Esophagus classification - upper middle and lower 1/3 rd for endoscopy purpose
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative sources. Here is the complete answer:
Esophagus Classification - Upper, Middle, and Lower Thirds (Endoscopic)
For endoscopic purposes, the esophagus is measured by distance from the upper incisor teeth (not the nose). The total esophageal length from incisors is approximately 40 cm (incisors to GEJ).
Endoscopic Landmark Reference Points (from incisors)
| Landmark | Distance from Incisors |
|---|---|
| Upper esophageal sphincter (UES) / Cricopharyngeus | 15 cm |
| Aortic arch crossing | 22 cm |
| Left mainstem bronchus crossing | 27 cm |
| Diaphragm / Lower esophageal sphincter (LES) / GEJ | 40 cm |
- Tintinalli's Emergency Medicine; Fischer's Mastery of Surgery, p. 726; Scott-Brown's Otorhinolaryngology
- Three anatomical constrictions at 15 cm, 23-27 cm, and 38-40 cm from incisors - these are the sites most prone to FB impaction and injury.
Division into Thirds (for Endoscopy / Oncology Staging)
The esophagus spans 15 cm to 40 cm from the incisors = 25 cm total endoscopic length, divided roughly into three equal segments:
| Segment | Distance from Upper Incisors | Length | Key Contents |
|---|---|---|---|
| Upper third (cervical + upper thoracic) | 15 - 24 cm | ~8 cm | Cricopharyngeus to just below aortic arch |
| Middle third (mid-thoracic) | 24 - 32 cm | ~8 cm | Aortic arch level to mid-thorax |
| Lower third (lower thoracic + abdominal) | 32 - 40 cm | ~8 cm | Mid-thorax to GEJ/cardia |
Note on variation: Different sources round slightly differently. A commonly used clinical approximation is:
- Upper third: 15-24 cm
- Middle third: 24-32 cm
- Lower third: 32-40 cm
Anatomical Diagram
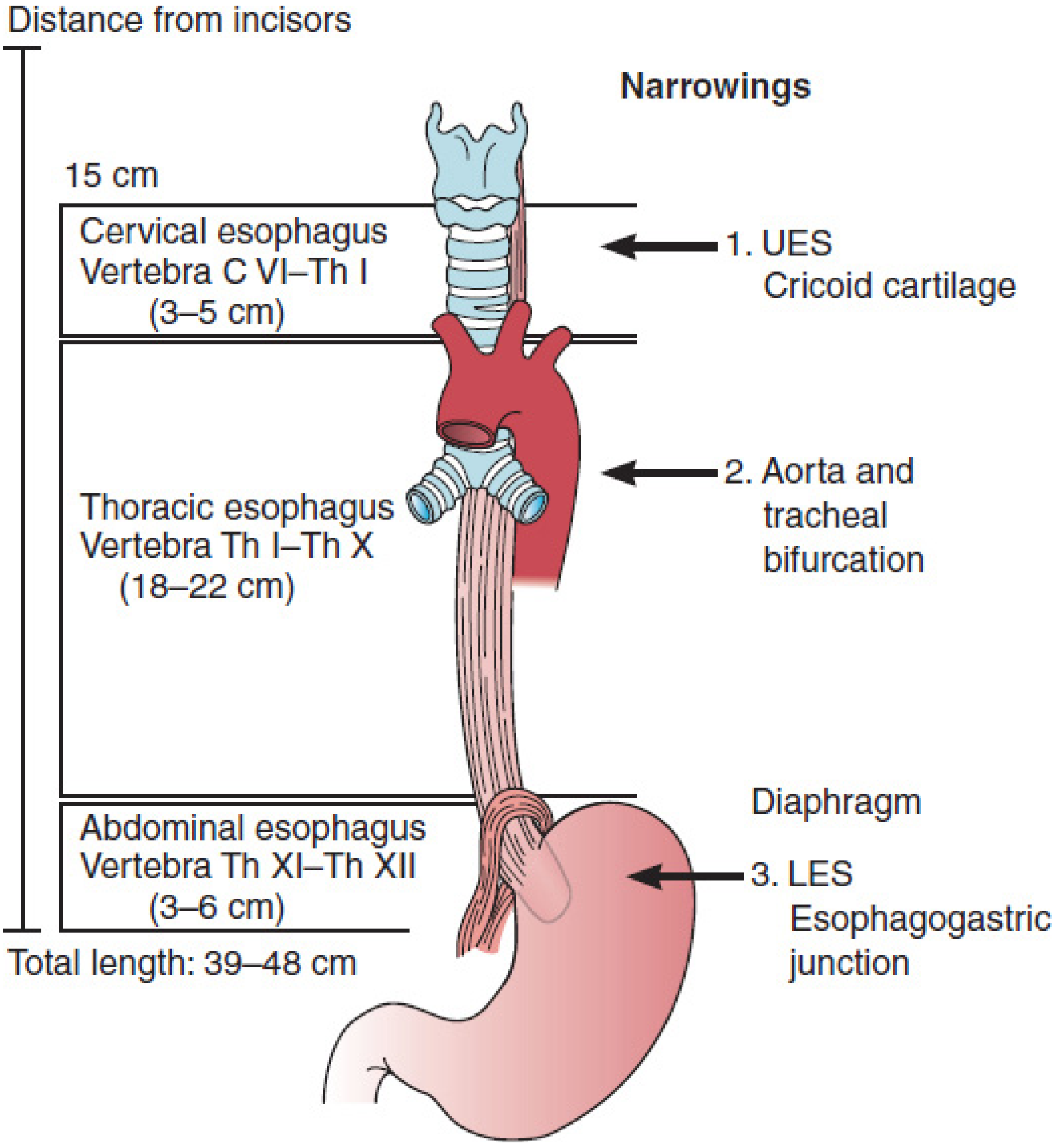
Source: Mulholland & Greenfield's Surgery - note the cervical (3-5 cm), thoracic (18-22 cm), and abdominal (3-6 cm) segments with three physiological narrowings.
Clinical Relevance of Each Third
Upper third (15-24 cm):
- Squamous cell carcinoma: 10-20% of esophageal SCC
- Striated muscle in upper 1/3rd
- Risks: aspiration, fistula to airway, recurrent laryngeal nerve involvement
Middle third (24-32 cm):
- Most common location for squamous cell carcinoma (~50%)
- Proximity to aorta and tracheal bifurcation - surgical resection more complex
- Varices can involve this segment
Lower third (32-40 cm):
-
Squamous cell carcinoma: ~40%; adenocarcinoma: >80% in lower third/GEJ
-
Most common site for esophageal varices (and most prognostically important size)
-
GERD, Barrett's esophagus, and adenocarcinoma cluster here
-
Smooth muscle in lower 2/3rds
-
Sabiston Textbook of Surgery (Table 84.1); Sleisenger & Fordtran's GI and Liver Disease
Quick Memory Aid
15 - 24 - 32 - 40 (from incisors) Upper = 15 to ~24 | Middle = 24 to ~32 | Lower = 32 to 40
This is a shared conversation. Sign in to Orris to start your own chat.