Septal swell body. MS ENT university exam pattern for 10 marks.
Reading File
Finding Sources
Searching the Web
septal swell body anatomy nasal ENT MS exam
Reading File
Reading Web Page
https://richardharvey.sydneyentclinic.com/2026/04/15/septal-…
Reading File
Loading Image
I now have comprehensive information to write a complete 10-mark MS ENT university exam answer. Here it is:
Septal Swell Body
Definition
The septal swell body (SSB) is a fusiform, widened region of the anterior nasal septum located anterior to the middle turbinate at the level of the internal nasal valve. It represents the thickest portion of the nasal septal mucosa and behaves physiologically like a turbinate.
Also known as: nasal septal turbinate, septal body, septal tumescence, septal cavernous body, Kiesselbach's ridge.
Historical Background
- First described by Morgagni (1662) as a "mucosal protuberance located anteriorly on the septum."
- Schiefferdecker described it as a vascular network on the anterior nasal septum.
- The term "septal swell body" entered ENT literature in German publications around 1951.
Anatomy
Location:
- Anterior nasal septum
- Superior to the inferior turbinate
- Anterior to the middle turbinate
- At the internal nasal valve region
Structure:
- Fusiform (spindle-shaped) - widest at the middle, tapering at both ends
- Composed of septal cartilage and bone covered by thick mucosa
- The thickest mucosal segment of the entire nasal septum
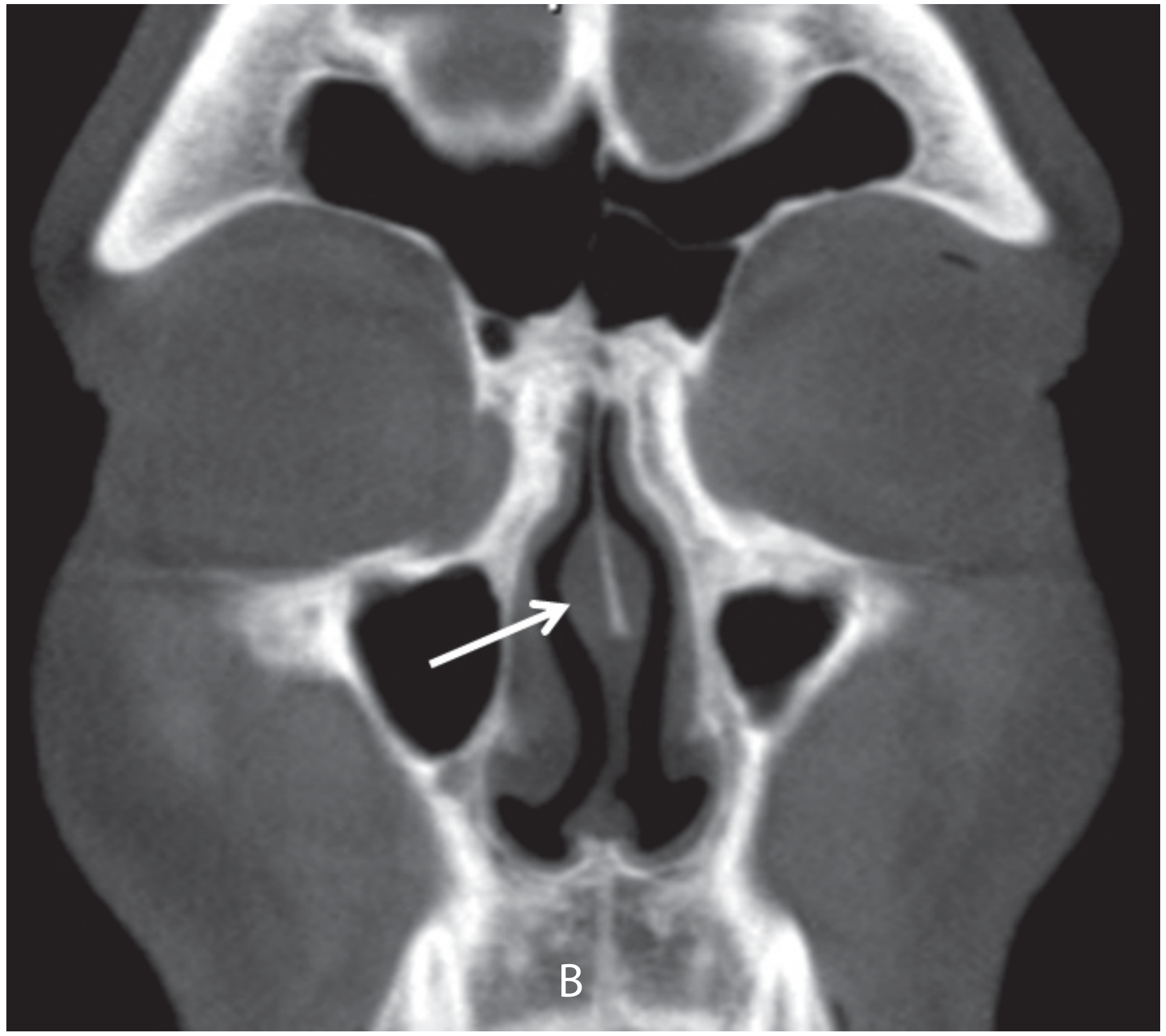
Imaging: Identified on coronal CT as a soft tissue bulge projecting from the anterosuperior septum into the nasal airway (see image below).
Histology
- Contains an increased amount of venous sinusoids (erectile tissue) and seromucinous glands
- Fewer glandular elements compared to adjacent septal mucosa
- Histology closely resembles that of the inferior turbinate - not ordinary septal mucosa
- Capable of engorgement and de-engorgement due to the vascular sinusoids, similar to turbinate erectile tissue
- Undergoes the same inflammatory remodelling as inferior turbinate mucosa in chronic sinonasal disease
Physiology and Functions
- Nasal airflow regulation - The vascular sinusoids allow the SSB to swell or shrink, altering resistance at the internal nasal valve (the narrowest part of the nasal airway)
- Humidification - Proximity to the internal nasal valve and its glandular content contribute to conditioning of inspired air
- Nasal cycle - Participates in the alternating congestion/decongestion cycle, analogous to the inferior turbinate
- Gravity-dependent size - SSB volume changes with head position, similar to turbinates
Clinical Significance
Why it Matters
- Frequently mistaken for high septal deviation on clinical examination and imaging - this is the most important pitfall
- Enlargement can cause significant nasal obstruction, especially at the internal nasal valve
- May be responsible for persistent nasal obstruction after otherwise adequate septoplasty if left untreated
Association with Disease
- Allergic rhinitis - SSB enlarges significantly in allergic patients (same inflammatory hypertrophy as inferior turbinate)
- Chronic rhinosinusitis - Associated with fibrosis and poor response to topical steroids
- Turbinate hypertrophy - Frequently co-exists
Diagnosis
- Anterior rhinoscopy / nasal endoscopy - Visible as a soft, bulging protuberance on the anterosuperior septum
- Coronal CT scan - Best imaging modality; soft tissue density mass on the septal surface at the level of inferior/middle turbinate junction
- Differentiation from septal deviation - SSB is a soft-tissue mucosal lesion; it cannot be corrected by submucosal resection or cartilage excision alone
Management
Medical
- Intranasal corticosteroid sprays (first-line; may reduce SSB volume in inflammatory disease)
- Nasal decongestants (temporary relief; confirm erectile nature of the lesion)
- Allergen control / treatment of underlying allergic rhinitis
Surgical (indicated when medical treatment fails)
| Technique | Details |
|---|---|
| Radiofrequency ablation (RFA) | Transmucosal, incisionless; submucosal RF wand reduces volume with minimal mucosal disruption |
| Cauterization / cryotherapy | Older techniques; less preferred |
| Submucosal resection | Excision of submucosal tissue through a mucosal incision |
| Septoplasty + SSB reduction | Combined procedure for co-existing septal deviation |
Key surgical principle: Because the SSB contains seromucinous glands, overly aggressive resection risks mucosal damage and dryness. Conservative volume reduction is preferred.
Evidence: A 2025 systematic review and meta-analysis (7 studies, n=232 patients) showed that septal swell body volume reduction (SSBVR) significantly improved nasal obstruction scores, and adding SSB reduction to inferior turbinate surgery improved outcomes compared to turbinate surgery alone (SMD 0.47).
Important Exam Points (Summary Table)
| Feature | Detail |
|---|---|
| Location | Anterosuperior nasal septum, anterior to middle turbinate, at internal nasal valve |
| Shape | Fusiform |
| Histology | Venous sinusoids + seromucinous glands (like inferior turbinate) |
| Key mimicker | High septal deviation (must distinguish!) |
| Function | Airflow regulation, humidification, nasal cycle |
| Best imaging | Coronal CT |
| First-line Rx | Intranasal corticosteroids |
| Surgical option | Radiofrequency submucosal ablation |
Sources:
This is a shared conversation. Sign in to Orris to start your own chat.