Fick's principle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here is a complete, textbook-grounded explanation of Fick's principle.
Fick's Principle
The Core Statement
Fick's principle (Adolf Fick, 1870) is based on conservation of mass: the amount of a substance taken up or released by an organ equals the product of blood flow to that organ and the arteriovenous concentration difference of that substance.
"The Fick principle states that there is conservation of mass... In the steady state, the rate of O₂ consumption by the body must equal the amount of O₂ leaving the lungs in the pulmonary vein minus the amount of O₂ returning to the lungs in the pulmonary artery."
- Costanzo Physiology, 7th Ed.
1. Application to Cardiac Output (Most Important Use)
The most common application is measuring cardiac output (CO) using oxygen as the indicator substance.
Formula
$$\text{CO (L/min)} = \frac{\dot{V}{O_2}}{C{aO_2} - C_{vO_2}}$$
| Variable | Meaning |
|---|---|
| VO₂ | Total body O₂ consumption (mL/min) |
| CaO₂ | Arterial O₂ content (mL O₂/mL blood) - sampled from any systemic artery |
| CvO₂ | Mixed venous O₂ content (mL O₂/mL blood) - sampled from pulmonary artery or right ventricle |
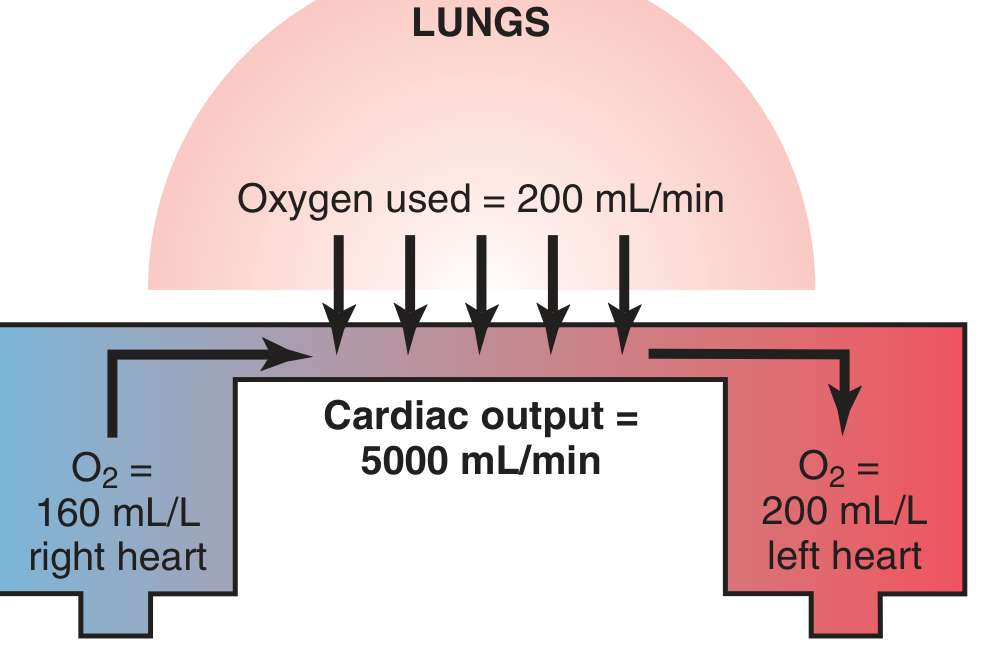
Numerical Example (from Guyton & Hall / Costanzo)
- O₂ absorbed by lungs: 200 mL/min
- Arterial O₂ content (left heart): 200 mL/L blood
- Venous O₂ content (right heart): 160 mL/L blood
- A-V difference: 200 - 160 = 40 mL/L
- CO = 200 ÷ 40 = 5 L/min
2. Practical Measurement - Cardiac Catheterization
During right heart catheterization:
- Mixed venous blood is sampled from the pulmonary artery (or right ventricle) via a catheter inserted through the brachial or subclavian vein
- Arterial blood is sampled from any systemic artery
- VO₂ can be measured directly using a metabolic cart (measuring O₂ disappearance from expired air) = Direct Fick method, or estimated using a nomogram (125 mL/min × BSA) = Indirect Fick method
The direct Fick is considered the gold standard for CO measurement. Harrison's notes it is "more reliable in the presence of tricuspid regurgitation and in low-output states" compared to thermodilution.
If VO₂ is not measured directly:
- Estimated VO₂ = 125 mL O₂/min × body surface area
- A-V O₂ difference = Hb (g/100 mL) × 1.36 (mL O₂/g Hb) × 10 × fractional O₂ saturation difference
3. Application to Renal Plasma Flow (RPF)
Fick's principle also applies to the kidney to measure renal plasma flow, using PAH (para-aminohippuric acid) as the indicator.
Conservation of mass at the kidney:
$$[\text{RA}]{\text{PAH}} \times \text{RPF} = [\text{RV}]{\text{PAH}} \times \text{RPF} + [\text{U}]_{\text{PAH}} \times \dot{V}$$
Solving for RPF:
$$\text{RPF} = \frac{[\text{U}]{\text{PAH}} \times \dot{V}}{[\text{RA}]{\text{PAH}} - [\text{RV}]_{\text{PAH}}}$$
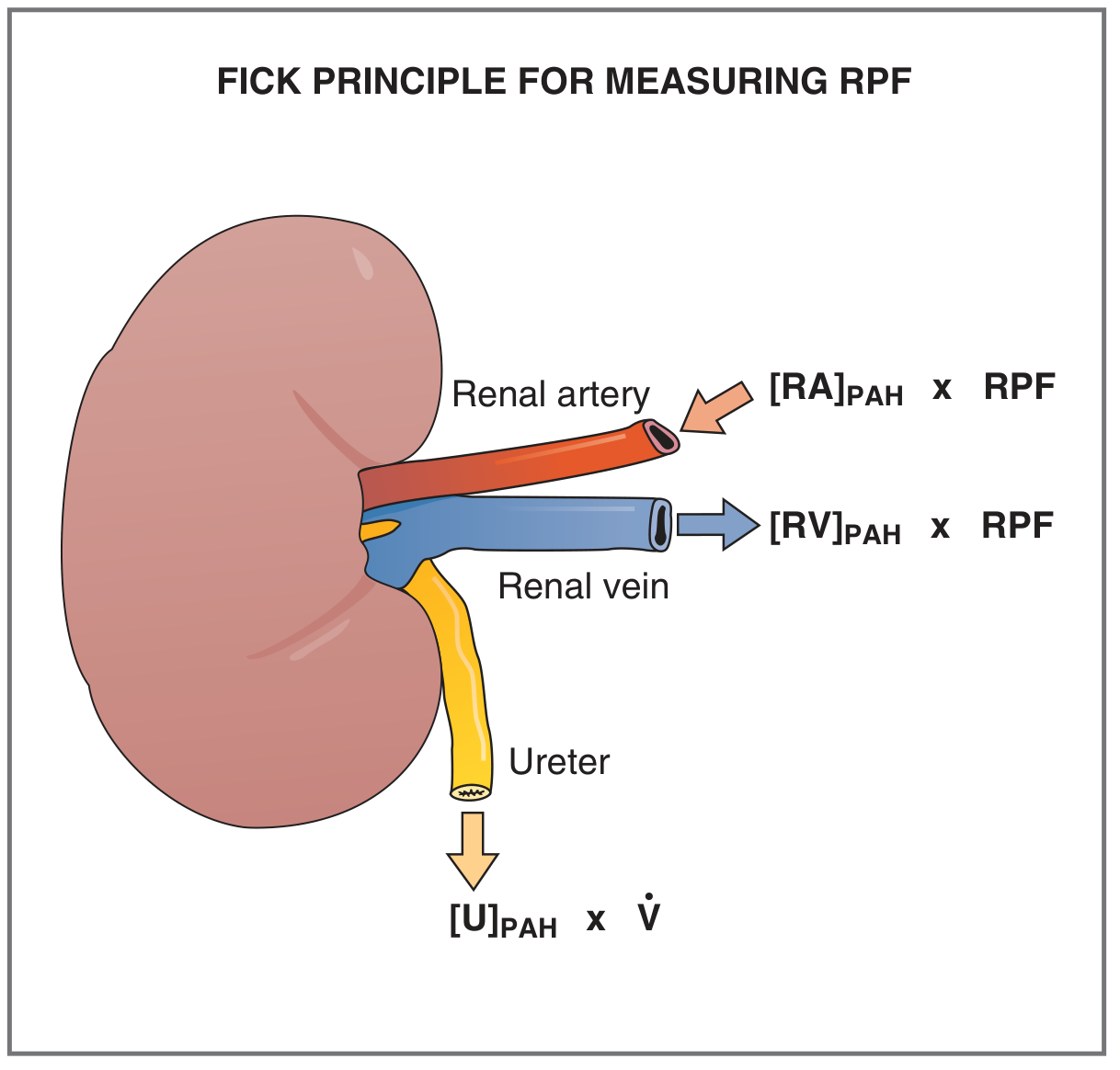
Why PAH? It is neither metabolized nor synthesized by the kidney; the kidneys nearly completely extract it (by filtration + secretion), making the renal vein concentration ~0. This maximizes the denominator and allows accurate measurement. (Costanzo Physiology, 7th Ed.)
4. General Organ Blood Flow (Conceptual Extension)
The principle applies to any organ:
$$\text{Organ blood flow} = \frac{\text{Rate of substance uptake/release by organ}}{\text{Arteriovenous concentration difference}}$$
For example:
- Renal blood flow = O₂ consumed by kidney ÷ (renal arterial O₂ - renal venous O₂)
- Brain perfusion, hepatic blood flow, etc. can all be estimated the same way
5. Indicator Dilution - the Fick-Derived Methods
All indicator-dilution methods (including thermodilution) are mathematical extensions of Fick's principle. In thermodilution, cold saline is the "indicator," and temperature change in the pulmonary artery is measured by a thermistor to calculate CO. (Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.)
Summary Table
| Application | Substance Used | Blood Flow Measured |
|---|---|---|
| Cardiac catheterization | Oxygen (O₂) | Cardiac output |
| Renal physiology | PAH | Renal plasma flow |
| Thermodilution | Temperature (cold saline) | Cardiac output |
| Any organ | Any non-metabolized indicator | Organ blood flow |
Sources:
- Costanzo Physiology, 7th Ed. - core derivation and RPF application
- Guyton and Hall Textbook of Medical Physiology - illustrated numerical example
- Harrison's Principles of Internal Medicine, 22E - clinical context in cardiac catheterization
- Fuster and Hurst's The Heart, 15th Ed. - direct vs. indirect Fick, gold standard status
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed. - anesthetic/perioperative application
Physiological basis of ficks principle
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Now I have all the material needed for a comprehensive, physiologically grounded answer.
Physiological Basis of Fick's Principle
1. The Foundational Law: Conservation of Mass
Fick's principle is built entirely on one physical law - conservation of mass: in a system at steady state, the amount of a substance entering a compartment must equal the amount leaving it. No substance appears or disappears from nowhere.
Applied to the cardiorespiratory system:
"The Fick principle states that there is conservation of mass, a concept that can be applied to the utilization of O₂ by the body."
- Costanzo Physiology, 7th Ed.
In the steady state, the rate at which O₂ is picked up by blood in the lungs must equal the rate at which the tissues consume it. Neither accumulation nor depletion of O₂ is occurring anywhere in the system.
2. The Oxygen Transport Chain - the Physiological Framework
To understand the basis, you must trace the complete oxygen pathway:
Atmosphere → Lungs (alveoli) → Pulmonary capillaries
→ Left heart → Systemic arteries → Tissues (consumption)
→ Systemic veins → Right heart → Pulmonary arteries → Lungs
At any cross-section of this circuit, three things are happening simultaneously:
| Event | Site | Physiological variable |
|---|---|---|
| O₂ loading | Pulmonary capillaries | CaO₂ (arterial O₂ content) rises |
| O₂ bulk transport | Heart/vessels | Cardiac output (Q) carries the O₂ |
| O₂ unloading | Tissue capillaries | CvO₂ (venous O₂ content) falls |
The amount of O₂ delivered to tissues per minute = Q × CaO₂
The amount of O₂ returning unused per minute = Q × CvO₂
Therefore the amount consumed by tissues per minute:
$$\dot{V}{O_2} = Q \cdot C{aO_2} - Q \cdot C_{vO_2} = Q \cdot (C_{aO_2} - C_{vO_2})$$
Rearranging to solve for cardiac output:
$$\boxed{Q = \frac{\dot{V}{O_2}}{C{aO_2} - C_{vO_2}}}$$
This is the Fick equation. The physiology justifies every term. (Medical Physiology, Boron & Boulpaep; Costanzo Physiology, 7th Ed.)
3. The Steady-State Assumption - Why It Matters
The entire principle requires steady state. This means:
- Cardiac output of the left and right hearts must be equal (no net blood pooling anywhere)
- O₂ consumption by tissues is constant (no sudden changes in metabolic rate)
- O₂ content of arterial and venous blood is not changing over time
If the system is not at steady state (e.g., during exercise onset, cardiac arrest, or rapid hemorrhage), the principle introduces error. This is why measurements are taken at rest or after equilibration.
"The fundamental assumption is that, in the steady state, the cardiac output of the left and right ventricles is equal."
- Costanzo Physiology, 7th Ed.
4. Physiological Components in the Equation
a. Oxygen Consumption (VO₂)
This reflects the metabolic demand of all tissues combined. Normally ~250 mL/min in a 70-kg adult at rest. It is the net O₂ "extracted" from the circulation. It can be:
- Measured directly at the mouth using a metabolic cart (expired gas analysis)
- Estimated as 125 mL O₂/min × body surface area (indirect Fick)
b. Oxygen Content (CaO₂ and CvO₂)
Oxygen is carried in blood in two forms - the vast majority bound to hemoglobin, and a small amount dissolved in plasma:
$$C_{aO_2} = (1.34 \times Hb \times SaO_2) + (0.0031 \times PaO_2)$$
| Component | Role |
|---|---|
| 1.34 mL O₂/g Hb | Hüfner's constant - O₂ binding capacity of hemoglobin |
| Hb (g/100 mL) | Hemoglobin concentration |
| SaO₂ (%) | % saturation (from oximeter or blood gas) |
| 0.0031 × PaO₂ | Dissolved O₂ (minor, ~1.5% of total) |
Normal values (Goldman-Cecil Medicine):
- Arterial O₂ content (CaO₂): ~20 mL/100 mL blood (SaO₂ ~95%, Hb ~15 g/100 mL)
- Mixed venous O₂ content (CvO₂): ~15 mL/100 mL blood (SvO₂ ~75%)
- A-V O₂ difference: ~5 mL/100 mL blood (= 50 mL/L)
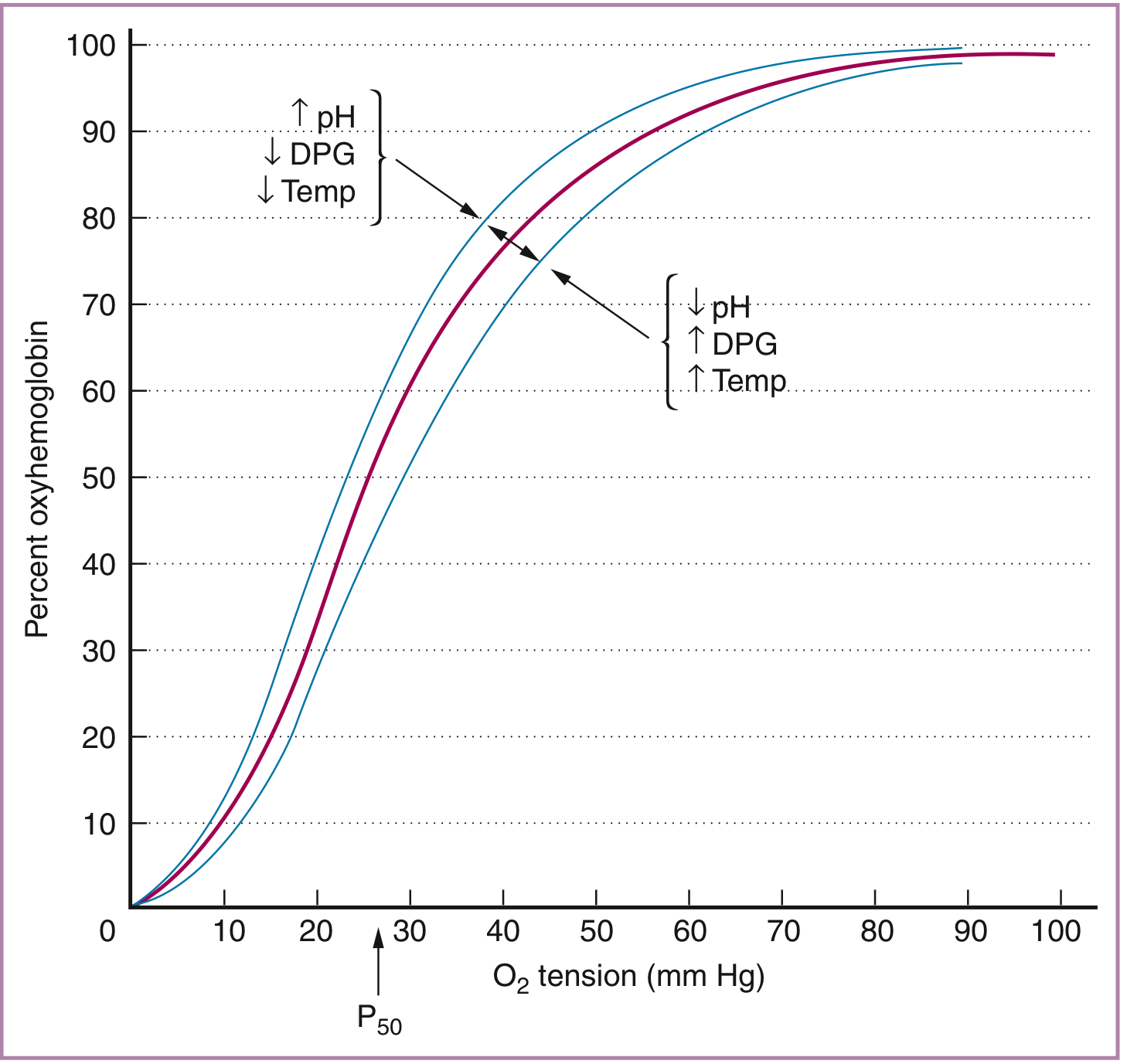
The oxyhemoglobin dissociation curve governs how much O₂ is loaded and unloaded - its sigmoidal shape allows efficient O₂ delivery across a range of tissue PO₂:
c. Mixed Venous Blood - Why the Pulmonary Artery?
The venous blood from different organs has different O₂ content (coronary sinus blood is very desaturated; renal venous blood is relatively well-saturated). For Fick's principle to represent whole-body O₂ consumption, venous blood must be thoroughly mixed. This mixing happens in the right ventricle and pulmonary artery - hence, pulmonary artery blood = true "mixed venous" blood (SvO₂ ~75%). (Miller's Anesthesia, 10th Ed.)
5. The Fick Equation and Oxygen Delivery/Consumption Balance
Fick's principle is also the physiological underpinning of the entire DO₂/VO₂ framework used in critical care:
| Parameter | Formula | Normal |
|---|---|---|
| O₂ Delivery (DO₂) | CO × CaO₂ × 10 | ~1000 mL/min |
| O₂ Consumption (VO₂) | CO × (CaO₂ - CvO₂) × 10 | ~250 mL/min |
| O₂ Extraction Ratio (OER) | VO₂ / DO₂ | ~25% |
| Mixed venous saturation (SvO₂) | SaO₂ - VO₂/(Q × 1.36 × Hgb) | 60-80% |
The body compensates for reduced DO₂ by increasing O₂ extraction (OER rises, SvO₂ falls). The myocardium already extracts ~75%, so the heart has almost no extraction reserve - making coronary blood flow critical. (Mulholland & Greenfield's Surgery, 7th Ed.)
Rearranging Fick's equation reveals the four determinants of SvO₂ (Miller's Anesthesia):
$$S_{v}O_{2} = S_{a}O_{2} - \frac{V\dot{O}_2}{Q \times 1.36 \times Hgb}$$
So SvO₂ falls when:
- SaO₂ falls (hypoxemia)
- VO₂ rises (fever, sepsis, exercise)
- Q falls (low cardiac output)
- Hgb falls (anemia)
6. Pulmonary Application - the "Mass Balance" at the Lung
From the lung's perspective, conservation of mass means:
O₂ added to blood by alveoli (q₂) = O₂ leaving lungs in pulmonary veins (q₃) - O₂ entering lungs in pulmonary artery (q₁)
Since q₁ + q₂ = q₃:
$$q_2 = Q \cdot C_{pvO_2} - Q \cdot C_{paO_2}$$
This is the same equation viewed from the lung side - the rate of O₂ absorbed by pulmonary capillary blood equals cardiac output times the pulmonary venous minus pulmonary arterial O₂ content. (Miller's Anesthesia, 10th Ed.)
7. Assumptions and Conditions Required for Validity
| Assumption | Physiological Rationale |
|---|---|
| Steady state | No net change in O₂ stores; VO₂ = O₂ uptake at lungs |
| Equal right and left CO | No intracardiac shunts or pulmonary AV shunts |
| Mixed venous sample from PA | Ensures blood represents all tissue beds, not just one organ |
| Hemoglobin not altered mid-measurement | Otherwise CaO₂ formula is inaccurate |
| VO₂ accurately measured | Direct measurement > estimated nomograms, especially in obese or critically ill |
The Fick method is most reliable in low-output states and when tricuspid regurgitation is present - precisely because thermodilution (which uses temperature mixing) becomes inaccurate in these situations. (Harrison's Principles, 22nd Ed.)
Summary Diagram (Conceptual)
LUNGS
O₂ absorbed = VO₂ = 250 mL/min
↓
┌───────────────────────────────────┐
│ Pulmonary artery blood │
│ (mixed venous, CvO₂ = 15 mL/dL) │
└───────────────────────────────────┘
↓ Cardiac output (Q)
┌───────────────────────────────────┐
│ Systemic arterial blood │
│ (CaO₂ = 20 mL/dL) │
└───────────────────────────────────┘
↓
TISSUES consume O₂
A-V difference = 5 mL/dL
Q = VO₂ / (CaO₂ - CvO₂)
= 250 / (20-15) mL/dL × 10
= 5000 mL/min
Sources:
- Costanzo Physiology, 7th Ed. - conservation of mass derivation, steady-state assumption
- Medical Physiology (Boron & Boulpaep) - mass balance at the lung
- Miller's Anesthesia, 10th Ed. - conservation of mass framing, SvO₂ determinants
- Goldman-Cecil Medicine - O₂ content formula and normal A-V difference
- Mulholland & Greenfield's Surgery, 7th Ed. - DO₂/VO₂/OER relationship
- Creasy & Resnik's Maternal-Fetal Medicine - O₂ consumption = CO × C(a-v)O₂
Wind kesssels vessels
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, textbook-grounded account of Windkessel vessels.
Windkessel Vessels
Origin of the Term
"Windkessel" is German for air chamber or wind chamber. The term comes from old fire-engine pumps that had a dome-shaped air chamber attached to the pump. The intermittent strokes of the pump pushed water into the rigid chamber, compressing the air inside, which then smoothed the pulsatile water jets into a near-continuous, steady stream. Otto Frank (1899) applied this analogy to the aorta and large elastic arteries, recognising they perform the same hydraulic function for the cardiovascular system.
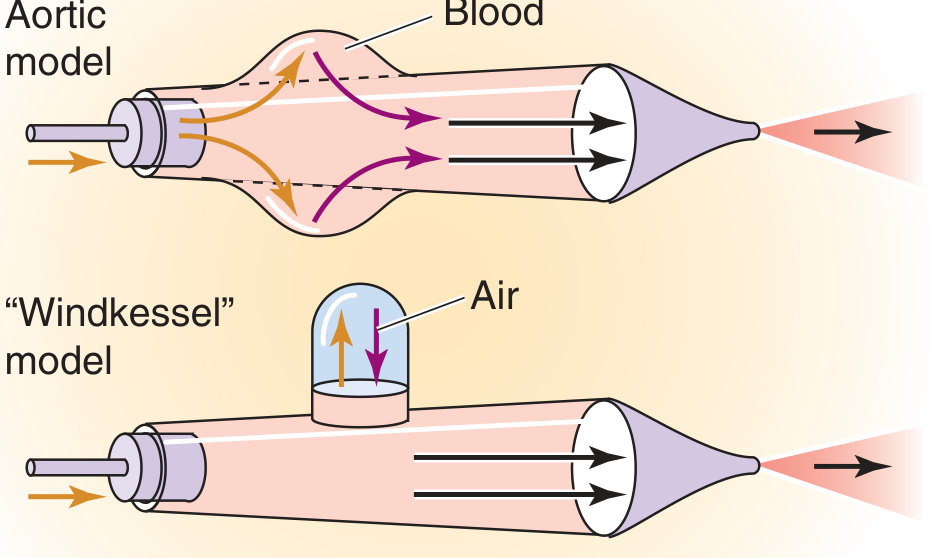
Top: The aortic model - during systole the wall expands (gold arrows), storing blood; during diastole it recoils (purple arrows), propelling blood forward. Bottom: The Windkessel analogy - the air dome stores pressure and releases it to maintain forward flow. (Medical Physiology, Boron & Boulpaep)
1. Which Vessels Are Windkessel Vessels?
Windkessel vessels = large elastic (conducting) arteries:
| Vessel | Role |
|---|---|
| Aorta | Primary Windkessel; receives the entire stroke volume |
| Pulmonary artery | Right-sided Windkessel |
| Innominate, subclavian, common carotid arteries | Major aortic arch branches |
| Iliac arteries | Distal Windkessel function |
Their walls contain abundant concentric elastin lamellae in the tunica media, arranged like tree rings, interleaved with smooth muscle cells. This gives them exceptional compliance. (Robbins & Cotran Pathologic Basis of Disease)
2. The Core Mechanism: Systole and Diastole
During Systole
The left ventricle ejects ~70 mL (stroke volume) rapidly into the aorta in ~0.3 s. The peripheral resistance vessels (arterioles) cannot accept all this blood instantly. Instead:
- The elastic walls of the aorta stretch and distend, storing roughly 50% of the stroke volume as potential energy (elastic deformation) in the vessel wall
- Aortic pressure rises to ~120 mmHg (systolic)
"The entry of blood into the arteries during systole causes the walls of these arteries to stretch and the pressure to increase to about 120 mmHg."
- Guyton & Hall, Medical Physiology
During Diastole
Once the aortic valve closes:
- The stretched elastic walls recoil, converting stored potential energy back into kinetic energy of blood flow
- This propels blood continuously through the peripheral vessels even though the heart is in diastole
- Aortic pressure falls gradually to ~80 mmHg (diastolic) - maintained by this elastic recoil, not by ventricular contraction
"After the aortic valve closes, pressure in the aorta decreases slowly throughout diastole because the blood stored in the distended elastic arteries flows continually through the peripheral vessels back to the veins."
- Guyton & Hall
The net result: a pulsatile input (systole/diastole) is converted into a near-continuous output at the tissue level. Capillary flow is largely non-pulsatile.
3. Quantitative Framework
Compliance (C)
$$C = \frac{\Delta V}{\Delta P}$$
Compliance is the volume increase per unit pressure increase. Higher compliance = more Windkessel buffering.
Pulse Pressure
$$\text{Pulse Pressure} = \text{Systolic} - \text{Diastolic} = 120 - 80 = 40 \text{ mmHg (normal)}$$
Pulse pressure is an inverse surrogate of arterial compliance:
- High compliance → aorta accommodates stroke volume with little pressure rise → narrow pulse pressure
- Low compliance (stiff aorta) → same stroke volume causes a greater pressure rise → wide pulse pressure
Arterial Compliance and Pulse Pressure
$$\text{Pulse Pressure} \approx \frac{\text{Stroke Volume}}{\text{Arterial Compliance}}$$
RC Time Constant
In the two-element Windkessel model, the arterial tree is modelled as a capacitor (compliance, C) in parallel with a resistor (peripheral resistance, R). The RC time constant = R × C, which determines how quickly pressure decays during diastole. (Fishman's Pulmonary Diseases)
4. Pulse Wave Propagation - What Happens Downstream
Because the aorta is elastic and compliant, the pressure wave travels relatively slowly and is dampened as it moves peripherally. As the wave reaches stiffer, less compliant vessels (muscular arteries):
- The wave speeds up (stiffer wall = faster propagation)
- The waveform becomes taller and narrower - peripheral systolic pressure can exceed central aortic systolic pressure
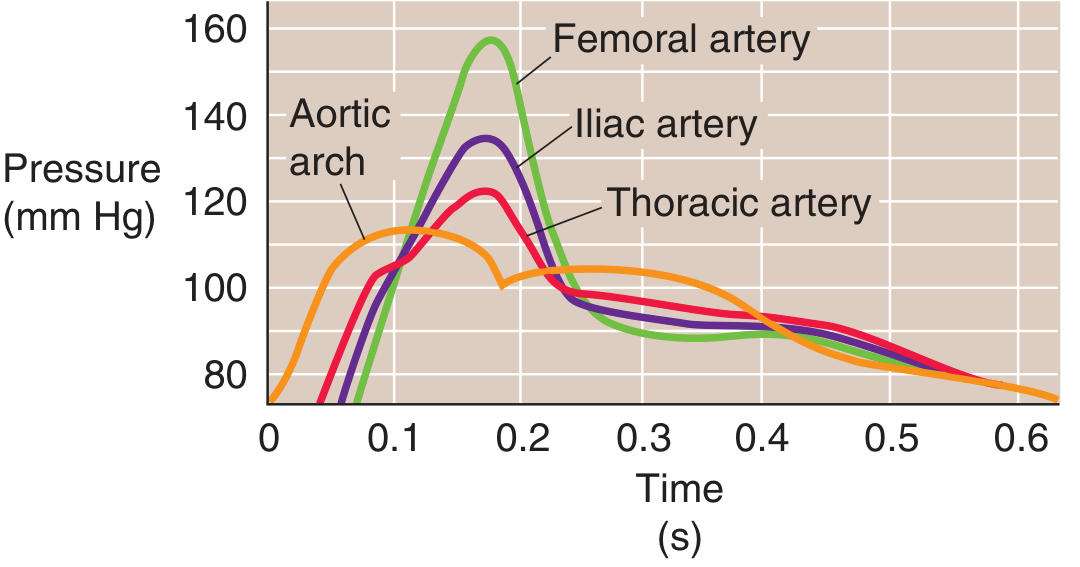
Pressure waves at four sites (10 cm intervals from aortic arch in a dog). As the wave moves downstream, peak pressure rises and the waveform narrows - a result of reduced compliance and wave reflection. (Medical Physiology, Boron & Boulpaep)
5. Structural Basis: The Elastic Artery Wall
The histological architecture of Windkessel vessels directly supports their function:
- Tunica media: concentric layers of elastin fibers + smooth muscle cells + collagen. "The high elastin content of the media allows these vessels to expand during systole and recoil during diastole." (Robbins & Cotran)
- Tunica intima: thick subendothelial layer; endothelium regulates tone via NO and other mediators
- Vasa vasorum: small vessels within the adventitia perfuse the outer wall of these large vessels
Compare to muscular arteries (medium-sized: coronary, renal), which have minimal elastin lamellae and primarily regulate flow by smooth muscle contraction.
6. Clinical and Pathophysiological Significance
Aging and Arteriosclerosis
With aging, elastin fibers fragment and are replaced by stiffer collagen:
- Arterial compliance falls
- Systolic pressure rises, diastolic pressure falls slightly
- Pulse pressure widens (isolated systolic hypertension in the elderly)
- Left ventricular afterload increases → LV hypertrophy
- Pulse wave velocity increases (aortic stiffness index)
"Aging decreases the distensibility of arteries. The decreased compliance elevates systolic pressure, slightly decreases diastolic pressure, and thus widens pulse pressure."
- Medical Physiology, Boron & Boulpaep
"In larger elastic arteries, arterial stiffness, associated with aging or disease, increases left ventricular afterload and portends a poor outcome."
- Harrison's Principles, 22nd Ed.
Aortic Aneurysm
Loss of aortic elastic tissue (elastin degradation, e.g., Marfan syndrome, atherosclerosis) removes the structural scaffolding, causing progressive dilatation - the wall can no longer withstand pulsatile forces. (Robbins & Cotran)
Pulmonary Windkessel
The pulmonary artery functions as the right-sided Windkessel. In pulmonary arterial hypertension (PAH), pulmonary arterial compliance (PAC) falls progressively, increasing RV afterload and driving RV failure. PAC = SV/PP is used to quantify this. (Fishman's Pulmonary Diseases)
7. Summary Table
| Feature | Normal Windkessel | Aged/Stiff Windkessel |
|---|---|---|
| Wall composition | Elastin-rich | Elastin reduced, collagen increased |
| Compliance | High | Low |
| Pulse pressure | ~40 mmHg | Wide (>60 mmHg) |
| Diastolic support | Good (maintained by recoil) | Reduced |
| Pulse wave velocity | Low (slower propagation) | High (faster propagation) |
| LV afterload | Normal | Increased |
| Clinical consequence | Continuous tissue perfusion | Systolic hypertension, LVH, organ damage |
Sources:
- Medical Physiology, Boron & Boulpaep - Windkessel model diagram, pressure wave propagation
- Guyton & Hall Textbook of Medical Physiology - aortic pressure curve mechanism
- Robbins & Cotran Pathologic Basis of Disease - elastic artery wall structure
- Harrison's Principles of Internal Medicine, 22nd Ed. - arterial stiffness and afterload
- Fishman's Pulmonary Diseases and Disorders - pulmonary Windkessel model and PAC
- Costanzo Physiology, 7th Ed. - compliance and pulse pressure relationship
Carotid sinus v/s carotid body
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - now I have all the material needed for a detailed comparison.
Carotid Sinus vs. Carotid Body
These two structures sit at the same anatomical landmark - the bifurcation of the common carotid artery - but perform completely different physiological roles. They are the body's primary sentinel stations for blood pressure and blood chemistry, respectively.
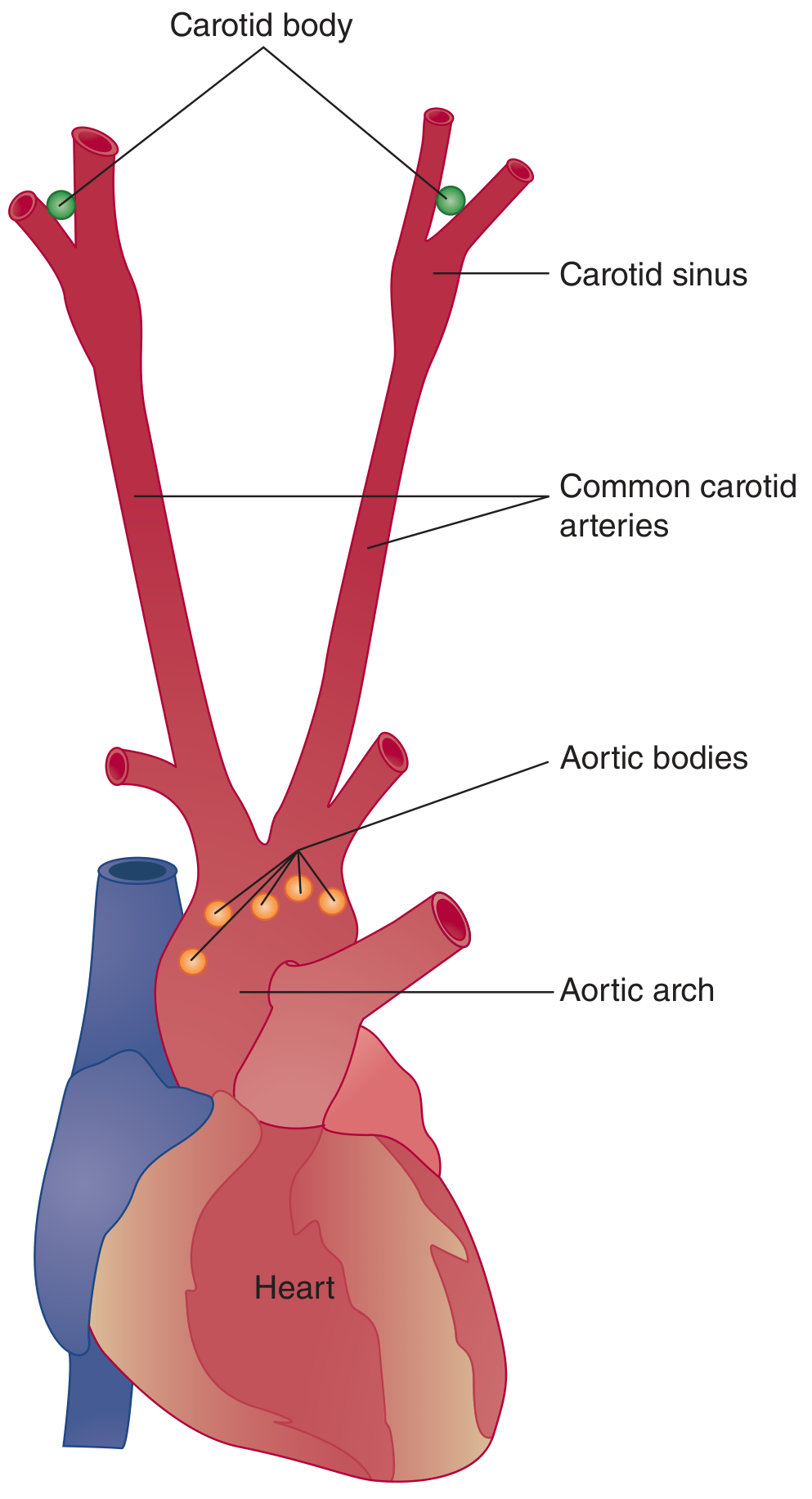
Carotid bodies (green dots) sit near the bifurcation. The carotid sinus is a dilation of the internal carotid just above the bifurcation. Aortic bodies cluster near the arch. (Ganong's Review of Medical Physiology, 26th Ed.)
At a Glance
| Feature | Carotid Sinus | Carotid Body |
|---|---|---|
| Type | Baroreceptor (mechanoreceptor) | Peripheral chemoreceptor |
| Senses | Arterial blood pressure (stretch/distension) | PaO₂, PaCO₂, pH |
| Location | Dilation of internal carotid artery just above bifurcation | Adventitia of posteromedial aspect of common carotid bifurcation |
| Structure | Stretch-sensitive nerve endings in vessel wall | Small neurovascular organ with Type I (glomus) and Type II cells |
| Afferent nerve | Carotid sinus nerve → CN IX (glossopharyngeal) | Nerve of Hering (branch of CN IX) → glossopharyngeal |
| CNS relay | Nucleus tractus solitarius (NTS), medulla | Chemosensitive area of medulla + respiratory centres |
| Primary response | Regulates heart rate, vascular tone, blood pressure | Increases ventilatory drive, also cardiovascular effects |
| Analogue structure | Aortic arch baroreceptors (CN X) | Aortic bodies (CN X via vagus) |
1. Carotid Sinus - Baroreceptor
Anatomy
"The carotid sinus is a small dilation of the internal carotid artery just above the bifurcation of the common carotid into external and internal carotid branches. Baroreceptors are in the adventitia of the vessel within this dilation."
- Ganong's Review of Medical Physiology, 26th Ed.
The receptor endings are mechanosensitive stretch receptors - they fire in proportion to the distension of the vessel wall, i.e., they directly sense arterial blood pressure.
Stimulus
- Activated by increased intraluminal pressure → vessel wall stretches → receptor fires more
- They are more sensitive to pulsatile pressure than constant pressure
- Most sensitive to rapid changes in pressure; rate of change is actually a stronger stimulus than absolute pressure
- Operational range: ~60-180 mmHg (fully activated at ~170 mmHg; silent below ~60 mmHg)
Afferent Pathway
- Carotid sinus nerve (nerve of Hering) → branch of CN IX (glossopharyngeal)
- Synapses on nucleus tractus solitarius (NTS) in medulla
- NTS then activates:
- Caudal ventrolateral medulla (CVLM) → GABAergic inhibition of rostral VLM (RVLM)
- Dorsal motor nucleus / nucleus ambiguus → vagal output
The Baroreceptor Reflex (Carotid Sinus Reflex)
When blood pressure rises (increased baroreceptor firing):
- Sympathetic outflow decreases → heart rate ↓, contractility ↓, vasodilation (↓TPR)
- Parasympathetic outflow increases → further heart rate ↓
- Net result: blood pressure falls back toward normal
When blood pressure falls (decreased firing):
- Sympathetic outflow increases → heart rate ↑, contractility ↑, vasoconstriction (↑TPR)
- Parasympathetic withdrawal
- Net result: blood pressure rises
This is a classic negative feedback loop for moment-to-moment blood pressure homeostasis. (Miller's Anesthesia, 10th Ed.; Costanzo Physiology, 7th Ed.)
Key Clinical Points
- In chronic hypertension, baroreceptors "reset" to the new higher pressure - they no longer signal it as abnormal, so hypertension is maintained rather than corrected
- Carotid sinus hypersensitivity - exaggerated baroreceptor response to neck pressure → severe bradycardia/syncope (e.g., when wearing a tight collar)
- Carotid sinus massage - used clinically to terminate supraventricular tachycardias by triggering vagal slowing of the AV node
- Volatile anaesthetics (especially halothane) inhibit the heart rate component of this reflex
2. Carotid Body - Peripheral Chemoreceptor
Anatomy
"The carotid body is located in the adventitia of the posteromedial aspect of the bifurcation of the common carotid artery. The normal carotid body measures 3 to 5 mm in diameter... average weight 12 mg."
- Cummings Otolaryngology
Despite its tiny size, blood flow and O₂ consumption per gram exceed those of the brain or thyroid - it is the most vascular tissue in the body relative to its mass, allowing it to sense arterial rather than venous blood chemistry.
Cell Types
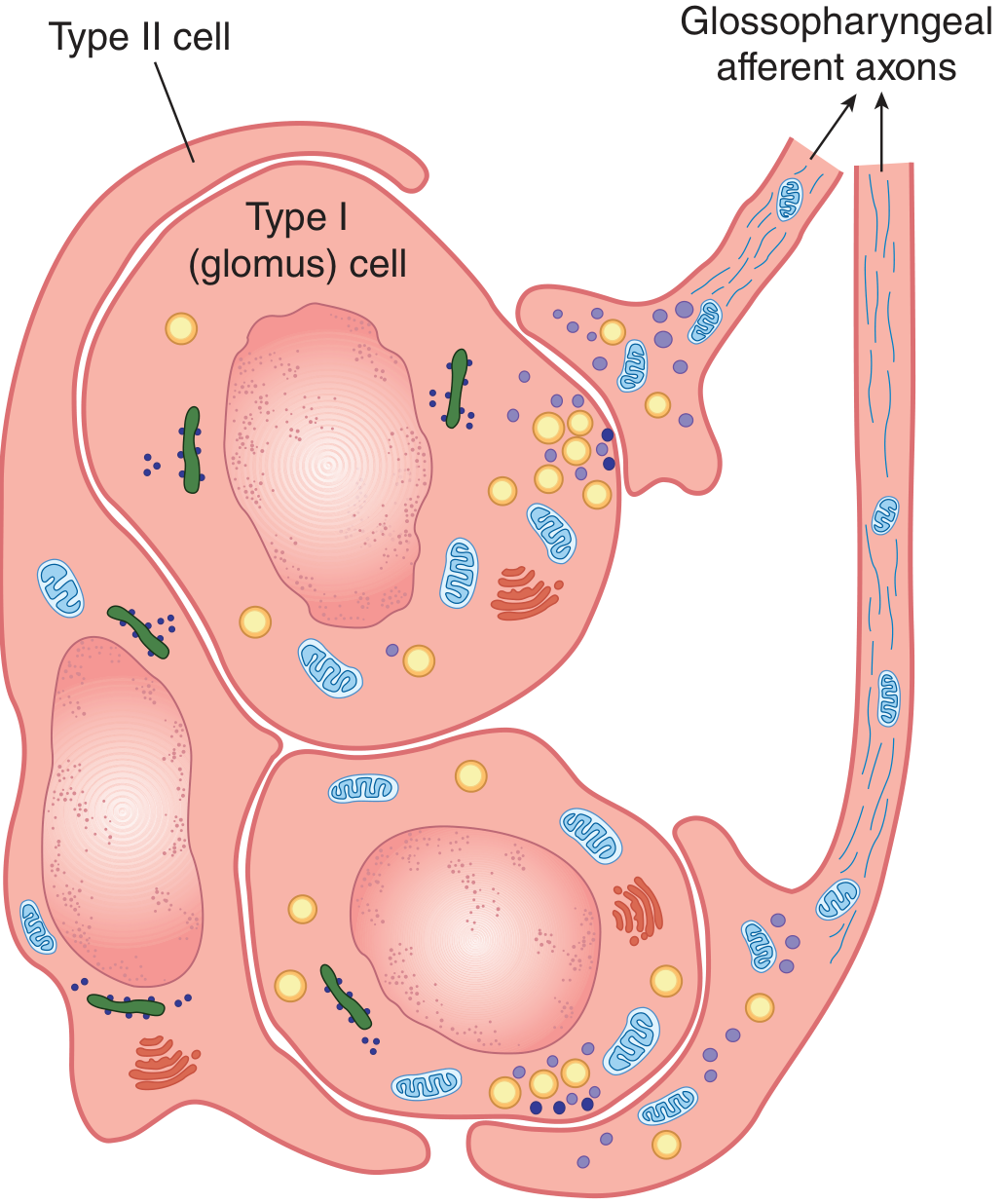
The carotid body contains two cell types surrounded by fenestrated sinusoidal capillaries:
| Cell | Also called | Origin | Function |
|---|---|---|---|
| Type I | Glomus cell | Neural crest | O₂ sensor; contains dense-core granules with catecholamines, dopamine, ACh, substance P; releases neurotransmitters on hypoxic stimulation |
| Type II | Sustentacular cell | Glial-like | Surrounds 4-6 Type I cells; support/scaffolding function; fully defined role unclear |
Stimuli
The carotid body is activated by:
- Hypoxia (PaO₂ < 60 mmHg) - the primary, most potent stimulus
- Hypercapnia (raised PaCO₂)
- Acidosis (low pH)
All three often occur together (e.g., hypoventilation). The body is an integrative sensor - acidosis and hypercapnia potentiate the response to hypoxia.
Mechanism of O₂ Sensing (Type I Glomus Cells)
Two complementary pathways are recognised:
Membrane hypothesis:
- Hypoxia inhibits O₂-sensitive K⁺ channels (outward rectifier, TASK channels) on Type I cells
- Reduced K⁺ efflux → membrane depolarisation → Ca²⁺ influx via L-type voltage-gated Ca²⁺ channels
- Ca²⁺ influx triggers action potentials and neurotransmitter release (dopamine, ACh, substance P, ATP)
- These neurotransmitters activate the cuplike endings of glossopharyngeal afferent fibers
Metabolic hypothesis:
- Mitochondrial cytochromes and NADPH oxidases act as O₂ sensors
- Hypoxia alters reactive oxygen species (ROS) generation → downstream signalling
Most likely both mechanisms work in concert across a range of hypoxemia severities. (Fishman's Pulmonary Diseases)
Afferent Pathway
- Nerve of Hering (a branch of CN IX, glossopharyngeal) → petrosal ganglion → medulla
- Drives the respiratory centre → increased rate and depth of breathing
- Also activates the parasympathetic system → bradycardia, ↓contractility (at normal O₂; masked by hypoxia's sympathetic drive)
Responses to Stimulation
| Stimulus | Primary Response | Cardiovascular Effect |
|---|---|---|
| Hypoxia (PaO₂ < 60 mmHg) | ↑ Ventilation rate and depth | Bradycardia (parasympathetic); with severe hypoxia: tachycardia (direct CNS sympathetic) |
| Hypercapnia | ↑ Ventilation | ↑ Sympathetic tone |
| Acidosis | ↑ Ventilation | ↑ Sympathetic tone |
"Acidemia, hypoxia, and hypercapnia stimulate the carotid body to initiate an autonomic reflex, which leads to increased respiratory rate and depth along with increased heart rate, blood pressure, and cerebral cortical activity."
- Cummings Otolaryngology
Key Clinical Points
- High altitude: People living at altitude have enlarged carotid bodies (up to 2× normal size) - chronic hypoxia causes hypertrophy
- Cyanotic congenital heart disease: Chronically blunted chemoreceptor sensitivity
- Carotid endarterectomy (CEA): Surgical manipulation can damage the nerve supply → postoperative respiratory insufficiency, reduced hypoxic ventilatory response
- Obstructive sleep apnea: Intermittent hypoxia sensed by carotid body mediates the hypertensive response
- Sudden infant death syndrome (SIDS): Some cases linked to small carotid bodies or decreased ratio of Type I to Type II cells - attenuated response to hypoxic crises
- Carotid body tumour (paraganglioma / glomus caroticum): Benign neuroendocrine tumour; associated with SDH gene mutations (SDHB, SDHC, SDHD)
3. Side-by-Side Comparison
| Carotid Sinus | Carotid Body | |
|---|---|---|
| Sensor type | Baroreceptor (pressure) | Chemoreceptor (chemistry) |
| What it detects | Arterial wall stretch = blood pressure | PaO₂, PaCO₂, arterial pH |
| Structure | Dilated thin-walled segment of internal carotid artery | Compact neurovascular organ (3-5 mm); Type I glomus cells + Type II sustentacular cells |
| Key nerve | CN IX (carotid sinus nerve) | CN IX (nerve of Hering) |
| CNS target | NTS → CVLM/RVLM + nucleus ambiguus | Medullary chemosensitive zone + respiratory centres |
| Primary function | Blood pressure homeostasis (moment-to-moment) | Respiratory drive; hypoxic ventilatory response |
| Triggered by | ↑ or ↓ arterial pressure | Hypoxia, hypercapnia, acidosis |
| Response to ↑ stimulus | ↓HR, ↓BP (vasodilation) | ↑Ventilation, cardiovascular effects |
| Aortic counterpart | Aortic arch baroreceptors (CN X) | Aortic bodies (CN X) |
| Clinical syndromes | Carotid sinus hypersensitivity, syncope | Carotid body tumour (paraganglioma), blunted hypoxic response |
| Effect of denervation | Acute hypertension (loss of inhibition) | Loss of hypoxic ventilatory drive |
Memory hook: The sinus is a sac (dilation) that detects stretch - S for Stretch/pressure. The body is a blob of cells that sniffs blood chemistry - B for Blood gases.
Sources:
- Ganong's Review of Medical Physiology, 26th Ed. - baroreceptor anatomy, carotid body cell types, afferent pathways
- Costanzo Physiology, 7th Ed. - baroreceptor reflex arc and medullary centres
- Miller's Anesthesia, 10th Ed. - baroreceptor reflex mechanism, chemoreceptor reflex
- Cummings Otolaryngology - carotid body anatomy, physiology, clinical associations
- Fishman's Pulmonary Diseases - O₂ sensing mechanisms (membrane vs. metabolic hypothesis)
This is a shared conversation. Sign in to Orris to start your own chat.