this pdf is made by you now teach me
cd /home/daytona/workspace/attachments/e63f2e6a-c6e1-42f6-a0af-6df231750718/ && python3 -c " import pdfplumber pdf_path = 'Ive now read all 35 slides Here is a full organize.pdf' with pdfplumber.open(pdf_path) as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() print(f'--- PAGE {i+1} ---') print(text[:500] if text else '[no text]') print() "
cd /home/daytona/workspace/attachments/e63f2e6a-c6e1-42f6-a0af-6df231750718/ && python3 -c " import pdfplumber pdf_path = 'Ive now read all 35 slides Here is a full organize.pdf' with pdfplumber.open(pdf_path) as pdf: for i, page in enumerate(pdf.pages): text = page.extract_text() print(f'=== PAGE {i+1} ===') print(text if text else '[no text]') print() "
🧠 Muscle Plasticity in Response to Electrical Stimulation - Full Lesson
1. History & Background
2. Definition
Skeletal muscle plasticity = the modification of skeletal muscle structures in response to environmental change.
- Dynamic ability to adapt when use increases
- In response to demands, the structure, biochemical, and physiological characteristics all change
3. Structure of Skeletal Muscle (The Hierarchy)
Muscle
└─ Fascicles
└─ Muscle fibers (cells)
└─ Myofibrils
└─ Thick (myosin) & Thin (actin) filaments
- Epimysium - outer covering of the whole muscle
- Perimysium - surrounds each fascicle
- Endomysium - wraps individual fibers
- Sarcolemma - the muscle cell membrane
- Sarcoplasmic reticulum (SR) - the calcium store (very important later!)
- Sarcomere - the functional contractile unit, bounded by Z-discs, containing actin (thin) and myosin (thick) filaments
4. Types of Muscle Fibres
| Property | Type I (Slow Oxidative) | Type IIA (Fast Oxidative-Glycolytic) | Type IIB (Fast Glycolytic) |
|---|---|---|---|
| Fiber/motor unit size | Small | Intermediate | Large |
| Mitochondria & capillaries | Many | Many | Few |
| Myoglobin content | High (red) | High (red) | Low (white) |
| Glycogen content | Low | Intermediate | High |
| Main ATP source | Oxidative phosphorylation | Oxidative phosphorylation | Anaerobic glycolysis |
| Rate of fatigue | Slow | Intermediate | Fast |
| Myosin ATPase activity | Low | High | High |
| Contractile speed | Slow | Fast | Fast |
| Best for | Long-distance running | 400m/800m | Short sprints |
| Examples | Postural back muscles | Major leg muscles | Extraocular eye muscles |
- Type I = "I run marathons" (slow, endurance, oxygen-based)
- Type IIB = "II-Blaze" (fast, explosive, burns out quick)
- Type IIA = the middle ground
5. Electrical Stimulation - The Key Principle
- Slow twitch fibres respond to low frequency currents
- Fast twitch fibres respond to high frequency bursts
6. Chronic Low-Frequency Stimulation (CLFS) - The Landmark Finding
Indirect electrical stimulation with tonic, low frequency current converts fast-twitch muscle into slow-twitch muscle.
What shifts fibres Fast → Slow?
- Increased neuromuscular activity
- Chronic electro-stimulation
- Endurance training
- Hyper-excitability / Myotonia
What shifts fibres Slow → Fast? (the reverse)
- Hypoxia
- Microgravity
- Immobilization
- Prolonged bed rest
- Experimental denervation
7. Time Course of Fibre Transformation
- Contractile property changes
- Metabolic changes
- Circulatory changes
- Structural changes
8. Components Modified by Stimulation
- Architecture of the muscle overall
- Fibre type distribution
- Fibre diameter
- Fibre length
- Tendon length
- Myosin heavy chain profile (very significant - changes the molecular identity)
- Mitochondrial distribution
- Capillary density
9. The Timeline of Changes After CLFS (Critical!)
⏱ 2-3 Hours
- Earliest observable change: swelling in the sarcoplasmic reticulum (SR) membrane network
- Significance is not fully understood, but it is consistently observed
⏱ 2-12 Days
- Size and number of mitochondria increase
- Volume % of mitochondria increases
- Oxidative enzyme activity increases
- Blood flow increases → greater metabolic activity
- Muscle fatigability begins to decrease
- Angiogenesis (more capillaries per mm²)
- ↑ Total blood flow
- ↑ Total oxygen consumption
- ↑ Oxidative enzymes and metabolic activity
- ↓ Muscle fatigability
⏱ 14 Days
- Z band increases in width
- Decrease in calcium ATPase amount and activity
⏱ 28 Days
- Myosin profile alters - different myosin monomers incorporate into single filaments
- Fast light chains (LC1f, LC2f, LC3f) → replaced by slow light chains (LC1s, LC2s)
- Heavy chain profile altered
- Fast fibres become structurally more like slow fibres
- Muscle mass and fibre area decrease
- Z band reaches full width
⏱ ~8 Weeks (End of Transformation)
- Z band is now the full width of a normal slow-contracting muscle
- Density of the T-system has decreased
- The transformed fast muscle is indistinguishable from a normal slow muscle
10. Summary of All CLFS Changes
- Slowing of contraction and relaxation time-courses
- Increased fatigue resistance
- Reduction in muscle bulk and tetanic tension (first shown in rabbit EDL and TA muscles)
- Loss of bulk = reduction in diameter of the largest, most fatigable fibres
- Profound alterations in gene expression
- Complete transformation of muscle fibre phenotype
11. Key Research Studies
| Study | Model | Key Finding |
|---|---|---|
| Trumble, Duan & Magovern | Rabbit latissimus dorsi, 6/12 weeks CLFS | ↑ endurance, ↑ type I collagen, ECM remodeling |
| Bruton (2002) | Literature review | Muscle adapts to training/detraining; genotype influences phenotypic response |
| Lotri-Koffi et al (2019) | Mouse NMES vs sham, 2.5 weeks | ↑ muscle mass, ↑ insulin sensitivity; useful in chronic disease |
| Tsutaki, Ogasawara et al (2013) | Rat gastrocnemius, HFS (100 Hz) vs LFS (10 Hz) | LFS recruits type II fibers regardless of frequency; stimulation without high force causes hypertrophy |
| Pette & Vrbová (2017) | Review | All essential components undergo reversible fast → slow transformation |
| Schnyder, Kupr & Handschin (2017) | Mini-review | Coregulators drive metabolic and myofibrillar plasticity; HDAC inhibition enhances endurance |
| Nuhr, Pette et al (2004) | CHF patients, CLFS of thigh | CLFS counteracts muscle deterioration in heart failure; increases exercise capacity |
12. Quick-Review Q&A
| Question | Answer |
|---|---|
| Who coined "Plasticity of Muscle"? | John Eccles, 1979 |
| What does CLFS do to fast-twitch muscle? | Converts it to slow-twitch phenotype |
| How long does full transformation take? | ~8 weeks (with 8-24 h/day stimulation) |
| What is the first change observed? | SR membrane swelling within 2-3 hours |
| When do mitochondria increase? | Within 2-12 days |
| What happens to myosin at 28 days? | Fast light chains (LC1f/2f/3f) → slow (LC1s/2s); phenotype shifts |
| What does Z band width indicate? | Full width = complete fast-to-slow transformation |
| What causes Slow → Fast shift? | Immobilization, bed rest, hypoxia, microgravity, denervation |
| Clinical applications? | Counteract atrophy in heart failure, insulin resistance, aging, disuse |
How to Study This
- The fibre type comparison table (Type I vs IIA vs IIB) - know every row cold
- The CLFS timeline (2-3 hrs → 2-12 days → 14 days → 28 days → 8 weeks) - know what changes when
- Bidirectional plasticity - what pushes Fast→Slow and what pushes Slow→Fast
Make a visual summary poster of muscle transformation
A detailed educational science poster titled "Muscle Plasticity & Fibre Transformation" with the following sections clearly laid out: TOP SECTION - Title banner: "MUSCLE PLASTICITY IN RESPONSE TO ELECTRICAL STIMULATION" with subtitle "From Fast-Twitch to Slow-Twitch: The Complete Transformation" LEFT COLUMN - "FIBRE TYPE COMPARISON TABLE" with 3 columns comparing Type I (Slow Oxidative), Type IIA (Fast Oxidative-Glycolytic), Type IIB (Fast Glycolytic). Rows: Size (Small / Medium / Large), Mitochondria (Many / Many / Few), Fatigue Rate (Slow / Medium / Fast), ATP Source (Oxidative / Mixed / Glycolysis), Best For (Marathon / 800m / Sprints). Use color coding: red for Type I, orange for Type IIA, blue for Type IIB. CENTER - A large illustrated arrow pointing RIGHT labeled "CLFS (Chronic Low-Frequency Stimulation)" showing transformation: Fast-twitch muscle cell on the left → Slow-twitch muscle cell on the right. Below the arrow, smaller arrows showing reverse: "Slow → Fast" caused by hypoxia, bed rest, immobilization, denervation. RIGHT COLUMN - "CLFS TRANSFORMATION TIMELINE" as a vertical timeline with icons: - Clock icon: "2-3 Hours: Sarcoplasmic Reticulum swelling (earliest change)" - Microscope icon: "2-12 Days: Mitochondria increase, angiogenesis, fatigue resistance begins" - DNA icon: "14 Days: Z-band widens, Ca²⁺ ATPase decreases" - Protein icon: "28 Days: Myosin light chains shift Fast→Slow (LC1f→LC1s), muscle mass decreases" - Checkmark icon: "8 Weeks: Full transformation — muscle indistinguishable from normal slow-twitch" BOTTOM SECTION - Two boxes side by side: Left box "Fast → Slow Triggers": increased activity, CLFS, endurance training, myotonia Right box "Slow → Fast Triggers": hypoxia, microgravity, immobilization, bed rest, denervation Footer: "John Eccles coined 'Plasticity of Muscle' — 1979 | Brown (1984) landmark CLFS finding" Clean scientific poster style, white background, bold headings, color-coded sections, professional medical illustration aesthetic
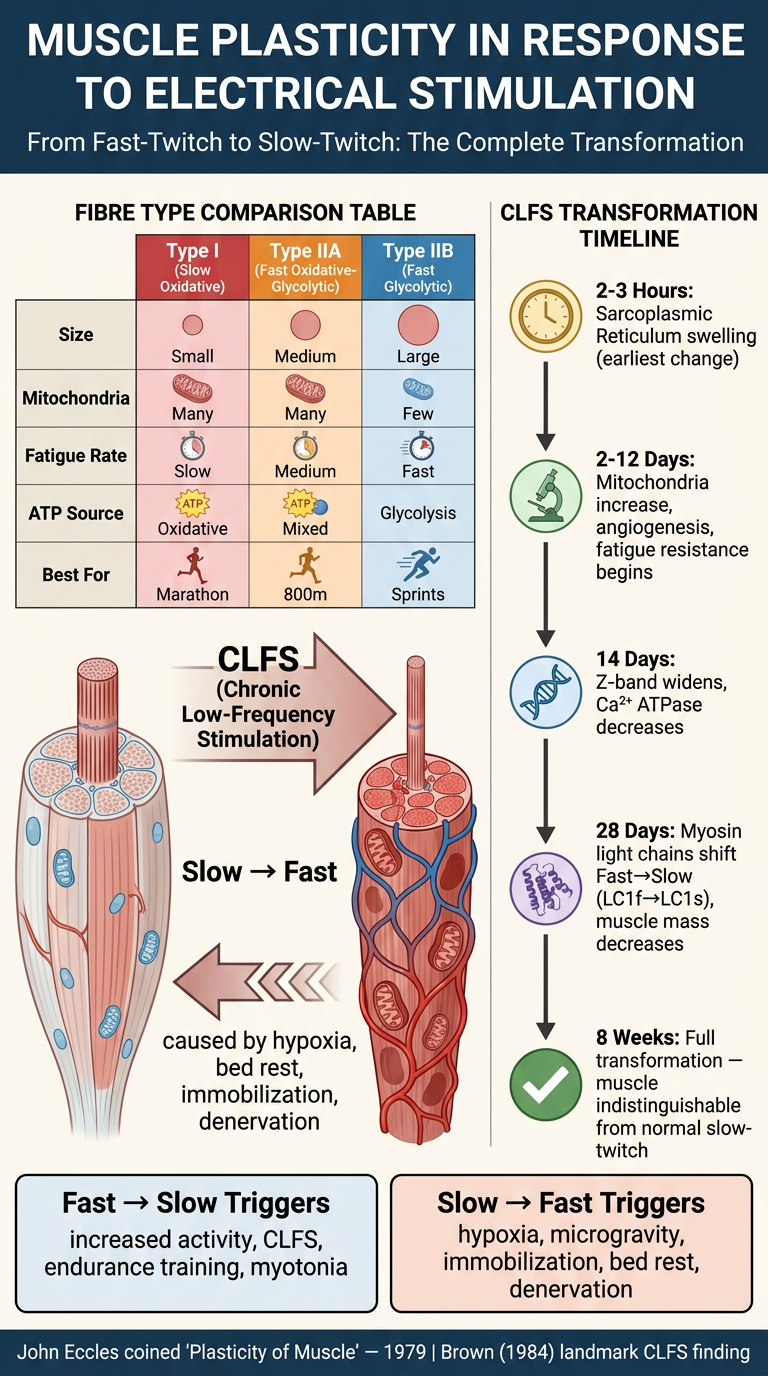
- Fibre type comparison (Type I / IIA / IIB) color-coded by speed and fatigue
- The central CLFS transformation arrow showing Fast → Slow conversion
- The full 8-week timeline with each stage of change (SR swelling → mitochondria → Z-band → myosin → complete transformation)
- Bidirectional plasticity - what drives each direction
- Key attribution (Eccles 1979, Brown 1984)