Ne0hritic vs nephritic syndrome
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Excellent - I now have comprehensive data from multiple authoritative sources. Here is the full comparison:
Nephrotic Syndrome vs. Nephritic Syndrome
These are the two cardinal presentations of glomerular disease. The distinction is fundamental: nephrotic reflects a permeability failure (protein leaks out), while nephritic reflects inflammation (cells and blood leak in).
Core Pathophysiology
Nephrotic Syndrome
The glomerular capillary wall - composed of endothelium, GBM, and podocytes - acts as both a size and charge barrier. In nephrotic syndrome, structural or physicochemical alterations in this barrier increase permeability to plasma proteins. The key proteins lost are albumin, immunoglobulins, antithrombin III, and lipid-binding proteins. Podocyte injury (foot process effacement) is the common final pathway regardless of the underlying cause.
Cascade of consequences:
- Massive proteinuria (≥3.5 g/day in adults; >50 mg/kg/day in children) → hypoalbuminemia (albumin <3 g/dL)
- Hypoalbuminemia → reduced plasma oncotic pressure → fluid shifts into the interstitium → edema
- Compensatory hepatic lipoprotein synthesis ↑ + reduced lipid catabolism → hyperlipidemia → lipiduria (oval fat bodies in urine)
- Loss of immunoglobulins → susceptibility to infection (especially pneumococcal, staphylococcal)
- Loss of antithrombin III + protein C/S → hypercoagulable state → renal vein thrombosis (especially in membranous nephropathy)
Two edema subtypes:
- Underfill (classic, e.g., minimal change disease): low plasma volume → activated RAAS, elevated aldosterone/ADH, low ANP → sodium retention
- Overfill (other causes): primary renal sodium retention → expanded plasma volume, suppressed RAAS
Nephritic Syndrome
Nephritic syndrome results from glomerular inflammation - proliferation of glomerular cells + infiltration of leukocytes. This inflammatory reaction damages capillary walls, permitting blood to enter the urine, and reduces GFR by reducing the filtering surface area. The reduced GFR leads to oliguria, fluid/sodium retention, and renin release from ischemic kidneys.
Clinical & Lab Features - Head to Head
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Onset | Insidious | Abrupt |
| Mechanism | Increased GBM permeability | Glomerular inflammation |
| Proteinuria | Massive (>3.5 g/day) | Mild-moderate (<3.5 g/day) |
| Hematuria | Absent or microscopic | Prominent (gross or microscopic) |
| RBC casts | Absent | Present (pathognomonic) |
| Serum albumin | Low (<3 g/dL) | Normal or slightly reduced |
| Edema | Severe, soft, pitting, periorbital | Mild-moderate |
| Blood pressure | Normal | Raised (hypertension) |
| JVP | Normal/low | Raised |
| GFR/azotemia | Usually preserved initially | Reduced, oliguria, azotemia |
| Urine color | Frothy (protein) | Smoky/brown (blood) |
| Lipids | Hyperlipidemia + lipiduria | Normal |
| Complement | Usually normal (except MPGN) | Often low (C3 low in PSAGN) |
Urinary Findings
| Finding | Nephrotic | Nephritic |
|---|---|---|
| Protein | +++++ | ++ |
| RBCs | Rare | +++ |
| RBC casts | No | Yes |
| WBCs | No | Possible |
| Oval fat bodies | Yes (lipiduria) | No |
| Fatty casts | Yes | No |
Causes
Nephrotic Syndrome Causes (Robbins 9e)
Primary (children vs. adults):
| Disease | Children | Adults |
|---|---|---|
| Minimal change disease (MCD) | 75% | 8% |
| Focal segmental glomerulosclerosis (FSGS) | 10% | 35% |
| Membranous nephropathy | 3% | 30% |
| MPGN | 10% | 10% |
Secondary (systemic diseases):
- Diabetes mellitus (most common worldwide)
- Amyloidosis
- Systemic lupus erythematosus (class V lupus nephritis)
- Drugs (NSAIDs, gold, penicillamine, heroin)
- Infections (hepatitis B, HIV, malaria)
Nephritic Syndrome Causes
| Disease | Key Feature |
|---|---|
| Post-streptococcal GN (PSAGN) | Latency 1-4 wks; subepithelial "humps" on EM; ↓C3 |
| IgA nephropathy (Berger's) | Episodic hematuria with URI; mesangial IgA deposits |
| Lupus nephritis (class III/IV) | Anti-dsDNA, ↓C3/C4 |
| ANCA-associated vasculitis (GPA, MPA) | pANCA/cANCA positive; pauci-immune |
| Anti-GBM disease (Goodpasture's) | Linear IgG on IF; pulmonary hemorrhage |
| MPGN | Can present as either nephrotic or nephritic; ↓C3 |
Rapidly Progressive GN (RPGN) - The Nephritic Emergency
When nephritic syndrome progresses to kidney failure over days to weeks, this is RPGN. The histologic hallmark is crescents - proliferation of parietal epithelial cells in Bowman's space due to GBM breaks and fibrin leakage. Three immunologic types:
| Type | Mechanism | IF Pattern | Serology |
|---|---|---|---|
| Type I | Anti-GBM antibodies | Linear IgG | Anti-GBM Ab |
| Type II | Immune complex | Granular ("lumpy-bumpy") | Varies (ANA, ASOT, ↓C3) |
| Type III | Pauci-immune (ANCA) | Negative / trace | ANCA positive |
Edema Mechanism Comparison
Nephrotic underfill vs. overfill:
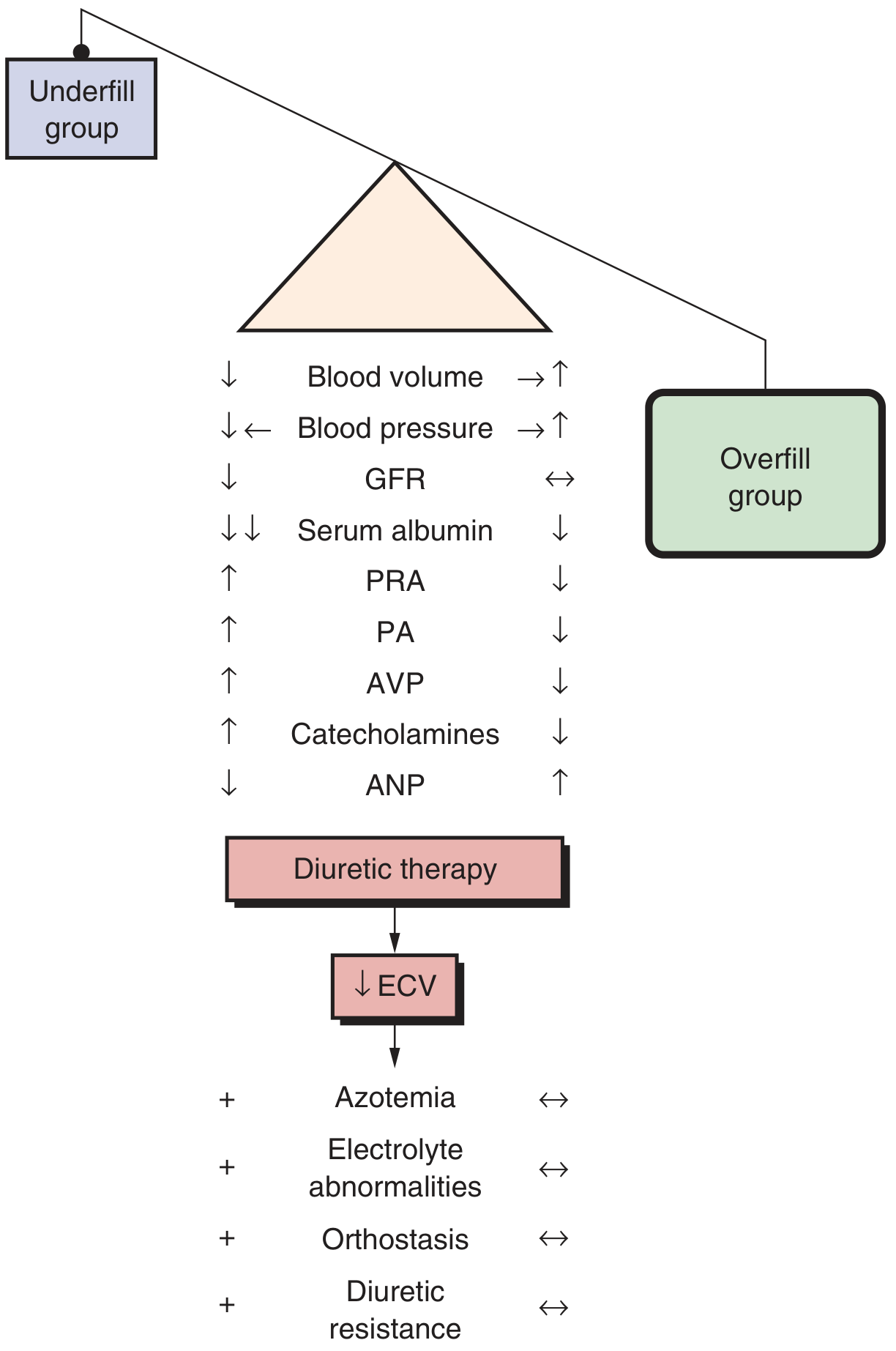
In the underfill group (typical of minimal change disease): low serum albumin → low oncotic pressure → contracted plasma volume → RAAS activation, elevated aldosterone, AVP, catecholamines, low ANP.
In the overfill group: primary renal sodium retention → expanded plasma volume → suppressed RAAS, low aldosterone. Diuretics in the underfill group risk azotemia and orthostasis; in the overfill group they work safely.
Key Memory Anchors
| Clue | Think |
|---|---|
| Frothy urine, periorbital puffiness, no hematuria | Nephrotic |
| Cola/tea-colored urine, hypertension, oliguria | Nephritic |
| Child with MCD | Nephrotic, steroid-responsive |
| Diabetic for 10+ years with proteinuria | Secondary nephrotic |
| Post-sore throat hematuria in child, ↓C3 | Post-streptococcal (nephritic) |
| Recurrent hematuria with upper respiratory infections | IgA nephropathy (nephritic) |
| Hemoptysis + hematuria, anti-GBM+ | Goodpasture's (nephritic/RPGN) |
| Rapidly deteriorating kidney function with crescents | RPGN |
| Can present as EITHER | MPGN |
Note: Some diseases - especially MPGN and lupus nephritis - blur the boundary and can present with mixed features of both syndromes simultaneously.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, 10e; Comprehensive Clinical Nephrology, 7e; Brenner and Rector's The Kidney, 2-Volume Set.
Create a clinical decision tree to differentiate these syndromes
Running Command
Running Command
Writing File
Running Command
Running Command
Running Command
Reading File
Editing File
Writing File
Running Command
Reading File
Running Command
Running Command
Running Command
Reading File
Running Command
Your clinical decision tree is ready:
Nephro Decision Tree
PDF Document · PDF
Here's what the tree covers, step by step:
Entry point: Patient with suspected glomerular disease
Branch 1 - Proteinuria ≥ 3.5 g/day?
- YES → Nephrotic pathway (green)
- NO / sub-nephrotic → Nephritic pathway (red)
Nephrotic branch (left, green):
- RBC casts / gross hematuria? → YES = mixed features (MPGN / Lupus, purple)
- Albumin < 3 g/dL + hyperlipidemia? → NO = re-evaluate orthostatic/overflow proteinuria
- C3 low / MPGN pattern? → YES = MPGN / Dense Deposit Disease
- Age split: Children (<16) → MCD 75%, FSGS 10% | Adults → FSGS 35%, Membranous 30%
Nephritic branch (right, red):
- Hematuria + azotemia? → NO = non-glomerular, further workup
- Hypertension + ↓GFR / oliguria? → NO = mild nephritic (IgA / thin GBM)
- Cr doubles in < 3 months? → NO = Classic nephritic (Post-strep GN, IgA, Lupus III/IV, ANCA)
- YES → RPGN / Crescentic GN (orange), split into:
- Type I: Anti-GBM (Goodpasture) - linear IgG
- Type II: Immune complex - granular IF, ↓C3/C4
- Type III: Pauci-immune (ANCA) - negative IF
Footer bar: Nephrotic complications vs. Nephritic complications side by side.
Gonadal hormones drugs pharmacology and medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from Goodman & Gilman's across all major drug classes. Let me compile the full answer:
Gonadal Hormones: Drugs, Pharmacology & Medicine
(Based on Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14e)
Overview: The HPG Axis - Pharmacological Control Points
The hypothalamic-pituitary-gonadal (HPG) axis provides multiple drug targets:
Hypothalamus → GnRH (pulsatile)
↓
Anterior pituitary → FSH + LH
↓
Gonads → Estradiol / Progesterone / Testosterone
↓
Target tissues (ER / PR / AR)
↓ (negative feedback)
Drugs act at every level: GnRH analogues, gonadotropins, sex steroid agonists/antagonists, receptor modulators, and enzyme inhibitors.
I. ESTROGENS
Chemistry & Classification
| Class | Examples |
|---|---|
| Steroidal (natural) | Estradiol (17β-estradiol), estrone, estriol |
| Steroidal (synthetic) | Ethinyl estradiol, mestranol, estradiol valerate/cypionate |
| Nonsteroidal synthetic | Diethylstilbestrol (DES) |
| Conjugated equine estrogens (CEE) | Premarin - mixture of sulfated estrogens |
Mechanism of Action
Estrogens act via two nuclear receptors - ERα and ERβ - which function as ligand-activated transcription factors. The ER-ligand complex dimerizes, binds estrogen response elements (EREs) in gene promoters, and recruits co-activators/co-repressors. Non-genomic signaling also occurs via membrane-associated ERs (rapid effects on ion channels, kinase cascades).
Pharmacokinetics
- Oral estradiol undergoes extensive first-pass hepatic metabolism → converted to estrone and estrone sulfate
- Ethinyl estradiol: synthetic, highly resistant to first-pass metabolism → far more potent orally than natural estradiol
- 0.625 mg conjugated estrogens ≈ 5-10 μg ethinyl estradiol (in terms of oral potency)
- Routes: oral, transdermal patch/gel, vaginal ring/cream, IM injection (esters)
- Transdermal avoids first-pass effect → lower hepatic impact on clotting factors and SHBG
Physiological Effects
- Secondary sexual development in females (puberty)
- Endometrial proliferation (→ requires progestin opposition to prevent hyperplasia/cancer)
- Bone: inhibits osteoclast activity → maintains bone mineral density
- Cardiovascular: favorable lipid profile (↑HDL, ↓LDL); complex vascular effects
- CNS: influences thermoregulation (hot flashes when deficient), mood, cognition
- Liver: stimulates synthesis of clotting factors, SHBG, angiotensinogen, triglycerides
Therapeutic Uses
1. Menopausal Hormone Therapy (MHT)
- Vasomotor symptoms (hot flashes, sweats) - most efficacious treatment
- Urogenital atrophy (vaginal dryness, dyspareunia)
- Osteoporosis prevention (reduces fracture risk)
- Women with intact uterus: must add progestin to prevent endometrial cancer
- Women post-hysterectomy: estrogen alone is appropriate
- Principle: minimum effective dose for shortest necessary duration
2. Oral Contraceptives (see Section IV below)
3. Female hypogonadism - primary ovarian insufficiency, Turner syndrome
4. Transgender hormone therapy (male-to-female)
Adverse Effects
- Thromboembolism (DVT, PE) - oral > transdermal; related to hepatic effect on clotting factors
- Endometrial cancer (unopposed estrogen)
- Breast cancer (long-term combination MHT - WHI trial data)
- Migraine exacerbation
- Nausea, fluid retention
- Hypertriglyceridemia (oral route)
- Contraindicated in: active thromboembolism, hormone-sensitive cancers, unexplained vaginal bleeding, active liver disease, pregnancy
II. PROGESTINS (Progestogens)
Classification
| Class | Key Drugs | Notes |
|---|---|---|
| Pregnanes | Progesterone (natural), MPA (medroxyprogesterone acetate), dydrogesterone | Progesterone has rapid first-pass metabolism; micronized form available |
| Estranes (19-nortestosterone) | Norethindrone, norethynodrel | Some androgenic activity |
| Gonanes (19-nortestosterone) | Levonorgestrel, norgestrel, norgestimate, desogestrel | Progestational; components of contraceptives |
| Spirolactone-derived | Drospirenone | Antimineralocorticoid activity; used in OCs |
| Antiprogestins/modulators | Mifepristone, ulipristal | See below |
Mechanism of Action
Bind progesterone receptors (PR-A and PR-B) → nuclear transcription regulation. Oppose estrogen-driven endometrial proliferation → converts proliferative to secretory endometrium. In sufficient doses, suppress LH surge → prevent ovulation.
Key Uses
- MHT - endometrial protection (any woman with a uterus on estrogen must have progestin added)
- Contraception (oral, injectable, implant, IUD, emergency)
- Assisted reproductive technology (luteal phase support)
- Endometriosis (depot MPA suppresses menstruation/lesions)
- Dysfunctional uterine bleeding
- Threatened/habitual abortion (progesterone support)
Key Drugs in Detail
Medroxyprogesterone acetate (MPA / Depo-Provera)
- Depot IM injection (150 mg every 3 months) - highly effective contraceptive
- Suppresses ovarian function → amenorrhea common
- Caution: delayed return of fertility (6-18 months); transient bone mineral density loss
Levonorgestrel
- Emergency contraception (Plan B): 1.5 mg within 72 h of unprotected sex
- Progestin-only pill ("mini-pill")
- IUD (Mirena): local uterine delivery, minimal systemic absorption
Micronized progesterone (Prometrium)
- Bioidentical; preferred by many over synthetic progestins for MHT
- Oral or vaginal; better tolerated (less androgenic/glucocorticoid effects)
Mifepristone (RU-486)
- Competitive antagonist at both PR isoforms (also anti-glucocorticoid at high doses)
- Medical abortion: combined with misoprostol (PGE1 analogue) for termination up to 10 weeks
- Also used for Cushing's syndrome (mifepristone blocks glucocorticoid receptor)
Ulipristal Acetate
- Partial PR agonist/antagonist
- Emergency contraception up to 120 h (5 days) post-intercourse - more effective than levonorgestrel, especially days 3-5
III. ANDROGENS
Physiology
- Testosterone is the principal androgen in both men and women
- Men: produced by Leydig cells (LH-stimulated); ~7 mg/day
- Women: corpus luteum + adrenal cortex; ~0.25 mg/day
- Precursors: androstenedione, DHEA (weak androgens, converted peripherally)
- Dihydrotestosterone (DHT): formed by 5α-reductase in prostate, skin, hair follicles - more potent at AR; responsible for prostate growth, male-pattern baldness
- Aromatization: testosterone → estradiol (via aromatase, in adipose/brain/bone)
Testosterone Across the Life Cycle
| Stage | Level | Significance |
|---|---|---|
| 1st trimester fetus | ~250 ng/dL | Male sexual differentiation (Wolffian duct development, external genitalia) |
| Birth | ~250 ng/dL | Brief postnatal surge |
| 2-3 months postnatal | ~250 ng/dL | "Minipuberty" |
| Childhood | <50 ng/dL | Minimal |
| Puberty (12-17 yrs) | Rising to adult levels | External genitalia growth, muscle, bone, voice, sexual hair, spermatogenesis |
| Adult male | 300-1000 ng/dL | Maintained by HPG axis |
| Postpuberty deficiency | Variable | Libido ↓ (weeks), Hgb ↓ (months), bone density ↓ (1 yr), muscle loss (years) |
Therapeutic Androgen Preparations
| Preparation | Route | Details |
|---|---|---|
| Testosterone enanthate / cypionate | Deep IM injection q 1-2 weeks | Formulated in oil; wide serum fluctuations → mood/libido swings |
| Testosterone undecanoate | IM q 10-14 weeks or oral | Long-acting IM; oral form bypasses first-pass via lymphatics |
| Testosterone gel/solution (1-2%) | Transdermal daily | Stable levels; risk of transfer to others via skin contact |
| Testosterone patch | Transdermal daily | Skin irritation common |
| Buccal testosterone | Buccal mucosa twice daily | Avoids first-pass; gum irritation |
| Alkylated androgens (methyltestosterone, oxandrolone) | Oral | 17α-alkylated - resist first-pass but hepatotoxic (peliosis hepatis, cholestasis) |
| Nandrolone decanoate | IM | Anabolic with lower androgenic ratio |
Oral testosterone itself is ineffective due to rapid hepatic catabolism. Preparations are designed to bypass this.
Therapeutic Uses of Androgens
- Male hypogonadism (primary or secondary) - restore virilization, sexual function, energy, bone density, mood
- Delayed puberty in boys - short course to initiate puberty
- Female hypogonadism / low libido - low-dose supplementation
- Wasting/catabolic states - HIV wasting, burns, major surgery (anabolic effect)
- Aplastic anemia - stimulate erythropoiesis
- Hereditary angioedema - anabolic androgens increase C1-inhibitor synthesis
Adverse Effects of Androgens
- Virilization in women (acne, hirsutism, clitoromegaly, voice deepening)
- Polycythemia (↑ EPO secretion)
- Dyslipidemia (↓HDL, ↑LDL)
- Suppression of spermatogenesis (negative HPG feedback → male contraceptive research)
- Hepatotoxicity (17α-alkylated compounds)
- Acne, oily skin
- Prostatic growth (contraindicated in prostate cancer)
- Premature epiphyseal closure if used in adolescents
- Cardiovascular events (↑ RBC viscosity, dyslipidemia)
Selective Androgen Receptor Modulators (SARMs)
Tissue-selective AR agonists designed to maximize anabolic effects (muscle, bone) while minimizing androgenic effects (prostate, scalp). Currently investigational (enobosarm/ostarine most studied); none yet approved.
IV. ORAL CONTRACEPTIVES
Combined Oral Contraceptives (COCs)
Mechanism of contraceptive action (multiple):
- Inhibition of LH surge → prevent ovulation (primary mechanism)
- Altered cervical mucus → impairs sperm penetration
- Altered endometrial receptivity → prevents implantation
- Altered tubal motility
Components:
- Estrogen: ethinyl estradiol (20-35 µg/day in modern pills); or estradiol valerate/estetrol in newer formulations
- Progestin: varies by generation
| Generation | Progestins | Notes |
|---|---|---|
| 1st | Norethindrone, norethynodrel | Moderate androgenic activity |
| 2nd | Levonorgestrel, norgestrel | Standard; lower VTE risk vs. 3rd/4th gen |
| 3rd | Desogestrel, gestodene, norgestimate | Less androgenic; slightly higher VTE risk vs. 2nd gen |
| 4th | Drospirenone, dienogest | Antimineralocorticoid (drospirenone); anti-androgenic; used in PCOS, acne |
Formulations:
- Monophasic: fixed estrogen + progestin dose throughout cycle
- Biphasic/triphasic: varying doses to mimic natural cycle (theoretical advantage unproven)
- Extended cycle / continuous (e.g., Seasonale): 84 active pills + 7 placebo → 4 periods/year
- Progestin-only pill ("mini-pill"): no estrogen; mechanism mainly cervical mucus + endometrium; must be taken at precise same time daily
Non-contraceptive benefits of COCs:
- Dysmenorrhea relief
- Management of endometriosis
- PCOS (cycle regulation, acne, hirsutism)
- PMS/PMDD (drospirenone-containing)
- Iron-deficiency anemia (reduced menstrual blood loss)
- Reduced risk of ovarian and endometrial cancer
- Acne treatment (anti-androgenic progestins)
Risks and Contraindications (WHO MEC):
- VTE (absolute contraindication in history of DVT/PE; risk ×3-4 with COCs)
- Arterial events: stroke, MI (risk highest with smoking + age >35)
- Hypertension (can worsen; estrogen raises angiotensinogen)
- Breast cancer (modest increased risk with current use)
- Liver disease / hepatic adenoma
- Migraine with aura (contraindication - ischemic stroke risk)
- Absolute contraindications: smoking >35 yrs + age >35, active VTE, stroke/MI history, hormone-sensitive cancer, active liver disease, unexplained vaginal bleeding
V. GnRH ANALOGUES
GnRH Agonists (Paradoxically Suppress Gonadal Function)
Continuous (non-pulsatile) GnRH receptor stimulation → receptor downregulation → suppressed FSH/LH → medical castration
| Drug | Route |
|---|---|
| Leuprolide (leuprorelin) | SC/IM depot (monthly, 3-monthly, 6-monthly) |
| Goserelin | SC implant |
| Buserelin, nafarelin | Intranasal |
| Triptorelin | IM depot |
Initial "flare" effect: first 1-2 weeks → transient ↑ in FSH/LH/testosterone (important in prostate cancer - can worsen bone pain temporarily; cover with antiandrogen)
After 1-3 weeks: pituitary downregulation → sustained hypogonadotropic hypogonadal state
Uses:
- Prostate cancer (androgen deprivation therapy)
- Endometriosis
- Uterine fibroids (leiomyomas)
- Precocious puberty
- Controlled ovarian hyperstimulation (IVF protocols) - used with gonadotropins to prevent premature LH surge
- Breast cancer (premenopausal ER+ - ovarian suppression)
- Menstrual suppression (thrombocytopenia, transsexual transitioning)
Long-term side effects: hot flashes, osteoporosis (add bisphosphonate ± add-back therapy), sexual dysfunction, fatigue, cognitive effects
GnRH Antagonists (Immediate Suppression - No Flare)
Competitive receptor antagonists → immediate ↓ FSH/LH (no flare effect)
| Drug | Use |
|---|---|
| Cetrorelix, ganirelix | IVF - prevent premature LH surge |
| Degarelix | Prostate cancer (no flare; preferred if spinal metastases or urinary obstruction) |
| Elagolix | Endometriosis (oral); also used in uterine fibroids |
| Relugolix | Prostate cancer (oral, daily) |
VI. SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMs)
SERMs bind ERα/ERβ but have tissue-selective agonist or antagonist activity depending on the local co-regulator environment.
| Drug | Breast | Bone | Uterus | Uses |
|---|---|---|---|---|
| Tamoxifen | Antagonist | Agonist | Agonist | Breast cancer (adjuvant + treatment); risk of endometrial cancer |
| Raloxifene | Antagonist | Agonist | Neutral/antagonist | Osteoporosis; breast cancer prevention; no endometrial risk |
| Toremifene | Antagonist | - | - | Breast cancer |
| Bazedoxifene | Antagonist | Agonist | Neutral | Osteoporosis prevention; paired with CEE ("TSEC" - tissue-selective estrogen complex) |
| Ospemifene | Neutral | - | Some agonism | Dyspareunia / HSDD (postmenopausal); oral |
| Clomiphene | Antagonist | - | - | Infertility (anovulation); blocks hypothalamic ER → removes negative feedback → ↑ FSH/LH |
All SERMs: increased VTE risk (similar to estrogen)
Tamoxifen (key details):
- Competitive inhibitor of 17β-estradiol binding to ER
- In breast: net antagonist → used in ER+ breast cancer (premenopausal and postmenopausal)
- In bone and liver: agonist → maintains bone density, favorable lipid effects
- In uterus: agonist → endometrial hyperplasia and cancer risk (important ADR)
- Metabolized by CYP2D6 to active metabolite endoxifen; CYP2D6 inhibitors (e.g., fluoxetine, paroxetine) reduce efficacy
Fulvestrant (not a SERM - pure antagonist / SERD):
- Selective Estrogen Receptor Downregulator (SERD)
- Competitively binds ER → no agonist activity → promotes receptor degradation
- IM monthly injection
- ER+ HER2- advanced breast cancer (post-aromatase inhibitor failure)
VII. AROMATASE INHIBITORS (Estrogen Synthesis Inhibitors)
Block conversion of androgens → estrogens (aromatase = CYP19A1), primarily used in postmenopausal women (adrenal/peripheral aromatization is the main estrogen source post-menopause).
| Drug | Type | Notes |
|---|---|---|
| Anastrozole | Non-steroidal (reversible) | Once daily oral; breast cancer adjuvant |
| Letrozole | Non-steroidal (reversible) | Also used for ovulation induction in PCOS |
| Exemestane | Steroidal (irreversible, "suicide inhibitor") | Aromatase inactivation; different resistance pattern |
Uses:
- Adjuvant therapy for postmenopausal ER+ breast cancer (more effective than tamoxifen postmenopausally)
- Metastatic breast cancer
- Letrozole: ovulation induction (increasingly first-line over clomiphene in PCOS)
ADRs: arthralgia/myalgia ("AI arthropathy"), osteoporosis (↓ estrogen → ↑ bone resorption), hot flashes, vaginal dryness; NOT suitable for premenopausal women (ovarian aromatase overwhelms inhibition unless combined with GnRH agonist)
VIII. ANTIANDROGENS
Inhibitors of Androgen Synthesis
| Drug | Mechanism | Use |
|---|---|---|
| Ketoconazole (high dose) | Blocks multiple steroidogenic enzymes (CYP17A1) | Rapid castration (adrenal crisis risk) |
| Abiraterone | Selective CYP17A1 inhibitor (17α-hydroxylase + 17,20-lyase) | Castration-resistant prostate cancer; given with prednisone (prevents mineralocorticoid excess) |
| Finasteride | 5α-reductase type II inhibitor → ↓ DHT | BPH, male-pattern baldness (Propecia) |
| Dutasteride | 5α-reductase type I + II inhibitor → ↓ DHT more completely | BPH |
Androgen Receptor Antagonists
| Drug | Generation | Notes |
|---|---|---|
| Flutamide | 1st gen | Hepatotoxic; rarely used now |
| Bicalutamide | 2nd gen | Better tolerated; prostate cancer |
| Enzalutamide | 3rd gen | No agonist activity; crosses BBB (seizure risk); castration-resistant prostate cancer |
| Apalutamide, darolutamide | 3rd gen | Metastatic/non-metastatic prostate cancer; darolutamide - lower CNS penetration |
| Spironolactone | Non-selective (also MR antagonist) | Hirsutism in women; acne; used off-label as anti-androgen in trans women |
| Cyproterone acetate | Progestogenic antiandrogen | Hirsutism; trans women; not available in USA |
IX. PDE5 INHIBITORS (Erectile Dysfunction)
Mechanism: Nitric oxide (NO) → guanylyl cyclase → cGMP → smooth muscle relaxation in corpus cavernosum → increased blood flow → erection. PDE5 degrades cGMP; PDE5 inhibitors prolong cGMP action.
| Drug | t½ | Onset | Duration | Notes |
|---|---|---|---|---|
| Sildenafil (Viagra) | 4 h | 30-60 min | 12 h | Also used for pulmonary arterial hypertension; affected by food (high-fat meal delays absorption) |
| Vardenafil | 4 h | 30-60 min | 10 h | Most potent PDE5 selectivity (Ki 0.1 nM) |
| Tadalafil (Cialis) | 17.5 h | 30-120 min | 36 h | "Weekend pill"; also used for BPH; not affected by food |
| Avanafil | 1.3-2 h | 15-30 min | 6 h | Fastest onset; least food effect |
Critical drug interaction: Absolute contraindication with organic nitrates (both raise cGMP/cGMP-dependent pathways → catastrophic hypotension). Also caution with α-blockers.
ADRs: Headache, flushing, dyspepsia, nasal congestion, visual disturbances (sildenafil/vardenafil - PDE6 inhibition in retina), priapism (>4 hours → urological emergency)
X. GONADOTROPINS
| Drug | Composition | Use |
|---|---|---|
| FSH (follitropin α/β, urofollitropin) | Recombinant or urinary FSH | Ovulation induction (IVF); male infertility (spermatogenesis) |
| LH (lutropin α) | Recombinant LH | Combined with FSH in ovulation induction |
| hCG (choriogonadotropin) | LH-like activity | Trigger ovulation; male hypogonadism (stimulate Leydig cells); cryptorchidism |
| Menotropins (hMG) | FSH + LH from urinary source | Ovulation induction |
Risk of ovarian hyperstimulation syndrome (OHSS) - potentially life-threatening complication of gonadotropin therapy; characterized by enlarged ovaries, ascites, pleural effusions, hemoconcentration, thrombosis.
XI. Quick Clinical Reference Summary
| Drug Class | Key Drugs | Main Use | Critical ADR/Interaction |
|---|---|---|---|
| Estrogens | Estradiol, ethinyl estradiol, CEE | MHT, contraception | VTE, endometrial Ca (unopposed) |
| Progestins | Progesterone, MPA, levonorgestrel | MHT, contraception, ART | Mood changes, irregular bleeding, thrombosis |
| Combined OC | Ethinyl estradiol + progestin | Contraception | VTE, migraine with aura |
| GnRH agonists | Leuprolide, goserelin | Prostate Ca, endometriosis | Flare effect, osteoporosis |
| GnRH antagonists | Degarelix, elagolix | Prostate Ca, endo | Osteoporosis (no flare) |
| SERMs | Tamoxifen, raloxifene | Breast Ca, osteoporosis | VTE; tamoxifen → endometrial Ca |
| SERDs | Fulvestrant | ER+ breast Ca | IM only; injection site reactions |
| Aromatase inhibitors | Anastrozole, letrozole, exemestane | Postmeno breast Ca | Arthralgia, osteoporosis |
| Androgens | Testosterone (various forms) | Male hypogonadism | Polycythemia, virilization, suppressed spermatogenesis |
| Antiandrogens | Enzalutamide, abiraterone, finasteride | Prostate Ca, BPH, hirsutism | Abiraterone: mineralocorticoid excess |
| Mifepristone | Mifepristone | Medical abortion | Anti-glucocorticoid at high doses |
| PDE5 inhibitors | Sildenafil, tadalafil | Erectile dysfunction, PAH | Nitrate contraindication, priapism |
| Gonadotropins | FSH, hCG | ART, hypogonadism | OHSS |
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14e - Chapter 49 (Estrogens, Progestins, Androgens) and Chapter 48 (SERMs, aromatase inhibitors)
Needle stick injury microbiology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, multi-source data. Here is the complete answer:
Needlestick Injury - Microbiology & Management
What Is a Needlestick Injury?
A needlestick (percutaneous sharps) injury is accidental puncture of the skin by a needle or other sharp instrument contaminated with blood or body fluid. An estimated 600,000-800,000 needlestick injuries occur annually in the US among healthcare workers. The three principal bloodborne pathogens of concern are HIV, HBV (Hepatitis B), and HCV (Hepatitis C).
The Three Key Pathogens
1. Hepatitis B Virus (HBV)
Organism: Hepadnaviridae family; partially double-stranded circular DNA virus. Serological markers:
- HBsAg - surface antigen; marker of infection
- HBeAg - "e" antigen; marker of active viral replication and HIGH infectivity
- Anti-HBs - protective antibody; marker of immunity (vaccination or recovery)
Environmental survival: HBV retains infectivity at room temperature for at least 7 days after drying on surfaces - the most environmentally stable of the three bloodborne pathogens.
Transmission risk after needlestick:
| Source Status | Risk of Clinical Hepatitis | Risk of Seroconversion |
|---|---|---|
| HBsAg+ AND HBeAg+ (high viremia) | 22-31% | 37-62% |
| HBsAg+ but HBeAg- (low viremia) | 1-6% | 23-37% |
| HBsAg- | Negligible | Negligible |
HBV has the highest per-exposure transmission risk of all three bloodborne pathogens after needlestick.
2. Hepatitis C Virus (HCV)
Organism: Flaviviridae family; single-stranded positive-sense RNA virus. 6 major genotypes (1-6); genotype 1 predominant in USA.
Transmission risk after needlestick:
- Average seroconversion rate: ~1.8% (range 0-7%)
- Risk factors for transmission:
- Deep injury
- Hollow-bore needle (carries larger blood volume)
- Visible blood on needle
- High source viral load
Note: HCV is not transmitted efficiently by needlestick compared to HBV, but is far more likely to establish chronic infection (55-85% chronicity rate) compared to HBV (5-10% in adults).
3. Human Immunodeficiency Virus (HIV)
Organism: Retroviridae, subfamily Lentiviridae; single-stranded RNA virus with reverse transcriptase. Tropism for CD4+ T-helper cells and macrophages.
Transmission risk after needlestick:
| Route | Risk per Exposure |
|---|---|
| Percutaneous (needlestick) from known HIV+ source | ~0.3% |
| Mucous membrane splash | ~0.09% |
| Non-intact skin | <0.09% |
| Intact skin | Negligible |
Factors that increase HIV transmission risk:
- Large volume of blood (visible blood contamination on device)
- Deep injury
- Device placed directly in vein or artery
- High source viral load / advanced AIDS (source patient dying within 2 months of exposure)
- Prolonged contact
Contrast: HBV (22-31%) > HCV (1.8%) > HIV (0.3%) - HBV is the most transmissible by needlestick by far.
Other Pathogens (Less Common)
| Pathogen | Notes |
|---|---|
| HDV (Hepatitis D) | Only infects HBsAg-positive individuals (requires HBV co-infection); PEP same as HBV |
| HTLV-1/2 | Rare occupational transmission reported |
| Malaria | Rare case reports |
| Syphilis | Theoretical; Treponema pallidum very fragile outside host |
| Tetanus | Especially with soil/dirt-contaminated needles found in community settings |
Immediate Management Steps (Universal for All Needlestick Injuries)
Step 1: First Aid (IMMEDIATE)
- Do not squeeze or suck the wound
- Wash thoroughly with soap and water for a minimum of 15 minutes
- For mucous membrane splashes (eyes, mouth): irrigate copiously with water/saline
- Allow the wound to bleed freely
Step 2: Report & Assess (Within Hours)
- Report to supervisor immediately
- Document: time/date, type of sharp, activity being performed, site and depth of injury, source patient details
- Test the source patient (with consent where applicable) for:
- HIV (rapid antibody/antigen test)
- HBsAg (Hepatitis B surface antigen)
- Anti-HCV (Hepatitis C antibody)
- Test the exposed healthcare worker (baseline) for:
- HIV (antibody/antigen)
- Anti-HCV
- Anti-HBs (Hepatitis B surface antibody - to assess immunity)
- HBsAg
- Review vaccination history (especially HBV)
- Consider tetanus prophylaxis based on vaccination status and wound type
Pathogen-Specific Post-Exposure Prophylaxis (PEP)
Hepatitis B PEP
Management depends on the exposed worker's vaccination/immune status and the source's HBsAg status:
| Exposed Worker's Status | Source HBsAg+ | Source HBsAg- | Source Unknown |
|---|---|---|---|
| Unvaccinated | HBIG × 1 dose (0.06 mL/kg IM) + start HBV vaccine series | Start HBV vaccine series | Start HBV vaccine series |
| Vaccinated - known responder (anti-HBs ≥10 mIU/mL) | No treatment | No treatment | No treatment |
| Vaccinated - known non-responder | HBIG × 1 + start vaccine series OR HBIG × 2 doses | No treatment | HBIG × 1 + start vaccine series or HBIG × 2 |
| Vaccinated - antibody response unknown | Test anti-HBs: if <10 → HBIG × 1 + vaccine booster; if ≥10 → no treatment | No treatment | Test anti-HBs; if <10 → vaccine booster; recheck in 1-2 weeks |
Key points:
- HBIG and HBV vaccine can be given simultaneously at different anatomical sites
- PEP should be administered as soon as possible after exposure (within 24 hours ideally)
- HBV vaccine series (3-dose: 0, 1, 6 months) is the best pre-exposure prevention
Hepatitis C PEP
No pharmacological PEP is currently recommended for HCV.
Management focuses on:
- Baseline anti-HCV testing of exposed worker
- Follow-up testing at 3-6 months for seroconversion
- If source is HCV-positive: consider HCV RNA testing at 3-4 weeks post-exposure for early detection
- If acute HCV infection is confirmed: refer to hepatologist - highly effective direct-acting antivirals (DAAs) can achieve sustained virological response (SVR) ≥95% even in acute phase
- Treat acute HCV rather than waiting for spontaneous clearance (which occurs in ~15-45%)
HIV PEP
PEP must be initiated within 72 hours - the sooner the better (ideally within 1 hour). Efficacy diminishes significantly with delay beyond 72 hours.
Preferred PEP Regimen (US DHHS / Goldman-Cecil guidelines):
Tenofovir disoproxil fumarate (TDF) / Emtricitabine (FTC) [Truvada] + Dolutegravir (or Raltegravir)
- 3-drug regimen
- Duration: 28 days (4 weeks)
| Component | Drug | Class |
|---|---|---|
| Backbone | TDF/FTC (Truvada) or TAF/FTC (Descovy) | NRTI |
| Third agent (preferred) | Dolutegravir (DTG) | Integrase inhibitor |
| Third agent (alternative) | Raltegravir (RAL) | Integrase inhibitor |
Follow-up testing for exposed worker:
- HIV antibody/antigen at 4-6 weeks, 3 months, and 6 months
- If taking PEP: monitor for drug toxicity (renal function with TDF; metabolic effects)
Important considerations:
- If source patient is on antiretroviral therapy with known drug resistance, consult specialist
- National Clinicians' Post-Exposure Prophylaxis Hotline: 1-888-448-4911 (24/7 consultation)
- If source HIV status is unknown: assess epidemiologic likelihood and initiate PEP if high suspicion, with reassessment when source testing results return
Restrictions during follow-up period (regardless of PEP):
- Refrain from donating blood, plasma, organs, tissue, or semen
- No need to modify sexual practices or avoid pregnancy (exposed person is not infectious to contacts)
- No specific precautions needed to prevent secondary household transmission
Community Needlestick (Non-Occupational)
Children and members of the public who sustain injuries from needles discarded in public places (parks, public toilets):
- Risk is generally lower than occupational injury (older needle, less blood volume, dried)
- A review of 14 studies found no transmissions among 613 children exposed to community needlesticks (for HIV, HBV, HCV)
- However, every community needlestick warrants evaluation, wound care, and counseling
- Tetanus prophylaxis especially important (soil/environmental contamination)
- HBV PEP decision based on vaccination status
- HIV PEP: based on epidemiological risk assessment (estimated prevalence of HIV among IDUs in local community)
Risk Factor Summary for High-Transmission Exposures
Transmission risk is HIGHER when:
- Deep percutaneous injury (vs. superficial)
- Hollow-bore needle (vs. solid suture needle)
- Visible blood on device
- Device placed in vein or artery (blood-filled)
- Large volume of blood
- High viral titer in source (HIV: advanced AIDS; HBV: HBeAg+, high DNA)
- Source dies within 2 months of exposure (marker of advanced disease)
Prevention Strategies
- Universal/Standard Precautions - treat all blood and body fluids as potentially infectious at all times
- HBV vaccination of all healthcare workers - most effective single intervention (gives >95% seroprotection)
- Safety-engineered devices - self-sheathing needles, needleless IV systems, retractable lancets
- No recapping of needles - single most common activity leading to needlestick injury
- Proper disposal: sharps containers - never overfill; place near point of use
- PPE: gloves, eye protection, gowns when splash risk exists
- Occupational health reporting systems - encourage reporting culture (many needlestick injuries go unreported)
- Double-gloves during high-risk procedures (surgical, obstetric)
Comparative Transmission Risk Summary
| Feature | HBV | HCV | HIV |
|---|---|---|---|
| Per-needlestick risk | 22-62% (HBeAg+) | ~1.8% | ~0.3% |
| Environmental stability | Survives 7 days dry | Hours-days | Minutes-hours |
| Vaccine available | Yes (highly effective) | No | No |
| PEP available | Yes (HBIG + vaccine) | No | Yes (ARV, 28 days) |
| Chronicity if infected | 5-10% (adults) | 55-85% | 100% (lifelong) |
| Cure possible | Functional cure (HBsAg loss) | Yes (DAAs, >95% SVR) | No (suppression only) |
Sources: Yamada's Textbook of Gastroenterology 7e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Goldman-Cecil Medicine; Harriet Lane Handbook 23e; Red Book 2021 (AAP)
This is a shared conversation. Sign in to Orris to start your own chat.