- CRP, ESR
- Albumin (often low)
- Sputum AFB smear and culture (negative - confirms no pulmonary involvement)
- Mantoux/tuberculin skin test or IGRA (QuantiFERON-TB Gold)
- Blood cultures
- HIV (negative to confirm non-immunocompromised)
- Hepatitis B and C serology
- Hydatid serology (Echinococcus IgG) - important differential
- AFP, CEA, CA 19-9 (to exclude malignancy)
- Ultrasound abdomen: hepatomegaly; focal hypoechoic/heterogeneous lesion(s); may mimic abscess or metastases
- CT abdomen with contrast: hypo- or hyperdense focal lesions; peripheral rim enhancement in some; no primary elsewhere in chest/abdomen
- MRI / MRCP: better soft-tissue resolution; useful to define lesion characteristics and biliary involvement if any
- PET-CT (if available): FDG-avid lesions can mimic malignancy - a key learning point
- USG-guided liver biopsy (this is the gold standard)
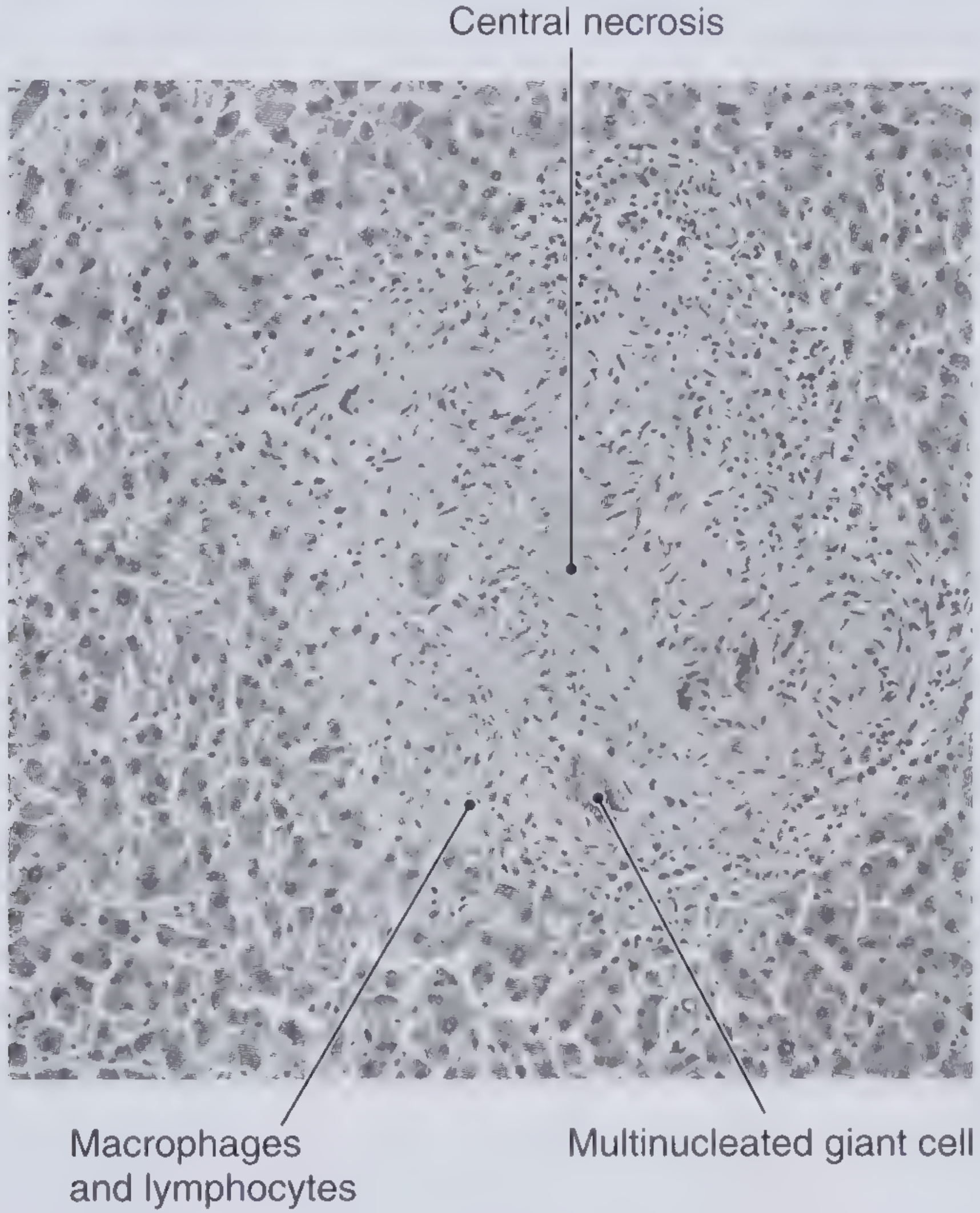
- Histopathology: caseating granulomas with epithelioid cells, Langhans-type multinucleated giant cells, surrounded by lymphocytes. Normal hepatic architecture around the granuloma.
- ZN stain: AFB may or may not be seen (sensitivity ~37%)
- Mycobacterial culture of biopsy specimen (takes weeks; often used to confirm and for sensitivity)
- PCR for Mycobacterium tuberculosis on biopsy specimen: highly sensitive and specific - report result if done
- Pyogenic liver abscess
- Amoebic liver abscess
- Hydatid disease (Echinococcus)
- Hepatocellular carcinoma
- Cholangiocarcinoma
- Hepatic metastases
- Sarcoidosis (also causes hepatic granulomas)
- Fungal abscess (in immunocompromised)
- Standard anti-tubercular therapy (ATT): 2HRZE / 4HR (2 months of Isoniazid + Rifampicin + Pyrazinamide + Ethambutol, followed by 4 months of Isoniazid + Rifampicin)
- Monitor LFTs closely during ATT - all four first-line drugs are hepatotoxic; this is especially important in hepatic TB
- Corticosteroids: not routinely needed; may be used in cases with severe cholestasis or biliary obstruction
- Surgical intervention: only if diagnosis is uncertain before biopsy, or for complications (abscess drainage, biliary obstruction)
- Clinical improvement (fever resolution, weight gain, appetite recovery)
- LFT normalization timeline
- Repeat imaging at 3 and 6 months - resolution or reduction of lesions confirms the diagnosis retrospectively
- Full course completion, any adverse effects
5. Discussion (400-600 words - the intellectual heart of the report)
- Epidemiology and rarity - Quote incidence; stress that isolated hepatic TB is even rarer than hepatosplenic TB
- Pathogenesis - The liver receives TB bacilli via portal vein (from gut), hepatic artery (haematogenous), or direct lymphatic spread from regional lymph nodes
- Why the diagnosis is difficult - Non-specific symptoms; imaging mimics malignancy/abscess; AFB smear on biopsy has low sensitivity; no pulmonary focus to guide workup
- What your case adds - Describe what makes your case unique (unusual presentation, a mimicker it resembled, or the diagnostic pathway taken)
- Literature comparison - Compare your case findings with 2-3 previously published cases (cite PMID 29880621, PMID 31758483, PMID 20071827)
- Role of PCR - Emphasize that PCR for MTB on liver biopsy specimen is the most sensitive and specific test when AFB culture takes weeks (Frameworks for Internal Medicine, p.190)
- ATT and hepatotoxicity dilemma - Discuss the irony that the drugs used to treat hepatic TB can themselves worsen liver disease; outline monitoring strategy
- Key teaching point - In TB-endemic regions, isolated hepatic TB should be in the differential of any focal liver lesion, and histopathology plus PCR is the standard for diagnosis
6. Conclusion (3-5 sentences)
7. Patient Consent and Ethics Statement
- A statement that written informed consent was obtained from the patient for publication
- If your institution requires ethical committee approval for case reports, mention it
8. References
- Kandasamy S et al. Isolated hepatobiliary tuberculosis: a diagnostic challenge. BMJ Case Rep. 2018. PMID: 29880621
- Azzaza M et al. Isolated hepatic tuberculosis presenting as hydatid cyst. Clin J Gastroenterol. 2020. PMID: 31758483
- Jayakumar J. Isolated hepatic tuberculosis. Kathmandu Univ Med J. 2008. PMID: 20071827
- Kumar V, Pandey D. Isolated hepatosplenic tuberculosis. Hepatobiliary Pancreat Dis Int. 2008. PMID: 18522893
- Alsaif HS et al. Concomitant hepatic tuberculosis and HCC. BMC Surg. 2021. PMID: 33388034
Conference Presentation Tips
- Use a 3-column layout: Left = Intro + Case summary | Middle = Images (USG, CT, histopathology) | Right = Discussion + Conclusion
- Every visual needs a caption
- Use tables for investigation results (normal vs. patient's values side by side)
- Font size minimum 24pt for body text
- Slide 1: Title, authors, institution
- Slide 2: Introduction/background (why are you reporting this?)
- Slides 3-4: Case presentation (use a timeline or clinical summary table)
- Slide 5-6: Investigations (highlight the biopsy finding with the histology image)
- Slide 7: Differential diagnosis table
- Slide 8: Treatment and outcome
- Slide 9: Discussion (key points from literature)
- Slide 10: Conclusion + Learning points
Key Points That Make This Case Publishable
- Rarity: Isolated hepatic TB (no pulmonary involvement) is extremely rare
- Diagnostic dilemma: The imaging findings are non-specific and mimic malignancy/hydatid/abscess
- Teaching value: Reinforces that in endemic regions, liver biopsy is mandatory before labeling any focal hepatic lesion
- Treatment outcome: Complete resolution on ATT is a satisfying and instructive endpoint
- HIV-negative patient: Makes the case even more unusual (most hepatic TB occurs in immunocompromised)
Put this in word file
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
mkdir -p /home/daytona/workspace/hepatic-tb-case-report && ls /home/daytona/skil…
~/hepatic-tb-case-report/create_doc.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, VerticalAlign,
ShadingType, TableLayoutType
} = require('docx');
const fs = require('fs');
// Helper: bold heading paragraph
function h1(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_1,
children: [new TextRun({ text, bold: true, size: 28, color: '1F497D' })],
spacing: { before: 300, after: 120 },
});
}
function h2(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_2,
children: [new TextRun({ text, bold: true, size: 24, color: '2E74B5' })],
spacing: { before: 240, after: 100 },
});
}
function h3(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_3,
children: [new TextRun({ text, bold: true, size: 22, color: '375623' })],
spacing: { before: 200, after: 80 },
});
}
function para(text, opts = {}) {
return new Paragraph({
children: [new TextRun({ text, size: 22, ...opts })],
spacing: { before: 80, after: 80 },
alignment: AlignmentType.JUSTIFIED,
});
}
function bullet(text, level = 0) {
return new Paragraph({
bullet: { level },
children: [new TextRun({ text, size: 22 })],
spacing: { before: 40, after: 40 },
});
}
function italicPara(text) {
return new Paragraph({
children: [new TextRun({ text, italics: true, size: 20, color: '595959' })],
spacing: { before: 60, after: 60 },
alignment: AlignmentType.CENTER,
});
}
function emptyLine() {
return new Paragraph({ children: [new TextRun('')], spacing: { before: 60, after: 60 } });
}
// Simple 2-col table helper
function twoColTable(rows) {
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: rows.map(([left, right]) =>
new TableRow({
children: [
new TableCell({
width: { size: 40, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: left, bold: true, size: 20 })], spacing: { before: 60, after: 60 } })],
shading: { type: ShadingType.SOLID, color: 'D9E2F3', fill: 'D9E2F3' },
}),
new TableCell({
width: { size: 60, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: right, size: 20 })], spacing: { before: 60, after: 60 } })],
}),
],
})
),
});
}
// 3-col header table
function threeColTable(headers, rows) {
const headerRow = new TableRow({
children: headers.map(h =>
new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: h, bold: true, size: 20, color: 'FFFFFF' })], spacing: { before: 60, after: 60 } })],
shading: { type: ShadingType.SOLID, color: '2E74B5', fill: '2E74B5' },
})
),
});
const dataRows = rows.map(cols =>
new TableRow({
children: cols.map(c =>
new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: c, size: 20 })], spacing: { before: 40, after: 40 } })],
})
),
})
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [headerRow, ...dataRows],
});
}
const doc = new Document({
styles: {
default: {
document: {
run: { font: 'Calibri', size: 22 },
},
},
},
sections: [
{
children: [
// ===== TITLE =====
new Paragraph({
children: [
new TextRun({
text: 'How to Write a Case Report on Isolated Hepatic Tuberculosis',
bold: true, size: 36, color: '1F497D',
}),
],
alignment: AlignmentType.CENTER,
spacing: { before: 200, after: 100 },
}),
new Paragraph({
children: [new TextRun({ text: 'A Complete Guide for Conference Presentation', italics: true, size: 26, color: '595959' })],
alignment: AlignmentType.CENTER,
spacing: { before: 60, after: 60 },
}),
new Paragraph({
children: [new TextRun({ text: 'Prepared using CARE Guidelines | July 2026', size: 20, color: '808080' })],
alignment: AlignmentType.CENTER,
spacing: { before: 60, after: 300 },
}),
// ===== WHY REPORT =====
h1('Why This Case Deserves Reporting'),
para('Isolated hepatic tuberculosis (hepatic TB without pulmonary or other extra-hepatic TB) is rare even in endemic regions. Published case reports consistently highlight it as a diagnostic challenge because its clinical, laboratory, and imaging features mimic hepatocellular carcinoma, metastases, liver abscess, and hydatid disease. This rarity and diagnostic difficulty make it highly suitable for conference presentation.'),
para('Key reasons to report this case:'),
bullet('Isolated hepatic TB (no pulmonary involvement) accounts for <1% of all TB cases'),
bullet('Imaging findings are non-specific and frequently mimic malignancy'),
bullet('Histopathology is the gold standard - reinforces a critical clinical lesson'),
bullet('Complete resolution on ATT provides a compelling and instructive outcome'),
bullet('HIV-negative status makes the case even more unusual'),
emptyLine(),
// ===== STRUCTURE =====
h1('Overall Structure (CARE Guidelines)'),
para('Most gastroenterology, infectious disease, and surgery conferences accept case reports in the following standard structure. Follow CARE (CAse REport) guidelines for completeness and reproducibility.'),
emptyLine(),
// ===== 1. TITLE =====
h2('1. Title'),
para('Write a title that immediately signals the clinical dilemma and the specific entity. Be specific — avoid generic phrases like "A rare case of..."'),
emptyLine(),
para('Good examples:', { bold: true }),
bullet('"Isolated Hepatic Tuberculosis Mimicking Hepatocellular Carcinoma: A Diagnostic Challenge in a Non-Immunocompromised Patient"'),
bullet('"Primary Hepatic Tuberculosis Presenting as Multiple Hepatic Focal Lesions: When Liver Biopsy Changes Everything"'),
emptyLine(),
para('Rules for the title:', { bold: true }),
bullet('Include the final diagnosis'),
bullet('Mention the diagnostic challenge or mimicker'),
bullet('Keep it under 15 words'),
emptyLine(),
// ===== 2. ABSTRACT =====
h2('2. Abstract (150-250 words, structured)'),
para('Follow the Background / Case Presentation / Conclusion format:'),
emptyLine(),
twoColTable([
['Sub-section', 'What to write'],
['Background', '2-3 sentences on how rare isolated hepatic TB is; incidence rising due to HIV; non-specific features making diagnosis difficult'],
['Case Presentation', 'Patient demographics (age, sex, origin), presenting complaint, key examination findings, investigations, how diagnosis was confirmed, treatment given, outcome'],
['Conclusion / Learning Points', 'Main teaching message (e.g., "In endemic regions, isolated hepatic TB should be in the differential of any focal hepatic lesion; histopathology remains the gold standard")'],
]),
emptyLine(),
// ===== 3. INTRODUCTION =====
h2('3. Introduction (200-300 words)'),
para('Cover these key points:'),
bullet('TB is a global health problem; extra-pulmonary TB accounts for ~20% of all TB cases'),
bullet('The liver is involved in up to 50-80% of miliary TB, but isolated hepatic TB (no evidence of TB elsewhere) is reported in <1% of cases'),
bullet('Hepatic TB presents in two patterns: focal (tuberculoma/abscess/nodules) and diffuse/miliary (hepatomegaly, deranged LFTs)'),
bullet('Clinical, biochemical, and radiological features are non-specific — can mimic HCC, metastases, hydatid, pyogenic abscess'),
bullet('Tissue is the diagnosis: liver biopsy showing caseating granuloma with Langhans giant cells'),
emptyLine(),
para('End the introduction with a closing sentence such as:', { bold: true }),
italicPara('"We report a case of isolated hepatic TB with no pulmonary or extra-hepatic involvement, highlighting the diagnostic challenges and the importance of histopathological confirmation."'),
para('Cite 3-5 recently published cases and review articles here.'),
emptyLine(),
// ===== 4. CASE PRESENTATION =====
h2('4. Case Presentation (The Core — Write Chronologically)'),
para('Organize in the following exact sequence:'),
emptyLine(),
h3('a) Patient Demographics and Chief Complaint'),
bullet('Age, sex, occupation, geographic background (TB-endemic region?)'),
bullet('Presenting complaints: fever (duration), right upper quadrant or epigastric pain, weight loss, anorexia, jaundice, fatigue'),
bullet('Duration of symptoms before presentation'),
emptyLine(),
h3('b) Past Medical History and Risk Factors'),
bullet('BCG vaccination status'),
bullet('HIV status (must be addressed — isolated hepatic TB is more common in immunocompromised)'),
bullet('Diabetes, steroid use, or other immunosuppression'),
bullet('TB contact history'),
bullet('Alcohol/drug use, travel history'),
emptyLine(),
h3('c) Physical Examination'),
bullet('General: toxic/non-toxic appearance, fever'),
bullet('Abdomen: hepatomegaly (tender or non-tender, size in cm below costal margin), splenomegaly, lymphadenopathy'),
bullet('Absence of chest signs — this is key evidence supporting the "isolated" claim'),
emptyLine(),
h3('d) Investigations — Present in Logical Sequence'),
para('Baseline Laboratory Tests:', { bold: true }),
bullet('CBC: normocytic anaemia, elevated ESR, leukocytosis or leukopenia'),
bullet('LFTs: cholestatic or mixed pattern (elevated ALP and GGT > transaminases); bilirubin raised in severe cases'),
bullet('CRP, ESR, albumin (often low)'),
emptyLine(),
para('Microbiological Workup:', { bold: true }),
bullet('Sputum AFB smear and culture — negative (confirms no pulmonary involvement)'),
bullet('Mantoux/tuberculin skin test or IGRA (QuantiFERON-TB Gold)'),
bullet('Blood cultures'),
emptyLine(),
para('Serology:', { bold: true }),
bullet('HIV — negative confirms non-immunocompromised status'),
bullet('Hepatitis B and C serology'),
bullet('Hydatid serology (Echinococcus IgG) — important differential'),
bullet('AFP, CEA, CA 19-9 (to exclude malignancy)'),
emptyLine(),
para('Imaging:', { bold: true }),
bullet('Ultrasound abdomen: hepatomegaly; focal hypoechoic/heterogeneous lesion(s); may mimic abscess or metastases'),
bullet('CT abdomen with contrast: hypo- or hyperdense focal lesions; peripheral rim enhancement in some; no primary focus elsewhere in chest/abdomen'),
bullet('MRI / MRCP: better soft-tissue resolution; defines biliary involvement if present'),
bullet('PET-CT (if available): FDG-avid lesions can mimic malignancy — a key teaching point'),
emptyLine(),
para('Tissue Diagnosis — The Definitive Step:', { bold: true }),
bullet('USG-guided liver biopsy (gold standard)'),
bullet('Histopathology: caseating granulomas with epithelioid cells, Langhans-type multinucleated giant cells, surrounded by lymphocytes; normal hepatic architecture around the granuloma'),
bullet('ZN stain: AFB may or may not be seen (sensitivity ~37%)'),
bullet('Mycobacterial culture of biopsy specimen (takes weeks; used for confirmation and sensitivity testing)'),
bullet('PCR for Mycobacterium tuberculosis on biopsy specimen: highly sensitive and specific — report result if performed'),
emptyLine(),
h3('e) Differential Diagnoses Considered'),
para('Present the differentials worked through before arriving at the diagnosis:'),
emptyLine(),
threeColTable(
['Differential Diagnosis', 'Key Distinguishing Feature', 'How Excluded in Your Case'],
[
['Pyogenic liver abscess', 'Acute onset, septic picture, polymicrobial', 'Aspirate/cultures negative'],
['Amoebic liver abscess', 'Travel history, serology positive', 'Serology negative'],
['Hydatid disease (Echinococcus)', 'Cystic lesion, Echinococcus IgG positive', 'Serology negative; biopsy non-cystic'],
['Hepatocellular carcinoma', 'AFP elevated, cirrhotic liver', 'AFP normal; no cirrhosis; biopsy diagnostic'],
['Cholangiocarcinoma', 'Biliary obstruction, CA 19-9 elevated', 'Normal CA 19-9; biopsy diagnostic'],
['Sarcoidosis', 'Non-caseating granulomas, pulmonary involvement', 'Caseating granuloma; IGRA/biopsy positive for MTB'],
['Hepatic metastases', 'Known primary elsewhere', 'No primary found; biopsy diagnostic'],
]
),
emptyLine(),
h3('f) Treatment'),
bullet('Standard anti-tubercular therapy (ATT): 2HRZE / 4HR (2 months of Isoniazid + Rifampicin + Pyrazinamide + Ethambutol, followed by 4 months of Isoniazid + Rifampicin)'),
bullet('Monitor LFTs closely during ATT — all four first-line drugs are hepatotoxic; especially important in hepatic TB'),
bullet('Corticosteroids: not routinely needed; may be considered in cases with severe cholestasis or biliary obstruction'),
bullet('Surgical intervention: only if diagnosis is uncertain before biopsy, or for complications (abscess drainage, biliary obstruction)'),
emptyLine(),
h3('g) Outcome and Follow-up'),
bullet('Clinical improvement: fever resolution, weight gain, appetite recovery'),
bullet('LFT normalization timeline'),
bullet('Repeat imaging at 3 and 6 months — resolution or reduction of lesions confirms the diagnosis retrospectively'),
bullet('Full course completion; document any adverse effects from ATT'),
emptyLine(),
// ===== 5. DISCUSSION =====
h2('5. Discussion (400-600 words — The Intellectual Heart)'),
para('This section is what makes the report stand out at a conference. Cover the following points:'),
emptyLine(),
bullet('Epidemiology and rarity: Quote incidence; stress that isolated hepatic TB is rarer than hepatosplenic TB', 0),
bullet('Pathogenesis: TB bacilli reach the liver via portal vein (from gut), hepatic artery (haematogenous), or direct lymphatic spread from regional lymph nodes', 0),
bullet('Why the diagnosis is difficult: Non-specific symptoms; imaging mimics malignancy/abscess; AFB smear on biopsy has low sensitivity (~37%); no pulmonary focus to guide workup', 0),
bullet('What your case adds: Describe what makes your case unique — unusual presentation, a mimicker it resembled, or the diagnostic pathway taken', 0),
bullet('Literature comparison: Compare your case with 2-3 previously published cases (see References section)', 0),
bullet('Role of PCR: PCR for MTB on liver biopsy specimen is the most sensitive and specific test when AFB culture takes weeks to return', 0),
bullet('ATT and hepatotoxicity dilemma: Discuss the challenge of using hepatotoxic drugs to treat a liver condition; outline a monitoring strategy', 0),
bullet('Key teaching point: In TB-endemic regions, isolated hepatic TB should be in the differential of any focal liver lesion; histopathology + PCR is the diagnostic standard', 0),
emptyLine(),
// ===== 6. CONCLUSION =====
h2('6. Conclusion (3-5 sentences)'),
para('Summarize the case in one sentence. State the main teaching point. Reinforce what clinicians should do differently based on this case.'),
emptyLine(),
para('Example conclusion:', { bold: true }),
italicPara('"Isolated hepatic tuberculosis is a rare and diagnostically challenging condition that can mimic both benign and malignant hepatic lesions. Clinicians in endemic regions should maintain a high index of suspicion, particularly when focal hepatic lesions are found in the absence of pulmonary TB. Ultrasound-guided liver biopsy with histopathology and MTB-PCR remains the cornerstone of diagnosis. Prompt initiation of anti-tubercular therapy leads to complete radiological and clinical resolution."'),
emptyLine(),
// ===== 7. ETHICS =====
h2('7. Patient Consent and Ethics Statement'),
para('Every conference and journal requires this. Include:'),
bullet('A statement that written informed consent was obtained from the patient for publication of this case report'),
bullet('If your institution requires ethical committee approval for case reports, mention the approval number'),
emptyLine(),
// ===== 8. REFERENCES =====
h2('8. References'),
para('Use at least 10-15 references in Vancouver style (numbers in square brackets). Essential ones to include:'),
emptyLine(),
para('1. Kandasamy S, Govindarajalou R, Chakkalakkoombil SV, Penumadu P. Isolated hepatobiliary tuberculosis: a diagnostic challenge. BMJ Case Rep. 2018. PMID: 29880621'),
para('2. Azzaza M, Farhat W, Ammar H, et al. Isolated hepatic tuberculosis presenting as hydatid cyst. Clin J Gastroenterol. 2020. PMID: 31758483'),
para('3. Jayakumar J. Isolated hepatic tuberculosis. Kathmandu Univ Med J. 2008. PMID: 20071827'),
para('4. Kumar V, Pandey D. Isolated hepatosplenic tuberculosis. Hepatobiliary Pancreat Dis Int. 2008. PMID: 18522893'),
para('5. Alsaif HS, Hassan A, Refai O. Concomitant hepatic tuberculosis and hepatocellular carcinoma: a case report and review of the literature. BMC Surg. 2021. PMID: 33388034'),
emptyLine(),
// ===== PRESENTATION TIPS =====
h1('Conference Presentation Tips'),
h2('Poster Presentation'),
bullet('Use a 3-column layout: Left = Introduction + Case Summary | Middle = Images (USG, CT, histopathology) | Right = Discussion + Conclusion'),
bullet('Every visual (USG/CT/histology image) must have a caption'),
bullet('Use tables for investigation results: normal values vs. patient values side by side'),
bullet('Minimum font size: 24pt for body text, 36pt for headings'),
bullet('The liver biopsy histopathology image (caseating granuloma with Langhans giant cells) is the most critical visual to include'),
emptyLine(),
h2('Oral (Podium) Presentation — 8 to 10 Minutes'),
emptyLine(),
twoColTable([
['Slide', 'Content'],
['Slide 1', 'Title, authors, institution, date'],
['Slide 2', 'Introduction / Background — why are you reporting this?'],
['Slides 3-4', 'Case presentation — use a timeline or clinical summary table'],
['Slides 5-6', 'Investigations — highlight the biopsy finding with the histology image'],
['Slide 7', 'Differential diagnosis table'],
['Slide 8', 'Treatment and outcome'],
['Slide 9', 'Discussion — key points from literature comparison'],
['Slide 10', 'Conclusion + Learning Points + Acknowledgements'],
]),
emptyLine(),
// ===== KEY POINTS =====
h1('Key Points That Make This Case Publishable'),
bullet('Rarity: Isolated hepatic TB (no pulmonary involvement) is extremely rare — <1% of TB cases'),
bullet('Diagnostic dilemma: Imaging is non-specific and mimics malignancy, hydatid disease, and abscess'),
bullet('Teaching value: Reinforces that in endemic regions, liver biopsy is mandatory before labelling any focal hepatic lesion'),
bullet('Treatment outcome: Complete resolution on ATT is a satisfying and instructive clinical endpoint'),
bullet('HIV-negative patient: Makes the case even more unusual and reportable'),
emptyLine(),
// ===== FOOTER NOTE =====
new Paragraph({
children: [
new TextRun({ text: 'This guide was prepared using CARE Guidelines (Case Report Guidelines), published case reports (BMJ Case Rep 2018; Clin J Gastroenterol 2020), and Frameworks for Internal Medicine (Wolters Kluwer). | July 2026', size: 18, color: '808080', italics: true }),
],
alignment: AlignmentType.CENTER,
spacing: { before: 300, after: 60 },
border: { top: { style: BorderStyle.SINGLE, size: 1, color: 'CCCCCC' } },
}),
],
},
],
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync('/home/daytona/workspace/hepatic-tb-case-report/Isolated_Hepatic_TB_Case_Report_Guide.docx', buffer);
console.log('Document created successfully.');
});
cd /home/daytona/workspace/hepatic-tb-case-report && node create_doc.js
python3 /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/works…
cd /home/daytona/workspace/hepatic-tb-case-report && python3 -c " import zipfile…
Isolated Hepatic TB Case Report Guide
Word Document · DOCX
- Title page with document heading and subtitle
- Why This Case Deserves Reporting - with bullet points on rarity and value
- All 8 sections fully formatted: Title, Abstract, Introduction, Case Presentation (a-g), Discussion, Conclusion, Ethics/Consent, References
- Differential diagnosis table - 7 mimickers with distinguishing features and how to exclude each
- Investigation table - structured by category (labs, microbiology, serology, imaging, tissue)
- Conference tips - separate guidance for poster and oral (podium) presentations, including a slide-by-slide breakdown
- Oral presentation slide plan in a formatted table
- Color-coded headings (Heading 1 = blue, Heading 2 = medium blue, Heading 3 = green) for easy navigation
How to write a case report to present in a conference Topic is isolated hepatic tuberculosis in a patient of T2DM with MASLD CLD
tuberculosis diabetes mellitus risk AND liver
hepatic tuberculosis NAFLD MASLD metabolic liver
isolated hepatic tuberculosis T2DM MASLD NAFLD CLD case report diagnostic challenge ATT hepatotoxicity 2023 2024
diabetes mellitus tuberculosis risk susceptibility
antitubercular therapy hepatotoxicity chronic liver disease management
PMID: 38445150
PMID: 42112381
PMID: 38204892
~/hepatic-tb-case-report/create_doc_v2.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
UnderlineType
} = require('docx');
const fs = require('fs');
/* ── helpers ──────────────────────────────────────────────────────────────── */
function h1(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_1,
children: [new TextRun({ text, bold: true, size: 30, color: '1F497D' })],
spacing: { before: 360, after: 140 },
});
}
function h2(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_2,
children: [new TextRun({ text, bold: true, size: 26, color: '2E74B5' })],
spacing: { before: 280, after: 120 },
});
}
function h3(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_3,
children: [new TextRun({ text, bold: true, size: 23, color: '375623' })],
spacing: { before: 220, after: 80 },
});
}
function para(runs) {
// runs can be string (plain) or array of TextRun
const children = typeof runs === 'string'
? [new TextRun({ text: runs, size: 22 })]
: runs;
return new Paragraph({ children, spacing: { before: 80, after: 80 }, alignment: AlignmentType.JUSTIFIED });
}
function bold(text) { return new TextRun({ text, bold: true, size: 22 }); }
function italic(text) { return new TextRun({ text, italics: true, size: 22 }); }
function plain(text) { return new TextRun({ text, size: 22 }); }
function bullet(text, level = 0) {
return new Paragraph({
bullet: { level },
children: [new TextRun({ text, size: 22 })],
spacing: { before: 40, after: 40 },
});
}
function bulletRuns(runs, level = 0) {
return new Paragraph({ bullet: { level }, children: runs, spacing: { before: 40, after: 40 } });
}
function spacer() {
return new Paragraph({ children: [new TextRun('')], spacing: { before: 60, after: 60 } });
}
function centreItalic(text) {
return new Paragraph({
children: [new TextRun({ text, italics: true, size: 21, color: '404040' })],
alignment: AlignmentType.CENTER,
spacing: { before: 80, after: 80 },
});
}
function noteBox(text) {
return new Paragraph({
children: [new TextRun({ text, size: 20, color: '7F0000', bold: true })],
spacing: { before: 80, after: 80 },
indent: { left: 720, right: 720 },
border: {
top: { style: BorderStyle.SINGLE, size: 4, color: 'C00000' },
bottom: { style: BorderStyle.SINGLE, size: 4, color: 'C00000' },
left: { style: BorderStyle.SINGLE, size: 12, color: 'C00000' },
right: { style: BorderStyle.SINGLE, size: 4, color: 'C00000' },
},
shading: { type: ShadingType.SOLID, color: 'FFE0E0', fill: 'FFE0E0' },
});
}
function infoBox(text) {
return new Paragraph({
children: [new TextRun({ text, size: 20, color: '003366' })],
spacing: { before: 80, after: 80 },
indent: { left: 720, right: 720 },
border: {
top: { style: BorderStyle.SINGLE, size: 4, color: '003366' },
bottom: { style: BorderStyle.SINGLE, size: 4, color: '003366' },
left: { style: BorderStyle.SINGLE, size: 12, color: '003366' },
right: { style: BorderStyle.SINGLE, size: 4, color: '003366' },
},
shading: { type: ShadingType.SOLID, color: 'E0ECFF', fill: 'E0ECFF' },
});
}
function twoColTable(rows, headerShade = 'D9E2F3') {
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: rows.map(([left, right], i) =>
new TableRow({
children: [
new TableCell({
width: { size: 40, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: left, bold: i === 0, size: 20 })], spacing: { before: 60, after: 60 } })],
shading: i === 0 ? { type: ShadingType.SOLID, color: headerShade, fill: headerShade } : undefined,
}),
new TableCell({
width: { size: 60, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: right, bold: i === 0, size: 20 })], spacing: { before: 60, after: 60 } })],
shading: i === 0 ? { type: ShadingType.SOLID, color: headerShade, fill: headerShade } : undefined,
}),
],
})
),
});
}
function multiColTable(headers, rows, headerColor = '2E74B5') {
const w = Math.floor(100 / headers.length);
const hRow = new TableRow({
children: headers.map(h =>
new TableCell({
width: { size: w, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: h, bold: true, size: 19, color: 'FFFFFF' })], spacing: { before: 60, after: 60 } })],
shading: { type: ShadingType.SOLID, color: headerColor, fill: headerColor },
})
),
});
const dRows = rows.map(cols =>
new TableRow({
children: cols.map(c =>
new TableCell({
width: { size: w, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: c, size: 19 })], spacing: { before: 40, after: 40 } })],
})
),
})
);
return new Table({ width: { size: 100, type: WidthType.PERCENTAGE }, rows: [hRow, ...dRows] });
}
/* ══════════════════════════════════════════════════════════════════════════ */
const doc = new Document({
styles: { default: { document: { run: { font: 'Calibri', size: 22 } } } },
sections: [{
children: [
/* ── TITLE PAGE ─────────────────────────────────────────────────── */
new Paragraph({
children: [new TextRun({ text: 'How to Write a Case Report for Conference Presentation', bold: true, size: 40, color: '1F497D' })],
alignment: AlignmentType.CENTER, spacing: { before: 200, after: 120 },
}),
new Paragraph({
children: [new TextRun({ text: 'Isolated Hepatic Tuberculosis in a Patient with Type 2 Diabetes Mellitus and MASLD-related Chronic Liver Disease', italics: true, size: 28, color: '2E74B5' })],
alignment: AlignmentType.CENTER, spacing: { before: 80, after: 80 },
}),
new Paragraph({
children: [new TextRun({ text: 'A Triple-Complexity Case | CARE Guidelines | July 2026', size: 20, color: '808080' })],
alignment: AlignmentType.CENTER, spacing: { before: 60, after: 400 },
}),
/* ── WHY THIS CASE ─────────────────────────────────────────────── */
h1('Why This Case Is Highly Conference-Worthy'),
para('This case carries three layers of clinical complexity that make it exceptionally suitable for conference presentation:'),
spacer(),
multiColTable(
['Factor', 'Clinical Significance', 'Educational Value'],
[
['Isolated Hepatic TB', 'No pulmonary or extra-hepatic TB — accounts for <1% of all TB cases', 'Rare entity; imaging mimics malignancy and hydatid disease'],
['Type 2 Diabetes (T2DM)', 'DM increases TB susceptibility 3-fold; impairs macrophage and neutrophil function; dysregulates cytokine signalling (Saula et al., Front Immunol 2026)', 'Explains unusual susceptibility in a "non-classic" immunocompromised host'],
['MASLD / CLD', 'MASLD is the most common chronic liver disease (>30% adult prevalence by 2030); background hepatic fibrosis amplifies ATT hepatotoxicity risk and complicates LFT interpretation', 'ATT use in a diseased liver is a genuine management dilemma'],
['Combined triple comorbidity', 'No published case series specifically describes isolated hepatic TB occurring on a background of T2DM + MASLD-CLD together', 'Potentially the first or one of very few such reports in the literature'],
]
),
spacer(),
noteBox('KEY POINT: The rarity of isolated hepatic TB alone makes a case reportable. The simultaneous presence of T2DM and MASLD-CLD elevates this to a triple-complexity case — a genuinely novel contribution.'),
spacer(),
/* ══ SECTION 1 — TITLE ═══════════════════════════════════════════ */
h1('Section 1: Title'),
para('A strong title signals the diagnostic dilemma AND names all three conditions. Aim for under 20 words.'),
spacer(),
para([bold('Suggested titles:')]),
bullet('"Isolated Hepatic Tuberculosis Unmasked in a Patient with Type 2 Diabetes and MASLD Chronic Liver Disease: A Triple Diagnostic and Therapeutic Challenge"'),
bullet('"Focal Liver Lesions in a Diabetic Patient with Metabolic Liver Disease — When Tuberculosis Mimics Malignancy"'),
bullet('"Isolated Hepatic Tuberculosis in T2DM with MASLD-CLD: Navigating Anti-Tubercular Therapy in a Compromised Liver"'),
spacer(),
para([bold('Title rules:')]),
bullet('Name the final diagnosis (Isolated Hepatic Tuberculosis)'),
bullet('Mention the host complexity (T2DM, MASLD/CLD)'),
bullet('Signal the challenge (diagnostic dilemma, therapeutic conundrum, or rare complication)'),
bullet('Avoid vague openers like "A rare case of..." or "An unusual presentation of..."'),
spacer(),
/* ══ SECTION 2 — ABSTRACT ════════════════════════════════════════ */
h1('Section 2: Abstract (150–250 words, Structured)'),
twoColTable([
['Sub-section', 'Content to include'],
['Background (2-3 sentences)', 'Isolated hepatic TB is rare even in endemic regions (<1% of TB). T2DM triples TB risk via immune dysregulation (impaired macrophages, altered cytokines). MASLD is the commonest CLD globally; co-existing hepatic fibrosis amplifies ATT hepatotoxicity and obscures LFT interpretation.'],
['Case Presentation (4-6 sentences)', 'Age, sex, known T2DM duration, MASLD-CLD stage. Presenting symptoms (fever, RUQ pain, weight loss, fatigue). Key findings (hepatomegaly, deranged LFTs — cholestatic pattern over baseline MASLD changes). Imaging (focal hepatic lesion — hypoechoic/rim-enhancing on CT, mimicking HCC or metastasis). Diagnosis by USG-guided liver biopsy: caseating granuloma + Langhans giant cells + MTB-PCR positive. ATT regimen used, LFT monitoring plan, and outcome.'],
['Conclusion / Learning Points', '(1) In endemic regions, isolated hepatic TB must be considered in T2DM patients with focal hepatic lesions even on a background of MASLD. (2) Liver biopsy with histopathology + MTB-PCR is the gold standard. (3) ATT in CLD patients requires CTP score-guided regimen modification and intensive LFT monitoring.'],
]),
spacer(),
/* ══ SECTION 3 — INTRODUCTION ════════════════════════════════════ */
h1('Section 3: Introduction (250–350 words)'),
para('Your introduction must establish three things: (a) why TB matters globally, (b) why the liver involvement is unusual, and (c) why this specific host (T2DM + MASLD) makes the case novel.'),
spacer(),
para([bold('Paragraph 1 — TB background:')]),
bullet('TB remains a leading cause of infectious disease mortality worldwide (WHO 2024)'),
bullet('Extra-pulmonary TB accounts for ~20% of all TB cases'),
bullet('Hepatic involvement occurs in up to 50–80% of miliary TB, but isolated hepatic TB (no pulmonary/extra-hepatic focus) represents <1% of cases and poses unique diagnostic challenges'),
spacer(),
para([bold('Paragraph 2 — Host complexity (T2DM):')]),
bullet('T2DM is a well-established risk factor for TB; it increases susceptibility ~3-fold'),
bullet('Hyperglycaemia impairs macrophage phagocytosis, dendritic cell function, neutrophil killing, and adaptive T-cell immunity (Saula et al., Front Immunol 2026 — systematic review of 81 studies)'),
bullet('DM also impairs granuloma formation — the primary containment mechanism for Mtb'),
bullet('The TB-DM comorbidity is a growing public health burden, especially in South Asia and sub-Saharan Africa'),
spacer(),
para([bold('Paragraph 3 — Host complexity (MASLD-CLD):')]),
bullet('MASLD (previously NAFLD) is now the most common CLD globally, defined by hepatic steatosis + at least one cardiometabolic risk factor (Robbins Pathology, 9th ed.)'),
bullet('MASLD in T2DM patients is classified as a high-risk group requiring mandatory hepatic fibrosis evaluation'),
bullet('When active liver disease is present, all four first-line ATT drugs pose hepatotoxicity risk — creating a management dilemma'),
bullet('Rifampicin and isoniazid induce hepatic cytochrome P-450 enzymes, potentially accelerating drug-induced injury in a fibrotic liver (Robbins Pathology)'),
spacer(),
para([bold('Closing sentence:')]),
centreItalic('"We report a rare case of isolated hepatic tuberculosis occurring on a background of Type 2 Diabetes Mellitus and MASLD-related Chronic Liver Disease, highlighting the diagnostic challenges, the role of liver biopsy, and the complexities of anti-tubercular therapy in a metabolically compromised host."'),
spacer(),
para('Cite 5–8 references here (see Section 8 for suggested references).'),
spacer(),
/* ══ SECTION 4 — CASE PRESENTATION ══════════════════════════════ */
h1('Section 4: Case Presentation (The Core — Write Chronologically)'),
/* 4a */
h2('4a. Patient Demographics and Chief Complaint'),
twoColTable([
['Element', 'What to document'],
['Age and sex', 'Middle-aged or older adult (T2DM + MASLD more prevalent >40 years)'],
['Occupation / origin', 'Note if from TB-endemic region or urban slum setting'],
['Duration of T2DM', 'How long known diabetic; current medication (metformin, insulin, etc.)'],
['MASLD/CLD stage', 'Known MASLD diagnosis? Ultrasound-proven? Biopsy-proven fibrosis stage (F0–F4)?'],
['Chief complaint', 'Fever (duration), RUQ/epigastric pain, weight loss, anorexia, fatigue, jaundice'],
['Duration before presentation', 'Subacute course (weeks-months) is typical for TB vs. acute for abscess'],
]),
spacer(),
/* 4b */
h2('4b. Past Medical History and Risk Factors'),
bullet('Type 2 Diabetes Mellitus: duration, glycaemic control (HbA1c level — poorly controlled T2DM = higher TB risk)'),
bullet('MASLD / CLD: stage of fibrosis (FIB-4 index, LSM by FibroScan, or liver biopsy), presence of cirrhosis (CTP class A/B/C)'),
bullet('Hypertension, dyslipidaemia — common MASLD comorbidities'),
bullet('No alcohol use — required for MASLD diagnosis (excludes alcohol-associated liver disease)'),
bullet('TB contact history, previous TB, or latent TB treatment'),
bullet('BCG vaccination status'),
bullet('HIV status — negative (this makes the case more unusual; TB in HIV-negative T2DM + MASLD is rarer)'),
bullet('No prior immunosuppressive therapy'),
spacer(),
infoBox('MASLD DIAGNOSIS NOTE: Under the 2023 nomenclature (Rinella et al., J Hepatol 2023), MASLD requires hepatic steatosis on imaging/histology + at least one of: BMI ≥25 kg/m², T2DM, hypertension, dyslipidaemia, or waist circumference criteria. Your patient with T2DM automatically qualifies.'),
spacer(),
/* 4c */
h2('4c. Physical Examination'),
twoColTable([
['System', 'Expected / notable findings'],
['General', 'Febrile, cachexic, pallor'],
['Abdomen', 'Hepatomegaly (tender, X cm below right costal margin); possible mild splenomegaly; no signs of portal hypertension (or if present, document ascites, caput medusae, splenomegaly)'],
['Respiratory', 'CLEAR chest — absence of respiratory signs is the defining feature of "isolated" hepatic TB'],
['Lymph nodes', 'No peripheral lymphadenopathy (further supports isolated hepatic involvement)'],
['Metabolic signs', 'Acanthosis nigricans (DM), obesity/central adiposity (MASLD)'],
]),
spacer(),
/* 4d */
h2('4d. Investigations — Present in Logical Sequence'),
h3('Baseline Haematology and Biochemistry'),
multiColTable(
['Test', 'Expected finding in this case', 'Why important'],
[
['CBC', 'Normocytic anaemia, elevated ESR/CRP, leukocytosis', 'Systemic inflammation; anaemia of chronic disease'],
['LFTs', 'Cholestatic or mixed pattern: elevated ALP, GGT; bilirubin raised; AST/ALT mildly elevated', 'In MASLD, baseline LFTs may already be abnormal — the new cholestatic shift is the key change'],
['Serum albumin', 'Low (reflects nutritional status and CLD)', 'Low albumin = reduced ATT drug binding; affects dosing'],
['Serum bilirubin', 'Raised (direct > indirect)', 'Guides CTP score if cirrhosis present'],
['PT/INR', 'May be prolonged in advanced CLD', 'Critical for CTP scoring and ATT safety'],
['HbA1c', 'Likely >8% (poorly controlled T2DM)', 'Quantifies immunosuppression from hyperglycaemia'],
['Fasting lipid profile', 'Dyslipidaemia (raised triglycerides, low HDL)', 'Confirms metabolic syndrome supporting MASLD diagnosis'],
['FIB-4 index', 'Calculate: (Age × AST) / (Platelets × √ALT)', 'Non-invasive fibrosis marker; FIB-4 >3.25 = advanced fibrosis risk (note: less accurate in T2DM >65 years)'],
]
),
spacer(),
h3('Microbiological Workup'),
bullet('Sputum AFB smear × 3 (on 3 consecutive days) — NEGATIVE, confirming no pulmonary involvement'),
bullet('Sputum culture for Mycobacterium tuberculosis — NEGATIVE'),
bullet('IGRA (QuantiFERON-TB Gold In-Tube) or Mantoux tuberculin skin test — document result'),
bullet('Blood cultures (aerobic, anaerobic, and mycobacterial) — NEGATIVE'),
spacer(),
h3('Serology and Tumour Markers'),
bullet('HIV 1 & 2 — NEGATIVE (crucial to establish non-immunocompromised baseline)'),
bullet('HBsAg, Anti-HCV — NEGATIVE (rules out viral hepatitis as cause of liver lesion/LFT derangement)'),
bullet('Hydatid serology — Echinococcus IgG NEGATIVE (key differential)'),
bullet('AFP — Normal (excludes HCC as primary diagnosis; in MASLD-CLD, AFP can be mildly elevated — document the level)'),
bullet('CEA, CA 19-9 — Normal (excludes colorectal metastases and cholangiocarcinoma)'),
bullet('ANA, AMA, ASMA — Negative (excludes autoimmune hepatitis and PBC)'),
spacer(),
h3('Imaging'),
multiColTable(
['Modality', 'Expected Findings', 'Diagnostic Contribution'],
[
['USG abdomen', 'Hepatomegaly; increased echogenicity (background MASLD steatosis); focal hypoechoic/heterogeneous lesion(s); possible perilesional oedema', 'First-line; detects focal lesion; background MASLD echo-pattern visible'],
['CT abdomen with contrast (triphasic)', 'Focal hypo- or heterodense lesion; peripheral rim enhancement in arterial phase (can mimic HCC/metastasis); no primary lesion elsewhere in abdomen or chest', 'Best for lesion characterisation and excluding pulmonary TB (chest CT in same session)'],
['MRI liver (with hepatobiliary contrast)', 'Better soft-tissue resolution; T2-bright core with peripheral enhancement; no satellite lesions or biliary invasion in isolated form', 'Useful if CT inconclusive; best pre-biopsy characterisation'],
['Chest X-ray / CT chest', 'NORMAL — this is the defining finding of "isolated" hepatic TB', 'Documents absence of pulmonary involvement'],
['FibroScan / Elastography', 'Document LSM (kPa) to stage MASLD fibrosis', 'Baseline fibrosis staging before starting hepatotoxic ATT'],
['PET-CT (if available)', 'FDG-avid hepatic lesion mimicking malignancy — a classic diagnostic pitfall', 'Can falsely suggest malignancy; reinforces need for biopsy'],
]
),
spacer(),
h3('Tissue Diagnosis — The Gold Standard'),
noteBox('In a patient with MASLD + T2DM, the temptation is to attribute all liver abnormalities to the metabolic liver disease. The only way to correctly diagnose hepatic TB is liver biopsy. Do NOT defer biopsy.'),
spacer(),
bullet('USG-guided or CT-guided percutaneous liver biopsy from the focal lesion'),
bullet('HISTOPATHOLOGY: Caseating granulomas with central necrosis; epithelioid macrophages; Langhans-type multinucleated giant cells; surrounding lymphocytic cuff. Normal hepatic architecture (hepatocytes, portal tracts) around the granuloma.'),
bullet('ZN (Ziehl-Neelsen) stain for AFB — may be positive or negative (sensitivity ~37%); AFB-positive confirms TB; AFB-negative does not exclude it'),
bullet('MTB-PCR on biopsy specimen — POSITIVE: highly sensitive and specific; provides rapid confirmation when culture is pending (Frameworks for Internal Medicine, Wolters Kluwer, p.190)'),
bullet('Mycobacterial culture (MGIT/liquid medium) — POSITIVE (takes 2–6 weeks; used for drug sensitivity testing)'),
bullet('ALSO note MASLD changes on background liver tissue: macrovesicular steatosis (≥5% hepatocytes), lobular inflammation, ballooned hepatocytes, perisinusoidal fibrosis — document the MASLD activity score and fibrosis stage (F0-F4)'),
spacer(),
/* 4e */
h2('4e. Differential Diagnoses Considered'),
multiColTable(
['Differential', 'Why It Was Considered', 'How It Was Excluded'],
[
['Hepatocellular carcinoma (HCC)', 'MASLD-CLD with focal hepatic lesion; DM is an HCC risk factor; FDG-avid on PET', 'AFP normal; biopsy shows granuloma not tumour cells; no cirrhosis or portal hypertension'],
['MASLD-related focal lesion (focal fat / focal sparing)', 'Background MASLD present', 'Focal fat does not enhance on CT; biopsy diagnostic'],
['Pyogenic liver abscess', 'Fever, RUQ pain, hepatomegaly', 'No acute septic picture; cultures negative; biopsy shows granuloma not pus'],
['Amoebic liver abscess', 'Endemic region; single large lesion', 'Entamoeba serology negative; biopsy not consistent'],
['Hydatid cyst', 'Cystic lesion in endemic region', 'Echinococcus IgG negative; CT morphology non-cystic'],
['Hepatic metastases', 'Multiple lesions on imaging; known DM (colorectal cancer risk)', 'CEA/CA19-9 normal; no primary found; biopsy diagnostic'],
['Sarcoidosis', 'Non-caseating hepatic granulomas', 'Caseating granuloma + MTB-PCR positive; no mediastinal adenopathy'],
['Drug-induced liver injury (DILI)', 'Patient on antidiabetic drugs (metformin)', 'Metformin does not cause granulomas; biopsy diagnostic'],
]
),
spacer(),
/* 4f */
h2('4f. Assessment of CLD Severity Before ATT — Critical Step'),
para([bold('This step is unique to your case and not discussed in simple hepatic TB reports. It must be highlighted.'), plain(' Before starting ATT, formally assess CLD severity:')]),
spacer(),
twoColTable([
['Assessment Tool', 'Relevance in This Case'],
['Child-Turcotte-Pugh (CTP) Score', 'Guides ATT regimen selection. CTP-A: standard ATT possible with monitoring. CTP-B: reduce hepatotoxic drugs. CTP-C: avoid standard ATT; use non-hepatotoxic regimen (streptomycin, ethambutol, fluoroquinolone, amikacin).'],
['MELD Score', 'If decompensated CLD present, high MELD predicts mortality risk from ATT-DILI.'],
['FIB-4 / FibroScan', 'Quantify fibrosis stage pre-treatment — baseline reference for monitoring.'],
['HbA1c', 'Targets <7% during TB treatment; poor glycaemic control worsens TB outcomes (TB also worsens glycaemic control — mutual amplification).'],
['Baseline LFTs', 'Document pre-ATT LFTs carefully — ATT-DILI is defined as >3× ULN in context of normal baseline; in MASLD, the "ULN" is already elevated in many patients.'],
]),
spacer(),
/* 4g */
h2('4g. Treatment — The Most Complex Section'),
noteBox('ATT in a patient with pre-existing MASLD-CLD is a genuine management conundrum (Diggikar et al., Cureus 2024). All first-line drugs (HRZE) carry hepatotoxicity risk. Rifampicin induces CYP450 and can also interact with anti-diabetic drugs.'),
spacer(),
h3('ATT Regimen Selection Based on CTP Score'),
multiColTable(
['CLD Severity', 'Recommended ATT Regimen', 'Notes'],
[
['CTP-A (compensated)', '2HRZE / 4HR — standard regimen with intensive LFT monitoring (weekly for 1 month, then 2-weekly)', 'Most patients with MASLD-CLD will be CTP-A'],
['CTP-B (moderate)', 'Reduce to 2 hepatotoxic drugs: 2HRE / 7HR (no pyrazinamide) OR replace one drug with a fluoroquinolone (levofloxacin/moxifloxacin)', 'Extend total treatment duration to 9 months'],
['CTP-C (decompensated cirrhosis)', 'Non-hepatotoxic regimen: Streptomycin + Ethambutol + Fluoroquinolone + Amikacin for 18-24 months', 'Avoid INH, RIF, PZA; refer to hepatology for liver transplant evaluation'],
]
),
spacer(),
h3('Additional Treatment Considerations'),
bullet('Pyridoxine (Vitamin B6) supplementation: 25-50 mg/day with INH to prevent peripheral neuropathy (especially important in DM patients with baseline neuropathy risk)'),
bullet('Rifampicin-drug interactions: RIF is a potent CYP3A4 inducer — reduces efficacy of sulfonylureas, glipizide, repaglinide; dose adjustment of anti-diabetic drugs may be needed'),
bullet('Metformin: can continue; not affected by RIF; monitor for lactic acidosis if renal function impaired'),
bullet('Glycaemic management: TB infection worsens glycaemic control (islet cell inflammation, cytokine-driven insulin resistance); target HbA1c <7% and increase glucose monitoring frequency during ATT'),
bullet('MASLD-specific: continue lifestyle modification, statin therapy (statins are safe with ATT); avoid alcohol; address obesity'),
bullet('LFT monitoring protocol: baseline → weekly × 4 weeks → biweekly × 2 months → monthly thereafter; stop ATT if ALT >3× ULN with symptoms or >5× ULN asymptomatic'),
spacer(),
h3('If ATT-DILI Occurs (Hepatotoxicity)'),
bullet('Stop all potentially hepatotoxic drugs if ALT >3× ULN with symptoms or >5× ULN asymptomatic'),
bullet('Switch to non-hepatotoxic regimen: ethambutol + streptomycin/amikacin + fluoroquinolone until LFTs recover'),
bullet('Rechallenge sequentially: start rifampicin first (least hepatotoxic of the three), then INH, then PZA — with 3-7 day intervals between each drug'),
bullet('If rechallenge fails, use permanent non-hepatotoxic regimen for 18-24 months'),
spacer(),
/* 4h */
h2('4h. Outcome and Follow-up'),
bullet('Clinical response: fever resolution (typically within 2-4 weeks of ATT)'),
bullet('Weight gain and appetite recovery'),
bullet('Glycaemic control: document HbA1c at 3 and 6 months (TB treatment often temporarily worsens DM control)'),
bullet('LFT trend: document weekly LFT results; note any ATT-DILI episodes and management'),
bullet('Imaging follow-up: repeat USG at 3 months and CT/MRI at 6 months — resolution of hepatic lesion confirms diagnosis retrospectively'),
bullet('MASLD follow-up: repeat FibroScan at 6-12 months — note if ATT worsened or stabilised hepatic fibrosis'),
bullet('Full ATT course completion (6-9 months depending on regimen used)'),
bullet('End of treatment: document cure criteria (clinical, biochemical, radiological resolution)'),
spacer(),
/* ══ SECTION 5 — DISCUSSION ══════════════════════════════════════ */
h1('Section 5: Discussion (500–700 words — Highest Impact Section)'),
para('Structure the discussion into distinct themes. This is where you distinguish your case from others in the literature.'),
spacer(),
h2('Theme 1: The Rarity of the Combination'),
bullet('Isolated hepatic TB alone is extremely rare (<1% of all TB)'),
bullet('The combination with T2DM + MASLD-CLD has not been systematically described'),
bullet('Compare with: Kandasamy 2018 (isolated hepatobiliary TB, no metabolic comorbidities); Azzaza 2020 (isolated hepatic TB mimicking hydatid, no DM); Diggikar 2024 (TB in cirrhosis, but not MASLD-specific)'),
spacer(),
h2('Theme 2: The Role of T2DM in Facilitating Hepatic TB'),
bullet('DM impairs innate immunity: reduced macrophage phagocytosis, neutrophil oxidative burst, dendritic cell antigen presentation (Saula et al., Front Immunol 2026 — systematic review of 81 studies covering immune dysregulation in TB-DM)'),
bullet('DM disrupts granuloma formation — the key containment mechanism for Mycobacterium tuberculosis'),
bullet('Hyperglycaemia-driven immunosuppression allows Mtb dissemination via portal blood to the liver without establishing a pulmonary focus — this may explain the "isolated" hepatic pattern'),
bullet('The reciprocal relationship: TB infection causes islet cell amyloidosis and cytokine-driven insulin resistance, further worsening DM control (Peng, Med Int 2024)'),
spacer(),
h2('Theme 3: MASLD as a Diagnostic Confounder'),
bullet('MASLD itself causes hepatomegaly, elevated ALT/AST, and focal lesions (focal fat / focal sparing) — all of which can mask or mimic hepatic TB'),
bullet('The background cholestatic pattern in MASLD tends to be less pronounced; a new cholestatic shift in a MASLD patient should raise suspicion for a superimposed process'),
bullet('FIB-4 diagnostic accuracy is reduced in T2DM patients >55 years — a limitation that must be acknowledged when staging fibrosis in this population (Han & Jun, Clin Mol Hepatol 2024)'),
spacer(),
h2('Theme 4: The ATT-Hepatotoxicity Dilemma'),
bullet('The irony: drugs used to treat hepatic TB can themselves cause or worsen hepatic injury'),
bullet('Rifampicin, isoniazid, and pyrazinamide are all associated with drug-induced liver injury; in a patient with established hepatic fibrosis (MASLD), the risk of progression to acute liver failure is amplified'),
bullet('Robbins Pathology (9th ed.) notes that rifampicin, phenytoin, isoniazid, and other enzyme-inducing agents may exacerbate the toxicity of other drugs by inducing cytochrome P-450 enzymes'),
bullet('The CTP score-guided approach (as proposed for cirrhosis TB management by Diggikar et al., 2024) is the most rational framework in this clinical scenario'),
bullet('ATT-DILI incidence in pre-existing liver disease is 2-3× higher than in patients with normal liver function'),
spacer(),
h2('Theme 5: Glycaemic Optimisation as Part of TB Treatment'),
bullet('This is a unique teaching point: TB and DM are bidirectional in their relationship'),
bullet('Poorly controlled DM leads to worse TB outcomes (slower sputum conversion, more relapses)'),
bullet('TB infection itself worsens glycaemic control — the inflammatory cytokine environment promotes insulin resistance'),
bullet('Rifampicin reduces plasma levels of sulfonylureas via CYP3A4 induction — anti-diabetic drug doses may need upward adjustment during ATT'),
bullet('Target HbA1c <7% during TB treatment; increase glucose monitoring; involve endocrinology/diabetology co-management'),
spacer(),
h2('Theme 6: Key Learning Points'),
infoBox('Learning Point 1: In TB-endemic regions, isolated hepatic TB must be considered in any T2DM patient with focal hepatic lesions — even when the liver disease appears to be attributable to MASLD.'),
spacer(),
infoBox('Learning Point 2: Liver biopsy with histopathology showing caseating granuloma + Langhans giant cells + MTB-PCR is the gold standard. Do not defer biopsy in the hope that empirical imaging will be diagnostic.'),
spacer(),
infoBox('Learning Point 3: Before starting ATT in a patient with CLD, calculate the CTP score. CTP class guides regimen selection. Intensive LFT monitoring is mandatory throughout treatment.'),
spacer(),
infoBox('Learning Point 4: ATT-DILI is more common in pre-existing liver disease. Have a clear protocol for stopping, bridging with non-hepatotoxic drugs, and sequential rechallenge.'),
spacer(),
infoBox('Learning Point 5: Optimise glycaemic control in parallel. Poor DM control worsens TB outcomes. TB worsens DM control. Both must be actively managed simultaneously.'),
spacer(),
/* ══ SECTION 6 — CONCLUSION ══════════════════════════════════════ */
h1('Section 6: Conclusion (4–5 sentences)'),
centreItalic('"Isolated hepatic tuberculosis in a patient with Type 2 Diabetes Mellitus and MASLD-related Chronic Liver Disease represents a rare but instructive clinical entity. The triple complexity of this case — a rare organ-specific infection occurring in a metabolically immunocompromised host with pre-existing liver disease — creates both diagnostic uncertainty and therapeutic risk. Liver biopsy with caseating granuloma histology and MTB-PCR remains the cornerstone of diagnosis. Anti-tubercular therapy in this setting requires a CTP score-guided regimen, intensive hepatic monitoring, and concurrent optimisation of glycaemic control. Clinicians in endemic regions must maintain a high index of suspicion for hepatic TB in any diabetic patient with focal hepatic lesions, regardless of background metabolic liver disease."'),
spacer(),
/* ══ SECTION 7 — ETHICS ══════════════════════════════════════════ */
h1('Section 7: Patient Consent and Ethics'),
bullet('Written informed consent obtained from the patient for publication of this case report and any accompanying images'),
bullet('Institutional ethical committee approval number (if required): _______________'),
bullet('Patient identity has been anonymised in the manuscript'),
spacer(),
/* ══ SECTION 8 — REFERENCES ══════════════════════════════════════ */
h1('Section 8: References (Vancouver Style)'),
para([bold('Essential references for this case:')]),
spacer(),
para('1. Kandasamy S, Govindarajalou R, Chakkalakkoombil SV, et al. Isolated hepatobiliary tuberculosis: a diagnostic challenge. BMJ Case Rep. 2018. PMID: 29880621'),
para('2. Azzaza M, Farhat W, Ammar H, et al. Isolated hepatic tuberculosis presenting as hydatid cyst. Clin J Gastroenterol. 2020. PMID: 31758483'),
para('3. Diggikar PM, Reddy HR, Mundada M, et al. Tuberculosis in a liver cirrhosis patient: a management conundrum. Cureus. 2024. PMID: 38445150'),
para('4. Saula AY, Cevik M, Cliff JM, et al. Immune dysregulation in tuberculosis-diabetes comorbidity: mechanistic and translational insights. Front Immunol. 2026. PMID: 42112381'),
para('5. Peng YF. Pulmonary tuberculosis and diabetes mellitus: epidemiology, pathogenesis and therapeutic management. Med Int (Lond). 2024. PMID: 38204892'),
para('6. Rinella ME, Lazarus JV, Ratziu V, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79:1542-56.'),
para('7. Trifonov P, Dragneva SS, Todovichin DK. Liver cirrhosis and tuberculosis: double impact of active tuberculosis and ATT causing acute liver injury. Am J Case Rep. 2026. PMID: 42415389'),
para('8. Jayakumar J. Isolated hepatic tuberculosis. Kathmandu Univ Med J. 2008. PMID: 20071827'),
para('9. Kumar V, Pandey D. Isolated hepatosplenic tuberculosis. Hepatobiliary Pancreat Dis Int. 2008. PMID: 18522893'),
para('10. Robbins, Cotran & Kumar. Pathologic Basis of Disease, 10th ed. Philadelphia: Elsevier; 2024. Chapter 18 (MASLD, Drug-Induced Liver Injury).'),
para('11. Han JW, Jun DW. FIB-4 diagnostic performance in T2DM patients with MASLD. Clin Mol Hepatol. 2024.'),
para('12. WHO. Global Tuberculosis Report. Geneva: WHO; 2024.'),
spacer(),
/* ══ SECTION 9 — CONFERENCE TIPS ════════════════════════════════ */
h1('Section 9: Conference Presentation Tips'),
h2('Poster Presentation'),
bullet('Column layout: Left = Introduction + Case Summary | Centre = Images (USG, CT, Histology) + Investigation Table | Right = Discussion + Conclusion + References'),
bullet('Critical visuals to include: (1) CT liver showing focal lesion, (2) Liver biopsy histology showing caseating granuloma with Langhans giant cell, (3) Timeline figure showing symptom onset → investigations → diagnosis → treatment → resolution'),
bullet('Include a "Metabolic Context" box: BMI, HbA1c, FIB-4, CTP score — this summarises the host complexity at a glance'),
bullet('Include a "LFT Monitoring Timeline" table: pre-ATT baseline → weekly values during treatment'),
bullet('Minimum font: 24pt body, 36pt headings'),
spacer(),
h2('Oral Presentation (8–10 minutes)'),
twoColTable([
['Slide', 'Content'],
['Slide 1', 'Title, authors, institution, conflict of interest declaration'],
['Slide 2', 'Background: TB epidemiology + why T2DM + MASLD make this special (3 bullet points per condition)'],
['Slide 3', 'Case: Patient demographics, symptoms, metabolic history (T2DM duration, HbA1c, MASLD stage)'],
['Slide 4', 'Examination and investigations — use a clean table; highlight the cholestatic LFT pattern on background MASLD'],
['Slide 5', 'Imaging: Show CT liver image + chest CT (normal) side by side'],
['Slide 6', 'Histopathology image of caseating granuloma with Langhans giant cells — this is the money slide'],
['Slide 7', 'Differential diagnosis table'],
['Slide 8', 'Treatment: CTP score calculation → regimen chosen → LFT monitoring chart'],
['Slide 9', 'Outcome: LFT normalisation trend + imaging resolution at 6 months'],
['Slide 10', 'Discussion + Learning Points (5 key takeaways in bold)'],
['Slide 11', 'Conclusion + References (top 5 only)'],
]),
spacer(),
/* ── FOOTER ─────────────────────────────────────────────────────── */
new Paragraph({
children: [new TextRun({ text: 'Sources: Robbins Pathology 10th ed. | Frameworks for Internal Medicine (Wolters Kluwer) | PubMed literature (2018-2026) | CARE Guidelines | WHO TB Report 2024 | Prepared July 2026', size: 17, color: '808080', italics: true })],
alignment: AlignmentType.CENTER,
spacing: { before: 400, after: 60 },
border: { top: { style: BorderStyle.SINGLE, size: 2, color: 'CCCCCC' } },
}),
],
}],
});
Packer.toBuffer(doc).then(buf => {
fs.writeFileSync('/home/daytona/workspace/hepatic-tb-case-report/Isolated_Hepatic_TB_T2DM_MASLD_Case_Report_Guide.docx', buf);
console.log('Done.');
});
Failed to create session: unauthorized: authentication failed: Bearer token is invalid
We encountered an error while processing your request. Please try again or reach out to us for help.