vancover classification
Vancouver classification periprosthetic femoral fracture
https://pmc.ncbi.nlm.nih.gov/articles/PMC3069264
Vancouver Classification - Periprosthetic Femoral Fractures
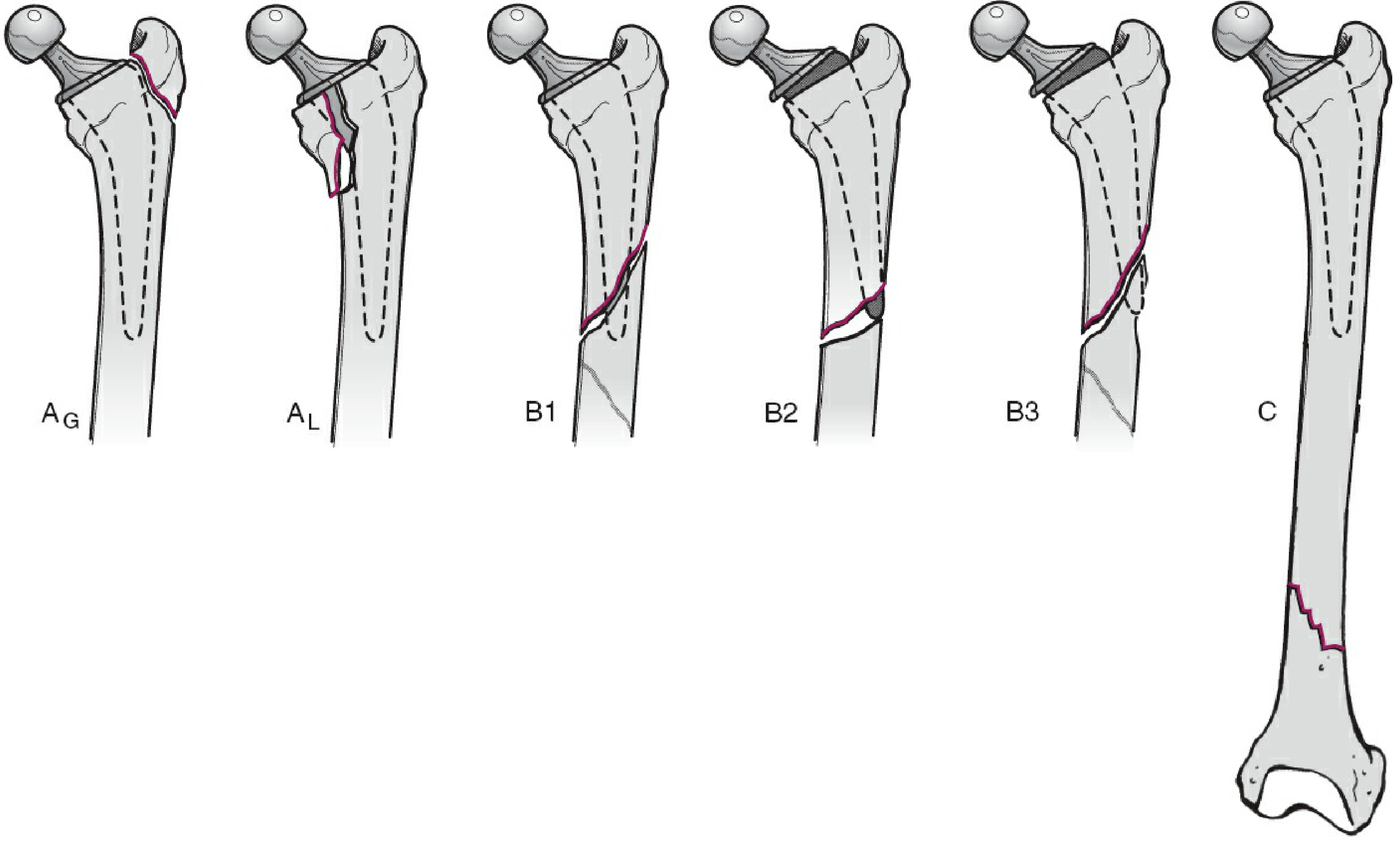
TYPE A - Trochanteric Region
| Subtype | Location | Treatment |
|---|---|---|
| A(G) - Greater trochanter | Fracture of the greater trochanter | Conservative + abduction precautions; ORIF (claw plate + cables) if displaced >2.5 cm |
| A(L) - Lesser trochanter | Fracture of the lesser trochanter (rare) | Conservative unless a large portion of the medial calcar is involved (then consider revision) |
TYPE B - Around or Just Below the Stem
| Subtype | Stem | Bone Stock | Treatment |
|---|---|---|---|
| B1 | Well-fixed | Good | ORIF with lateral locked plate ± cortical strut allograft |
| B2 | Loose | Good | Revision THA with long-stem prosthesis (+ adjunctive fixation) |
| B3 | Loose | Poor (osteolysis/deficient) | Revision THA + structural allograft, tumor prosthesis, or allograft-prosthetic composite |
Key pitfall: Distinguishing B1 from B2 preoperatively can be difficult. ORIF alone for a B2 fracture (loose stem) gives unsatisfactory results - always have revision components available intraoperatively.
TYPE C - Well Below the Stem Tip
- Fracture is distal to the tip of the prosthesis, treated entirely on its own merits
- Treatment: ORIF as for any standard femoral shaft/distal femur fracture, without regard for the prosthesis (except ensuring fixation does not leave a stress-riser gap between plate and stem tip)
Intraoperative Vancouver Classification (Extended)
- Subtype I: Simple cortical perforation
- Subtype II: Nondisplaced linear cortical crack
- Subtype III: Displaced or unstable fracture
Summary Table
| Type | Location | Bone Stock | Stem | Treatment |
|---|---|---|---|---|
| A(G) | Greater trochanter | Good | Fixed | Conservative / ORIF if >2.5 cm displaced |
| A(L) | Lesser trochanter | Good | Fixed | Conservative / ORIF if large calcar involved |
| B1 | Around stem | Good | Fixed | ORIF ± strut allograft |
| B2 | Around stem | Good | Loose | Revision THA (long stem) |
| B3 | Around stem | Poor | Loose | Revision THA + bone augmentation or tumor prosthesis |
| C | Below stem | Good | Fixed | ORIF (independent of prosthesis) |
Clinical Pearls
- Type B2 is the most common type seen in practice
- Mortality after periprosthetic fracture is significant: ~9% at 90 days, 21% at 1 year for revision cases (NHS National Joint Registry data)
- Outcomes after revision for periprosthetic fracture are worse than revision for aseptic loosening
- The classification has been validated for reliability and inter-/intraobserver agreement and is the current gold standard
door classification of bone stock
Dorr classification femoral bone stock canal morphology types A B C
Dorr classification hip femoral canal type A B C cortical index THA stem selection
https://pmc.ncbi.nlm.nih.gov/articles/PMC7371079
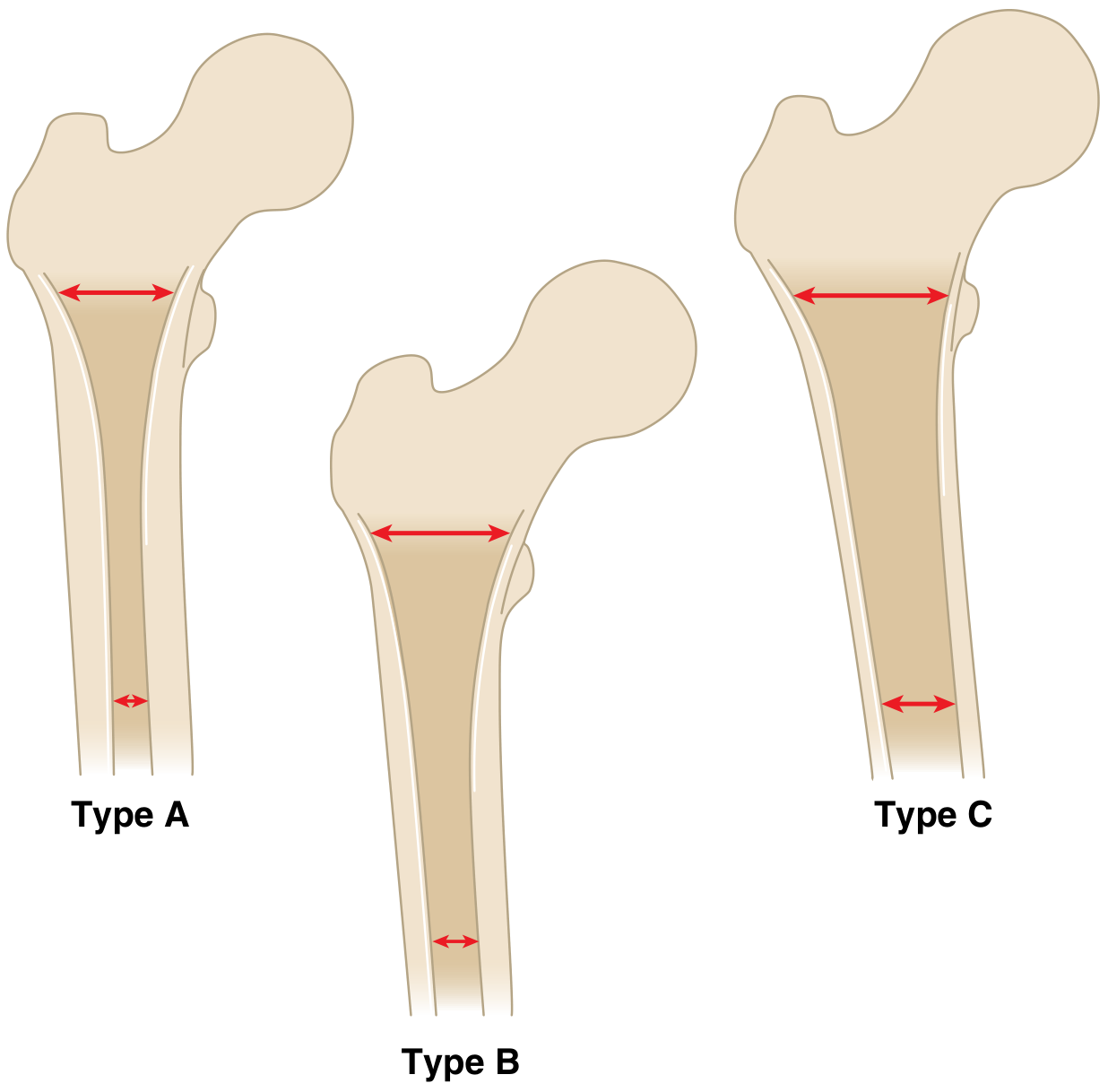
Dorr Classification of Proximal Femoral Bone Morphology
The Three Types
| Feature | Type A | Type B | Type C |
|---|---|---|---|
| Canal shape | "Champagne flute" - wide metaphysis, narrow diaphysis | Intermediate | "Stovepipe" - uniform wide canal throughout |
| Cortices | Thick on both AP and lateral XR | Thinning of posterior cortex on lateral XR | Thinning on both AP and lateral views |
| Cortical Index | > 0.58 (thick cortex) | 0.50 (intermediate) | < 0.42 (thin cortex) |
| Canal Flare Index (CFI) | ≥ 4.7 (high flare) | 3.0 - 4.7 | < 3.0 (no flare) |
| Typical patient | Young male | Intermediate | Elderly female, osteoporotic |
| Bone quality | Good | Moderate | Poor |
| Preferred fixation | Cementless | Cementless | Cemented (preferred) |
Quantitative Indices (how to measure)
- Measured on AP radiograph at 10 cm distal to the mid-lesser trochanter
- Formula: (Diaphyseal diameter - Intramedullary canal diameter) / Diaphyseal diameter
- Type A: CI > 0.58 | Type B: ~0.50 | Type C: < 0.42
- Intramedullary isthmus width / canal width at calcar level
- Higher ratio = wider distal canal (Type C)
- Type C: ~0.64 | Type A: ~0.57
- Intracortical width 20 mm proximal to lesser trochanter / isthmus width
- Champagne flute (Type A): ≥ 4.7 | Normal (Type B): 3.0-4.7 | Stovepipe (Type C): < 3.0
Clinical Significance
- Small diaphyseal canal relative to wide metaphysis - risk of medial calcar fracture if templating over-fills metaphysis
- Thick posterior fin can anteriorly displace the stem, causing retroversion and instability
- Best treated with cementless stems; short stems or metaphyseal-filling designs are suitable
- Most common type
- Posterior cortex thins on lateral view
- Cementless fixation is appropriate
- Transition zone between A and C characteristics
- Wide, uniform canal with thin cortices - characteristic of osteoporosis
- Poor metaphyseal fill with cementless stems - risk of subsidence
- Cemented fixation traditionally preferred
- However: modern cementless stem designs have shown durable fixation even in Type C - but intraoperative fracture risk remains a concern in elderly/inactive patients
Reliability Note
aseptic loosening vs septic loosening
Aseptic Loosening vs. Septic Loosening
Overview
| Feature | Aseptic Loosening | Septic Loosening (PJI) |
|---|---|---|
| Definition | Mechanical failure of implant-bone interface WITHOUT infection | Implant loosening CAUSED BY periprosthetic joint infection |
| Cause | Wear debris - osteolysis, micromotion, stress shielding | Bacteria (biofilm) - inflammatory destruction of bone-implant interface |
| Incidence | Most common cause of late THA/TKA failure | ~1-2% primary THA; ~4% revision THA |
| Onset | Gradual, years after surgery | Acute (early), subacute, or chronic (late) |
Aseptic Loosening
- Bearing surface wear (polyethylene, metal, cement) produces micro/nano particles
- Macrophages phagocytose particles → activated → release pro-inflammatory cytokines (IL-1, TNF-α, PGE2)
- Osteoclast activation → periprosthetic osteolysis
- Progressive bone loss → implant micromotion → loosening
- PMMA cement debris also damages polyethylene, worsening the cycle
- Metal-on-polyethylene bearing (high wear rate)
- Component malposition → increased wear
- High-impact activities / young active patients
- Metal-on-metal bearings → adverse local tissue reaction (ALTR)
- Poor cementing technique (mantle defects)
- Gradual onset of start-up pain (pain on initiating movement, relieved with activity - classic "loosening pain")
- No fever, no systemic signs
- Normal or mildly elevated inflammatory markers (CRP, ESR)
- Joint aspiration: non-inflammatory fluid, sterile cultures
- Progressive radiolucent lines at bone-cement or bone-implant interface
- Periprosthetic lytic lesions (osteolysis)
- Component migration / subsidence / tilt
- Eccentric wear of polyethylene (femoral head shifts within cup)
- No periosteal reaction (unlike infection)
Septic Loosening (Periprosthetic Joint Infection - PJI)
- Bacteria (most commonly Staphylococcus epidermidis, S. aureus, streptococci) adhere to the implant surface and form a biofilm (glycocalyx)
- Biofilm protects bacteria from antibiotics and host immune response
- Bacterial products and host inflammatory response destroy bone at the interface
- Chronic low-grade biofilm infections may present similarly to aseptic loosening
- Acute postoperative: < 4 weeks (direct intraoperative contamination)
- Chronic/delayed: > 3 weeks, most common presentation - low-grade biofilm (e.g. S. epidermidis slowly multiplying)
- Acute hematogenous: Any time - seeding from remote site (dental, urinary, respiratory)
- Persistent pain + warmth + swelling + erythema
- Sinus tract (pathognomonic if present)
- Fever, raised WBC (not always - especially in chronic biofilm PJI)
- CRP and ESR elevated (CRP more reliable - returns to normal faster postoperatively)
Diagnosis - ICM-18 Criteria for PJI (2018)
- Two positive periprosthetic cultures with same organism
- Sinus tract communicating with the joint
| Parameter | Threshold | Score |
|---|---|---|
| Serum CRP (chronic) | ≥ 10 mg/L | 2 |
| Serum ESR | ≥ 30 mm/h | 1 |
| Synovial WBC (acute/chronic) | ≥10,000 / ≥300 cells/μL | 3 |
| Synovial PMN % (acute/chronic) | ≥90% / ≥70% | 2 |
| Positive leukocyte esterase or α-defensin | ++ / ≥1.0 | 3 |
| Single positive culture | - | 2 |
| Positive histology at surgery | - | 3 |
| Gross purulence intraoperatively | - | 3 |
Differentiating the Two - Key Points
| Feature | Aseptic | Septic |
|---|---|---|
| CRP/ESR | Normal or mildly elevated | Elevated (CRP more reliable) |
| Joint aspiration WBC | < 1750 cells/μL (hip) | ≥ 300 cells/μL (chronic) / ≥ 10,000 (acute) |
| PMN% | < 65% | ≥ 70% (chronic) / ≥ 90% (acute) |
| α-defensin | Negative | Positive (≥ 1.0) |
| Culture | Sterile | Positive (may need multiple samples) |
| Radiolucency pattern | Smooth, scalloped osteolysis | Irregular, may have periosteal reaction |
| Nuclear medicine | Tc bone scan positive in both; labelled WBC scan (indium) positive only in infection - sensitivity 64-77%, specificity 78-86% |
Treatment
| Aseptic Loosening | Septic Loosening (PJI) | |
|---|---|---|
| Surgery | Single-stage revision arthroplasty ± bone grafting / augments for bone defects | Two-stage revision (preferred) |
| Stage 1 | N/A | Remove implant + debridement + antibiotic-loaded cement spacer + deep cultures |
| Between stages | N/A | IV/oral antibiotics guided by sensitivities (typically 6 weeks) |
| Stage 2 | N/A | Remove spacer, re-implant prosthesis once infection cleared |
| Alternatives | One-stage revision (selected cases, known organism, good bone stock); DAIR (debridement, antibiotics, implant retention) for acute/early PJI with stable implant | |
| Outcomes | Generally good, though worse than primary THA | Worse overall; mortality 9% at 90 days, 21% at 1 year |
zone of cementing
Zones of Cementing in Total Hip Arthroplasty
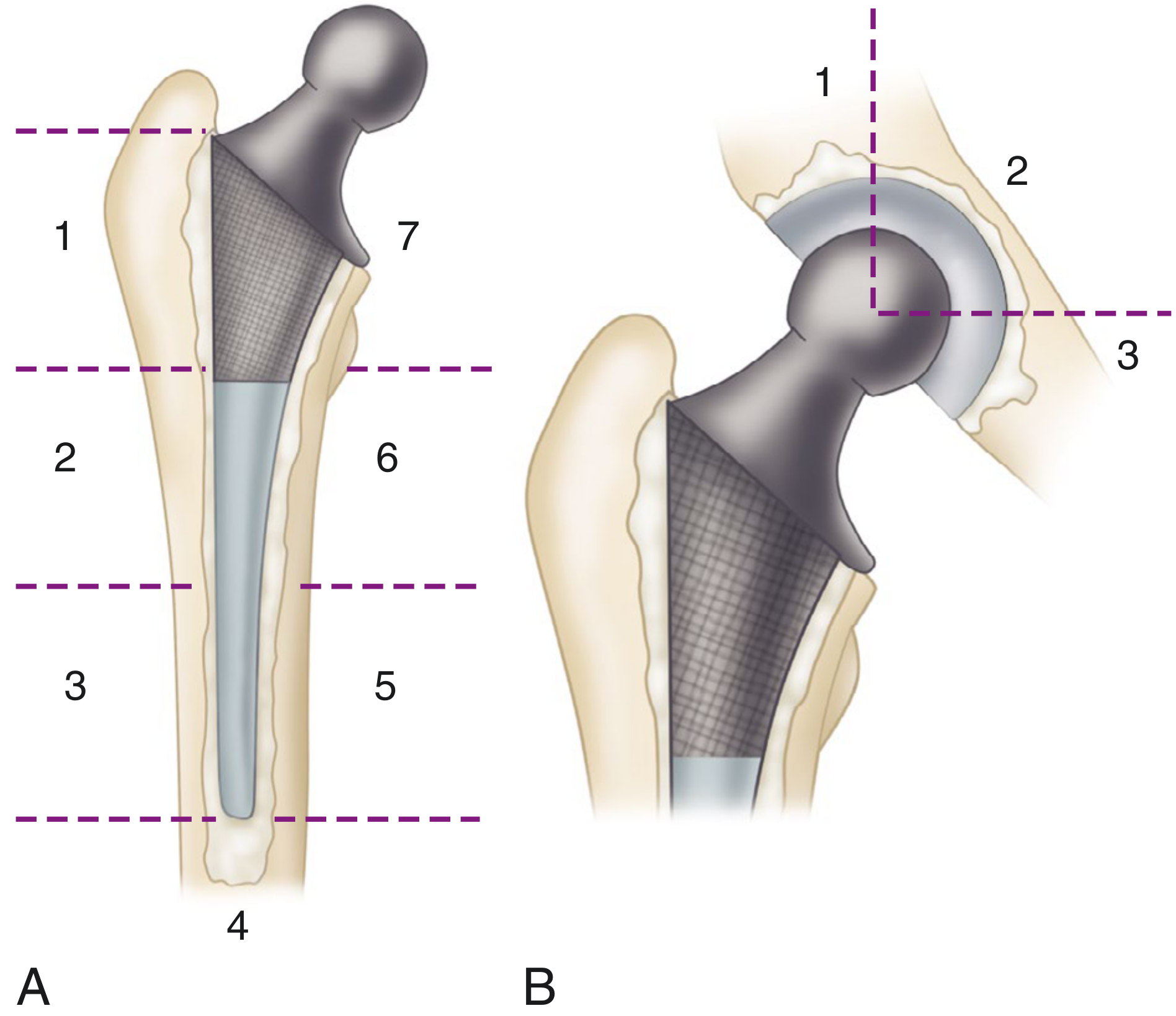
A. Gruen Zones - Femoral Component (7 Zones)
| Zone | Location | Side |
|---|---|---|
| 1 | Superolateral (proximal, lateral) | Lateral |
| 2 | Mid-lateral | Lateral |
| 3 | Inferolateral (distal, lateral) | Lateral |
| 4 | Stem tip (distal) | Distal |
| 5 | Inferomedial (distal, medial) | Medial |
| 6 | Mid-medial | Medial |
| 7 | Superomedial (proximal, medial - calcar region) | Medial |
- Zone 1: Radiolucency between stem and cement - indicates stem debonding from cement, possible early stem deformation
- Zone 7: Fragmentation of cement at the superomedial calcar region - classic early loosening sign
- Zone 4: Cement mantle fracture at the stem tip - axial loading fracture
- Zones 2 & 6: Radiolucency between cement mantle and surrounding bone - cement-bone interface failure
- Stem subsidence, varus tilting, stem fracture are other signs
B. DeLee & Charnley Zones - Acetabular Component (3 Zones)
| Zone | Location | Clinical significance |
|---|---|---|
| Zone 1 | Superolateral (above center line, lateral) | Load-bearing zone - most critical; rim integrity key |
| Zone 2 | Superior (above center line, medial) | Central / dome area |
| Zone 3 | Inferomedial (below center line) | Medial wall / teardrop area |
| Score | Meaning |
|---|---|
| 0 | No lesion |
| 1 | Small lesion < 1 cm |
| 2 | Lesion ≥ 1 cm, superolateral rim intact ≥ 1 cm OR radiolucent line < 2 mm |
| 3 | Superolateral rim intact < 1 cm OR radiolucent line ≥ 2 mm |
| 4 | Osteolysis invades entire superolateral rim or rim fracture |
C. Barrack Grading of Cement Mantle Quality (Femur)
| Grade | Appearance | Significance |
|---|---|---|
| A | Complete fill ("white-out"), no radiolucencies | Ideal |
| B | Slight radiolucency at bone-cement interface (< 50%) | Acceptable |
| C | Lucency around 50-99% of interface OR any cement mantle defect | High risk of loosening |
| D | Complete lucency on any projection OR mantle defect at stem tip | High risk of loosening |
Clinical Use - Harris Radiographic Loosening Criteria
| Grade | Definition |
|---|---|
| Definite loosening | Migration of component or cement |
| Probable loosening | Complete radiolucency around entire cement mantle |
| Possible loosening | Incomplete radiolucency surrounding > 50% of cement |
Key Technical Errors Causing Loosening
- Inadequate removal of soft cancellous bone from calcar - cement lacks dense bone support
- Thin or incomplete cement mantle - cracks under cyclic loading
- Stripping all trabecular bone - removes surface for cement interdigitation
- Inadequate cement pressurization - poor flow into cancellous interstices
- Stem motion during cement hardening
- Voids in cement from poor mixing technique
- Varus malalignment of the stem
different cementing techniques in thr and generation of cementing
generations of cementing technique total hip replacement first second third fourth generation
https://www.wheelessonline.com/joints/cementing-technique-fo…
Generations of Cementing Technique in Total Hip Replacement
1st Generation - Finger Packing (Charnley Era, 1960s-1970s)
- Cement mixed by hand in open bowl
- Introduced into the femoral canal by finger packing (digital pressure)
- No medullary plug
- No cement gun
- No pressurization device
- No porosity reduction (no vacuum, no centrifugation)
- Canal not specifically cleaned or dried
- Poor cement-bone interdigitation
- High porosity in cement mantle (voids, air bubbles reduce strength by ~30%)
- Blood and fat contamination of cement
- Inadequate pressurization
- No control of cement depth
- Aseptic loosening rate up to 30% at 10 years (Stauffer, 1982)
2nd Generation - Modern Canal Preparation (1970s-1980s)
| Step | What Was Added |
|---|---|
| Canal cleaning | Pulsatile lavage (jet washing) to remove fat, blood, debris from cancellous bone |
| Canal drying | Adrenaline-soaked (epinephrine) sponges to achieve hemostasis and dry the canal |
| Medullary plug | Distal cement restrictor (plastic or cement plug) placed ~1-2 cm below stem tip to block the canal, allowing pressurization |
| Retrograde filling | Cement gun fills canal from distal to proximal (retrograde), preventing air entrapment |
| Pressurization | Digital or wedge pressurizer holds cement under pressure during insertion |
| Medullary brush | Canal brushed to clean trabecular surfaces |
3rd Generation - Cement Quality Improvement (1980s-1990s)
| Step | What Was Added |
|---|---|
| Vacuum mixing | Cement mixed under vacuum to eliminate air bubbles and reduce porosity by up to 50% |
| Centrifugation | Alternative to vacuum - spins mixed cement to remove voids |
| Pressurization device | Dedicated proximal femoral seal to maintain continuous pressurization during cement injection and stem insertion |
| Stem surface modification | Pre-coating of stem with cement (controversial) or surface texturing to improve stem-cement bonding |
4th Generation - Stem Centralization (1990s-present)
| Step | What Was Added |
|---|---|
| Proximal centralizer | Collar or fins at the proximal stem ensure the stem is centered in the canal proximally |
| Distal centralizer | Plastic centralizer at the stem tip ensures stem is equidistant from canal walls distally |
| Pre-heating the stem | Warming the stem slows cement polymerization at the stem-cement interface, improving interdigitation and reducing micro-debonding |
| Stem design optimization | Tapered polished stems (Exeter design) allow controlled subsidence within the cement mantle (composite beam concept), reducing interface stress |
Summary Comparison Table
| Generation | Era | Key Feature | Problem Solved |
|---|---|---|---|
| 1st | 1960s | Finger packing | Baseline (no refinement) |
| 2nd | 1970s-80s | Pulsatile lavage + distal plug + cement gun (retrograde) + pressurization | Blood/fat contamination; poor pressurization |
| 3rd | 1980s-90s | Vacuum mixing / centrifugation + improved pressurizer | Cement porosity and void formation |
| 4th | 1990s+ | Proximal + distal centralizers + pre-heated stem | Inadequate/non-uniform cement mantle |
Components of the Modern (4th Gen) Cementing Technique - Step by Step
- Canal preparation: Pulsatile lavage + medullary brush + epinephrine sponges (dry, clean canal)
- Distal plug: Cement restrictor placed ~2 cm below stem tip
- Vacuum mixing: Mix PMMA under vacuum to reduce porosity
- Retrograde filling: Cement gun fills canal from distal to proximal
- Pressurization: Proximal seal + pressurizer applied as cement is injected
- Stem insertion: Pre-heated, centralized stem (distal + proximal centralizers) inserted in neutral alignment
- Held still: Stem held absolutely still while cement polymerizes (prevents debonding)
- Check cement mantle: Aim for Barrack grade A ("white-out") on postop XR
Note on Cemented vs. Hybrid THA
- Cemented acetabular cup has higher long-term loosening rates than cementless, and advances in cementing technique have NOT significantly reduced acetabular failure - hence most surgeons now use cementless acetabular cups routinely
- Cemented femoral stem (especially polished tapered designs like Exeter) continues to show excellent 15-20+ year survivorship with modern technique - still widely used, especially in elderly patients with poor bone stock (Dorr Type C)
- Hybrid THA = cementless cup + cemented stem - currently the most common construct in many registries
type of stems and acetabular cup
types of femoral stems acetabular cups total hip arthroplasty classification cemented cementless design
https://journaloei.scholasticahq.com/article/143525-cementle…
Types of Femoral Stems and Acetabular Cups in THA
PART 1: FEMORAL STEMS
A. Classification by Fixation Method
1. Cemented Stems
| Design | Concept | Example | Mechanism |
|---|---|---|---|
| Composite Beam (bonded) | Stem fully bonded to cement mantle - load transferred along entire stem length | Charnley stem | Surface roughened/textured to maximize stem-cement bond |
| Taper-Slip (unbonded) | Polished stem designed to subside within cement mantle under load - generates hoop stresses that improve fixation | Exeter stem | Polished collarless double-taper - controlled subsidence is intentional |
- Collared: Collar rests on calcar - transfers some load via collar-calcar contact, prevents subsidence
- Collarless: No collar - depends entirely on cement for load transfer (Exeter principle)
2. Cementless (Uncemented) Stems
- Bone ingrowth: Bone grows into porous surface (beads, mesh, trabecular metal)
- Bone ongrowth: Bone grows onto grit-blasted/hydroxyapatite-coated surface
B. Classification by Stem Geometry (Radaelli Classification - 6 Types)
| Type | Geometry | Fixation Zone | Characteristics | Example |
|---|---|---|---|---|
| Type A - Flat taper (single wedge) | Wedge-shaped in one plane (AP) only | Metaphyseal | Simple design; good metaphyseal fill; risk of aseptic loosening higher vs B | Corail, Summit |
| Type B1 - Quadrangular taper (double wedge, narrow) | Tapered in both AP and ML planes; narrow | Metaphyso-diaphyseal | Most widely used cementless design | Tri-Lock, Accolade |
| Type B2 - Quadrangular taper (double wedge, standard) | Tapered in both AP and ML planes; standard width | Metaphyso-diaphyseal | Most commonly used overall (~38-60% of cementless stems in registries) | Anthology, Profemur |
| Type B3 - Quadrangular taper (double wedge, broad) | Wider version of B2 | Metaphyso-diaphyseal | Better for large/wide canals | - |
| Type C1 - Fit and fill (anatomic, standard) | Fills metaphysis in 3D | Metaphyseal | Designed to match proximal femoral anatomy closely | AML, Solution |
| Type C2 - Fit and fill (anatomic, modular) | C1 + modular neck/body | Metaphyseal | Adjustable offset, version, and leg length | SROM, ZMR |
| Type C3 - Fit and fill (anatomic, short) | Short fit-and-fill design | Metaphyseal only | Bone-conserving; newer concept | Metha |
| Type D - Conical | Cylindrical-conical taper | Diaphyseal | Fixes distally in diaphysis; used in revision or deformed femurs | Wagner cone |
| Type E - Cylindrical | Straight cylindrical with porous coating | Diaphyseal | Press-fit in diaphysis; full coating needed | AML (fully coated) |
| Type F - Calcar-guided short stem | Ultra-short, metaphyseal only | Metaphyseal | Bone-conserving; preserves femoral neck | Optimys, Nanos |
C. Classification by Stem Length
| Length | Use |
|---|---|
| Ultra-short | Bone conservation; minimal invasive surgery |
| Short | Primary THA with good bone stock |
| Traditional/Standard | Most primary THA |
| Long | Bypass cortical defects, periprosthetic fractures |
| Ultra-long/Revision | Significant bone loss, revision THA |
D. Other Design Features
Collar vs. Collarless
- Collared: Load sharing through calcar; may reduce stress shielding proximally; prevents subsidence
- Collarless: Lighter; designed for taper-slip or press-fit; no calcar contact required
Modularity
- Monobloc (one-piece): Neck angle and offset fixed; simpler, fewer interfaces
- Modular neck: Interchangeable neck segments allow adjustment of anteversion, offset, leg length intraoperatively
- Modular body: Proximal and distal bodies separate - useful in revision THA
Surface Treatment (Cementless)
| Treatment | Mechanism | Fixation Type |
|---|---|---|
| Porous beads (sintered) | Bone ingrowth into bead interstices | Ingrowth |
| Fiber metal mesh | Bone ingrowth into mesh | Ingrowth |
| Trabecular metal (tantalum) | High porosity (80%), very low modulus | Ingrowth |
| Hydroxyapatite (HA) coating | Osteoconductive; accelerates bone ongrowth | Ongrowth |
| Grit-blasting | Rough surface; bone ongrowth | Ongrowth |
Materials
- Stainless steel (historical, first generation)
- Cobalt-chrome (CoCr): High strength, stiff; used for monobloc stems
- Titanium alloy (Ti-6Al-4V): Lower modulus (closer to bone - less stress shielding); better for cementless; most common today
PART 2: ACETABULAR CUPS
A. Classification by Fixation Method
1. Cemented All-Polyethylene Cup
- Single-piece UHMWPE cup cemented directly into prepared acetabulum
- Original Charnley design
- Now largely abandoned - higher loosening rate than cementless at >10 years
- Still used in elderly patients (>80 years) with limited activity demands
2. Cementless Modular Cup (Metal Shell + Liner) - Current Standard
- Outer metal shell: Hemispherical titanium or CoCr - press-fit with biological fixation
- Inner liner: Snaps/locks into shell - articulates with femoral head
- Hemispherical press-fit (1-2 mm larger than reamed acetabulum)
- Porous coating / HA coating on outer surface
- Supplementary screws (usually 1-3) in superior/posterior dome for additional fixation
B. Types of Acetabular Liners
| Liner Type | Material | Advantages | Disadvantages |
|---|---|---|---|
| Standard polyethylene | Conventional UHMWPE | Cheap, proven | Higher wear rate; osteolysis risk |
| Highly cross-linked polyethylene (HXLPE) | Cross-linked UHMWPE | 50-80% less wear than conventional; current gold standard | Slightly more brittle; controversial in large heads |
| Ceramic | Alumina or zirconia | Very low wear rate | Expensive; risk of fracture; squeaking |
| Metal | CoCr | Hard-on-hard, low wear | ALTR (adverse local tissue reaction); ion release; declining use |
| Elevated rim | HXLPE with raised posterior rim | Reduces posterior dislocation risk | Reduces ROM; impingement risk on opposite side |
| Dual mobility | Inner poly ball + outer metal head inside outer shell | Anti-dislocation - two articulations | Larger acetabular component needed |
C. Special Acetabular Cup Designs
Dual Mobility Cup
- Two articulating surfaces: small femoral head inside large polyethylene ball, inside metal shell
- Dramatically reduces dislocation risk
- Preferred in revision THA, high dislocation risk patients, neuromuscular disease
Constrained Liner
- Locks the femoral head inside the cup mechanically
- Used when abductors are deficient or recurrent dislocation cannot be controlled
- High edge loading - risk of loosening if used in wrong patients
Trabecular Metal (Tantalum) Cup
- Used in revision THA with bone defects
- Highly porous (80%) - excellent bone ingrowth
- Can augment with tantalum "bullets" or wedges for large defects
D. Acetabular Cup Positioning - Lewinnek Safe Zone
- Inclination (abduction): 40° ± 10° (30-50°)
- Anteversion: 15° ± 10° (5-25°)
Summary - Choosing the Right Implant
| Patient | Preferred Stem | Preferred Cup |
|---|---|---|
| Young, active, good bone stock (Dorr A/B) | Cementless press-fit (Type B2 or A) | Cementless modular + HXLPE liner |
| Elderly, osteoporotic (Dorr C) | Cemented polished taper (Exeter) | Cementless modular cup (cemented cup if very elderly) |
| Revision THA | Long cementless modular stem (Type D/E) | Trabecular metal cup ± augments |
| High dislocation risk | Any stem | Dual mobility cup |
| Recurrent dislocation | Any stem | Constrained liner |
cemented vs uncemented vs hybrid thr
cemented vs cementless vs hybrid total hip replacement comparison outcomes indications complications registry data
https://aoj.amegroups.org/article/view/3848/html
Cemented vs. Cementless vs. Hybrid THA
1. Definitions
| Type | Femoral Stem | Acetabular Cup |
|---|---|---|
| Fully Cemented | Cemented (PMMA) | Cemented (PMMA) |
| Fully Cementless | Press-fit / biological ingrowth | Press-fit / biological ingrowth |
| Hybrid | Cemented stem + Cementless cup | (most common combination) |
| Reverse Hybrid | Cementless stem + Cemented cup | (less common, mostly historical) |
2. Principles of Fixation
Cemented THA
- PMMA acts as a grout - fills the space between implant and bone, providing immediate mechanical interlock
- Cement is not a glue - it transfers loads via compression
- Immediate full weight-bearing possible
- Relies on quality of cement mantle for long-term fixation
Cementless THA
- Initial stability by press-fit (interference fit - stem/cup 1-2 mm larger than reamed space)
- Biological fixation develops over 6-12 weeks as bone grows into/onto porous surface (ingrowth) or HA-coated surface (ongrowth)
- Protected weight-bearing may be advised for 6 weeks in some designs
- Relies on bone quality and adequate initial press-fit for long-term fixation
Hybrid THA
- Rationale: combine the proven cemented femoral stem survivorship with the superior cementless acetabular cup survivorship (cemented cups have unacceptably high long-term loosening rates)
- Currently the most commonly used construct in many national registries (Sweden, Norway, UK)
3. Indications
| Feature | Cemented | Cementless | Hybrid |
|---|---|---|---|
| Age | Elderly (>70-75 yrs) | Young/middle-aged (<65 yrs) | Middle-aged (55-75 yrs) |
| Bone quality | Poor - osteoporotic (Dorr C) | Good (Dorr A/B) | Moderate |
| Activity level | Low demand | High demand, active | Moderate demand |
| Dorr type | Type C (stovepipe) | Type A/B | Type B |
| Hip fracture | Preferred (elderly) | Avoid in elderly with poor bone | Not standard |
| Revision THA | Avoid (higher failure with cement in revision) | Preferred | Possible |
| Bone deformity / dysplasia | Adaptable | May be difficult to achieve press-fit | Depends |
4. Advantages and Disadvantages
Cemented THA
- Immediate, reliable fixation regardless of bone quality
- Full weight-bearing immediately (no ingrowth waiting period)
- Lower cost of implants
- Lower risk of intraoperative periprosthetic fracture (0.23% vs 3.0% for cementless - Abdel et al.)
- Better survivorship in elderly (>75 years) and poor bone stock
- Antibiotic-loaded cement possible - reduces infection risk
- Shorter surgical time (no complex press-fit sizing)
- Bone Cement Implantation Syndrome (BCIS): Fat, marrow, cement monomer embolize into circulation during canal pressurization → hypotension, hypoxia, arrhythmia, cardiac arrest - potentially fatal, especially in cardiopulmonary disease
- Longer operative time (mixing, pressurization)
- Cement aging and fatigue over time - microfractures in mantle → loosening
- Poor performance in young/active patients - cyclic loading causes early cement fatigue
- Once loosened, revision is harder - cement removal is technically demanding and destroys bone
- Thermal necrosis possible from exothermic PMMA reaction
- No bone stock preservation benefit
Cementless THA
- No BCIS risk - major advantage in cardiorespiratory compromise
- Preserves bone stock - easier future revision (remove stem without cement)
- Better survivorship in young/active patients (<65 years) - no cement fatigue
- Faster to implant (no mixing, waiting for polymerization)
- Better long-term performance in good bone stock
- Lower cost for revision if needed (less bone destruction)
- Intraoperative periprosthetic fracture risk significantly higher (3% vs 0.23%) - especially in Dorr C / osteoporotic bone
- Thigh pain (10-20%) - diaphyseal fixation stems transmit loads to distal cortex causing pain; usually resolves with bony ingrowth
- Stress shielding - proximal femur load-bypassed → proximal bone resorption over time
- Higher cost of implants
- Initial fixation depends on precise surgical technique (press-fit)
- Higher early revision rate in elderly (>75 years) - inadequate press-fit in soft osteoporotic bone
- Requires minimum 6-week bone ingrowth period for secure fixation
Hybrid THA
- Combines best of both worlds: cemented stem survivorship + cementless cup survivorship
- Avoids cemented cup (highest long-term acetabular loosening rate)
- Lowest revision rate across most age groups in registry data (particularly 55-74 years)
- Eliminates BCIS risk from acetabular cement pressurization
- Avoids thigh pain / stress shielding of cementless stems
- Two different techniques required - longer learning curve
- Not ideal at extremes of age (very young or very old)
- Reverse hybrid (cementless stem + cemented cup) has generally poor outcomes - now largely abandoned
5. Registry Data and Outcomes (by Age Group)
| Age Group | Best Revision Rate | Notes |
|---|---|---|
| < 55 years | Cementless stem | Lowest revision rate; bone ingrowth superior in young active patients |
| 55 - 74 years | Hybrid | Hybrid consistently shows lowest revision rate in this age group |
| ≥ 75 years | Cemented | Cementless has unacceptably high revision rate in elderly (3.8% vs 3.0%) |
- England & Wales Registry (14 years): Cemented 4.88% revision < Hybrid 5.38% < Cementless 8.9%
- However hybrid had lowest aseptic loosening rate
- NARA: Periprosthetic fracture was more common revision cause for cementless (27%) vs cemented
- Norwegian Register: When analyzing modern implants only (2006-2016), no significant difference between fixation methods - modern cementless technology has closed the gap
6. Global Trends
| Country | Dominant Construct | Trend |
|---|---|---|
| UK / Scandinavia | Cemented / Hybrid | Hybrid increasing |
| USA / Australia | Cementless | Rapidly increasing cementless use |
| Germany | Cementless | Predominantly cementless |
| New Zealand | Mixed | Hybrid growing rapidly |
- The "cementless paradox" - despite higher revision rates in registries, cementless use has increased dramatically in many countries (driven by surgeon training, US market preference, belief in bone preservation)
- Modern cementless designs with HA coating and improved geometry are narrowing the survivorship gap with cemented/hybrid constructs
7. Quick Decision Guide
Patient >75 years or Dorr C (osteoporosis) → Cemented THA
Patient <55 years, active, good bone stock → Cementless THA
Patient 55-74 years, moderate activity → Hybrid THA (cemented stem + cementless cup)
High cardiovascular/respiratory risk → Avoid cemented (BCIS risk) → Cementless/Hybrid
Revision THA → Cementless (preserve bone, avoid cement in revision bed)
Hip fracture, elderly → Cemented (immediate WB, BCIS precautions taken)