Mri findings in toxoplasmosis
Reading File
Finding Sources
Searching PubMed
toxoplasmosis MRI brain findings
Searching the Web
MRI findings cerebral toxoplasmosis eccentric target sign radiology
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from authoritative textbooks along with actual MRI images. Here is a complete, well-referenced answer:
MRI Findings in Cerebral Toxoplasmosis
Cerebral toxoplasmosis is caused by reactivation of Toxoplasma gondii in immunocompromised patients - primarily HIV/AIDS with CD4 counts below 100 cells/mm³. MRI is the most sensitive imaging modality and is more useful than contrast-enhanced CT for detection.
Location / Distribution
- Predilection sites: basal ganglia, thalamus, and corticomedullary junction
- Lesions are typically multiple (multifocal), though solitary lesions occur
- Can involve periventricular white matter and corpus callosum
Signal Characteristics by Sequence
| MRI Sequence | Typical Finding |
|---|---|
| T1 (unenhanced) | Hypointense lesions; peripheral T1 shortening if hemorrhage present |
| T2 / FLAIR | Hyperintense lesions with surrounding hyperintense perilesional edema; variable hypo-isointense or mixed patterns also described |
| T1 + Gadolinium | Ring-enhancing lesions (most common); can be nodular; may be absent in severely immunocompromised patients |
| DWI | Hyperintense on DWI; the core of the abscess typically does not show restricted diffusion (ADC values relatively low, but less restricted than pyogenic abscess) |
| ADC map | Relatively low ADC, but overlaps with lymphoma |
(Grainger & Allison's Diagnostic Radiology, p. 1482)
Pathognomonic / Characteristic Signs
1. Eccentric Target Sign (post-contrast T1)
The most specific imaging sign - seen in up to ~30% of cases. It consists of:
- An innermost enhancing eccentric nodule (viable trophozoites)
- A surrounding hypointense zone (coagulative necrosis)
- A peripheral enhancing rim (inflammatory vascular reaction)
This sign is highly suggestive of toxoplasmosis over other lesions, including CNS lymphoma.
2. Concentric Target Sign (T2-weighted)
Three concentric rings on T2:
- Central hyperintensity (necrotic fluid core)
- Peripheral hypointensity (mural blood / hemosiderin)
- Outer hyperintense ring of perilesional edema
(Mahadevan et al., J Magn Reson Imaging 2013)
MR Images from Textbooks
Fig. 1 - Cerebral toxoplasmosis in a 50-year-old HIV-positive male: (A) Axial FLAIR showing hyperintense lesions in the right frontal periventricular region and splenium of the corpus callosum. (B) High signal on DWI trace diffusion imaging.
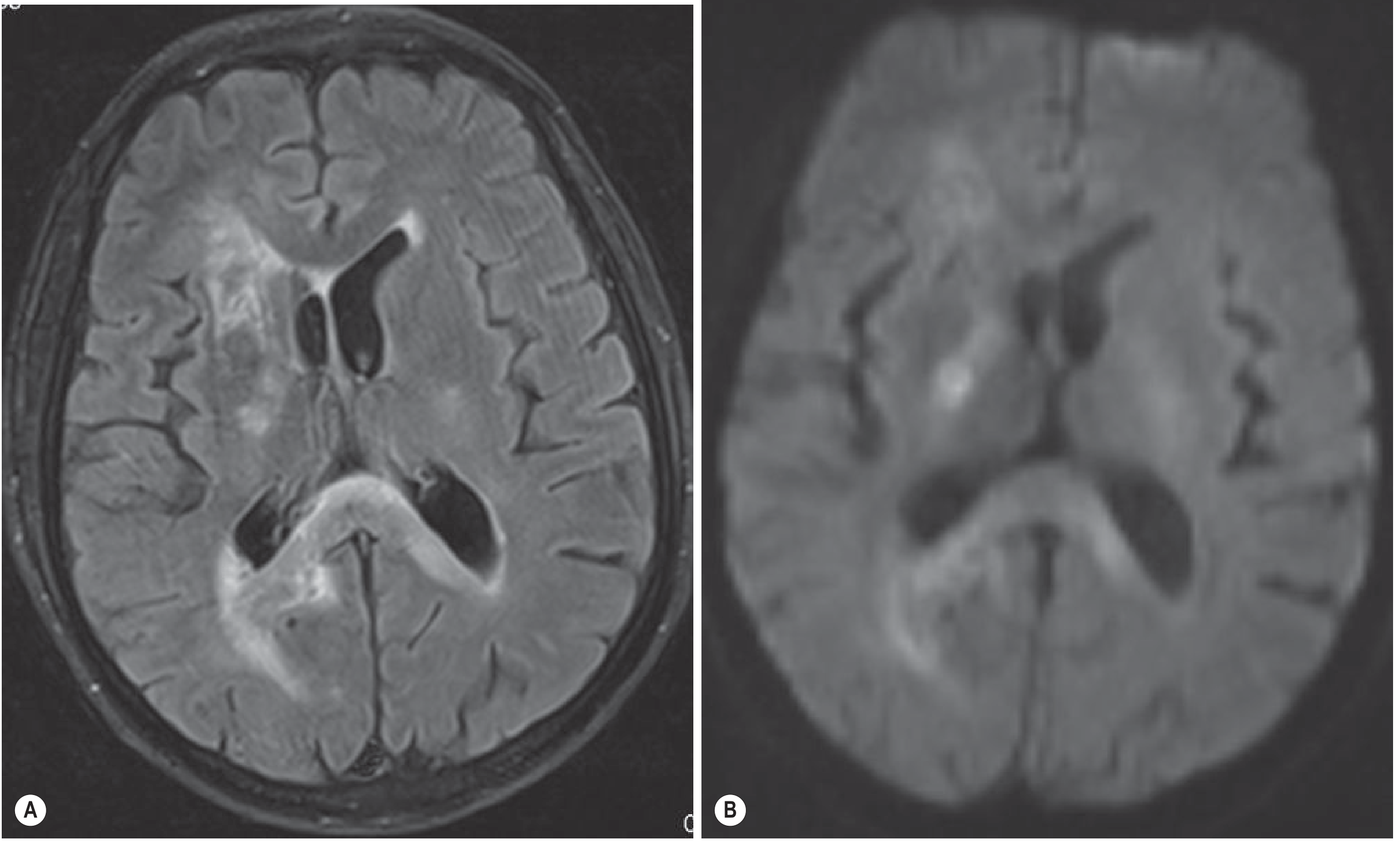
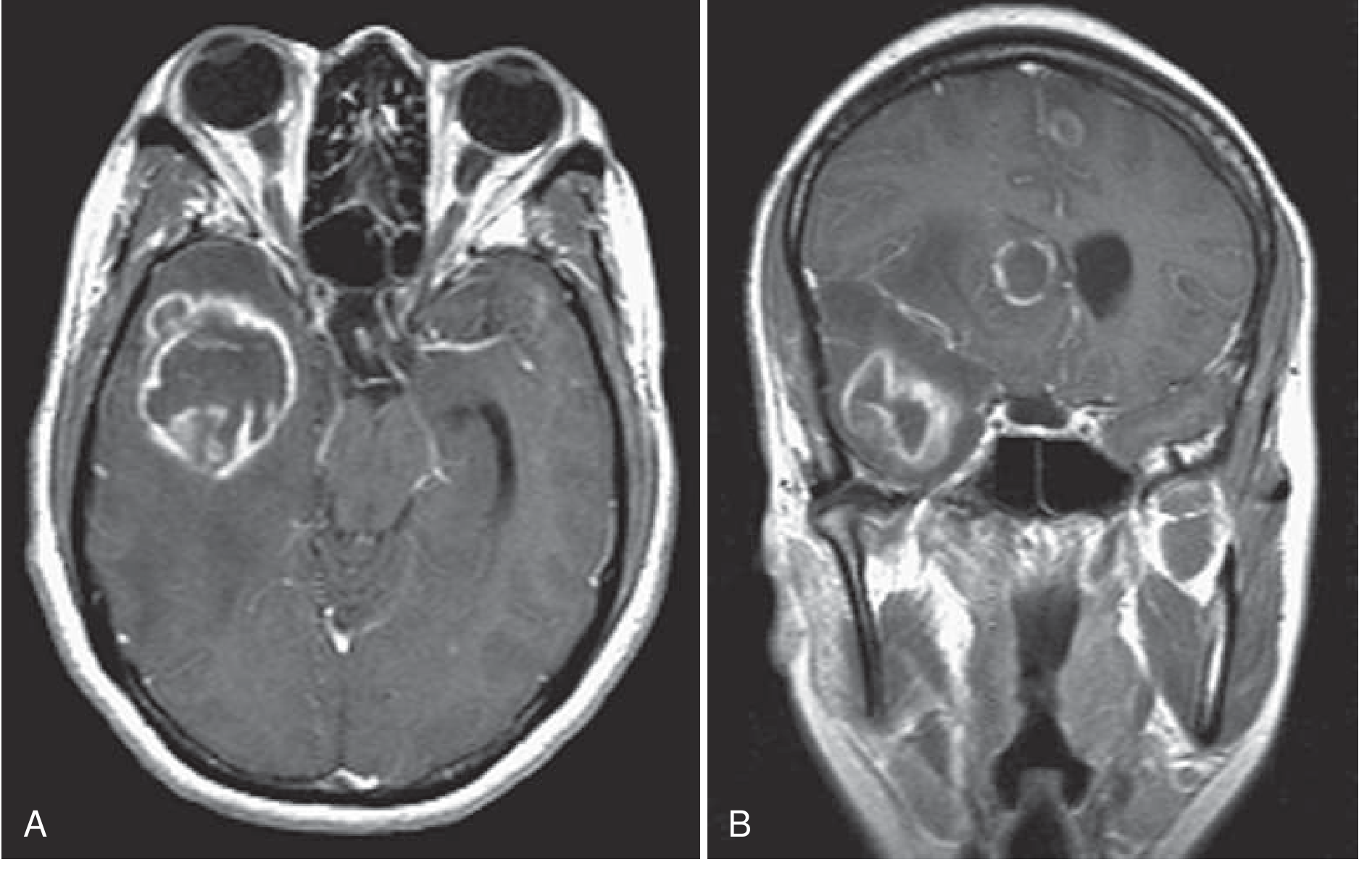
Fig. 2 - Cerebral toxoplasmosis in AIDS: Postgadolinium axial (A) and coronal (B) T1-weighted MRI showing multiple ring-enhancing lesions with mass effect.
Additional Advanced MRI Findings
MR Spectroscopy:
- Increased lipid-lactate peak (characteristic)
- Reduced Cho (choline), Cr (creatine), and NAA (N-acetylaspartate)
- Choline peak may occasionally also be elevated (overlaps with lymphoma)
MR Perfusion (DSC - Dynamic Susceptibility Contrast):
- Decreased perfusion with relative cerebral blood volume (rCBV) <1.5
- This contrasts with CNS lymphoma, which shows increased perfusion (rCBV >1.5)
- This distinction is the most useful advanced MRI feature to differentiate the two
(Radiopaedia - Neurotoxoplasmosis; AJR 2020)
Differential Diagnosis on MRI
| Feature | Toxoplasmosis | Primary CNS Lymphoma |
|---|---|---|
| Number | Multiple (usually) | Often solitary |
| Location | BG, corticomedullary junction | Periventricular, adjacent to lateral ventricles |
| DWI restriction | Variable (usually not restricted) | Restricted diffusion (hypercellular tumor) |
| Perfusion (rCBV) | Low (<1.5) | High (>1.5) |
| Thallium SPECT / FDG PET | Cold lesion (minimal uptake) | Hot lesion (high uptake) |
| Eccentric target sign | Present (~30%) | Absent |
| Response to empirical therapy | Lesions decrease in 10 days | No change |
(Grainger & Allison's Diagnostic Radiology, p. 1482; Tintinalli's Emergency Medicine, p. 1077)
Clinical Context
MRI is preferred over CT. In patients with HIV/AIDS, positive Toxoplasma IgG serology plus typical MRI findings justifies empirical treatment with pyrimethamine + sulfadiazine + leucovorin without waiting for biopsy. A decrease in lesion size within 10 days confirms the diagnosis. If no response, primary CNS lymphoma must be excluded by biopsy or Epstein-Barr virus PCR in CSF. - Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine
Mri findings of brain in cmv and ebv
Finding Sources
Finding Sources
Searching the Web
CMV encephalitis EBV CNS lymphoma MRI brain findings radiology
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10494941
Reading File
Finding Sources
I have comprehensive information from authoritative sources. Here is the full, well-structured answer:
MRI Findings of the Brain in CMV and EBV
Part 1: Cytomegalovirus (CMV) Encephalitis
CMV is a beta-herpesvirus. CNS infection almost exclusively occurs in severely immunocompromised patients - particularly HIV/AIDS with CD4 count <50 cells/µL. Two distinct CNS syndromes exist with different MRI patterns.
CMV Encephalitis (Hematogenous Spread)
Pathologically, CMV spreads hematogenously to cortical and subcortical gray matter, producing microglial nodules and cytomegalic cells.
| Sequence | Finding |
|---|---|
| T1 (unenhanced) | Decreased signal diffusely in parenchyma; ventriculomegaly |
| T2 / FLAIR | Increased signal intensity outlining the ventricles (periventricular); may be diffuse throughout the parenchyma |
| T1 + Gadolinium | Subependymal / periventricular enhancement - thin line of enhancement bordering the ventricles |
| CT equivalent | Ventriculomegaly; decreased attenuation diffusely |
Key feature: "Pencil-thin" T2/FLAIR periventricular hyperintensity with matching subependymal contrast enhancement - a pattern that distinguishes it from HIV encephalopathy (HAD) and PML. (Dartmouth CNS Infection Radiology; Harrison's Principles of Internal Medicine 22E)
CMV Ventriculoencephalitis (CSF Dissemination)
Occurs more acutely, often on a background of CMV retinitis. The MRI picture is more dramatic:
- Dilated ventricles (prominent ventriculomegaly) - a key distinguishing feature vs. CMV encephalitis
- Brainstem signal changes
- Ependymal enhancement lining the entire ventricular system
- Often associated with cerebellar T2/FLAIR abnormalities
(Bradley and Daroff's Neurology in Clinical Practice, p. 1639)
CMV - Summary of MRI Pattern
The hallmark is periventricular / subependymal disease, reflecting the virus's tropism for ependymal cells and periventricular tissue - the opposite of HIV encephalopathy which preferentially affects white matter.
- MRI is the method of choice (low sensitivity/specificity but best available imaging)
- May be normal in early disease
- Diagnosis confirmed by CSF CMV PCR (positive in <50% of encephalitis, better in ventriculoencephalitis)
Part 2: Epstein-Barr Virus (EBV) Brain Involvement
EBV causes CNS disease through three distinct mechanisms, each with a different MRI pattern:
2A. EBV Encephalitis (Immunocompetent, especially children)
EBV encephalitis is uncommon; MRI is abnormal in 27-80% of patients.
Distribution of involvement (from largest case series of 45 pediatric patients):
| Region | Frequency |
|---|---|
| Cortical / subcortical | 20% |
| White matter | 15.5% |
| Basal ganglia | 11% |
| Thalamus | 9% |
| Brainstem | 6.2% |
| Substantia nigra | 4.4% |
| Cerebellum | 4.4% |
| Spinal cord | 3% |
Signal characteristics:
- T2 / FLAIR: Hyperintense lesions in the above regions - often cortical/subcortical and basal ganglia
- DWI: Diffusion restriction seen in ~24% of cases
- SWI / GRE: Susceptibility changes (microhemorrhage) in ~15.5%
- Meningeal enhancement on post-contrast T1 in 5-22%
- Brainstem and cerebellar T2/FLAIR hyperintensity is notable in children
- Also in children/adolescents: prominent cerebellar involvement (Harrison's 22E)
(Vyas et al., as cited in PMC10494941)
2B. EBV-Associated Primary CNS Lymphoma (PCNSL) - Most Important CNS Manifestation
EBV is the causative driver of PCNSL in immunocompromised patients (HIV/AIDS, organ transplant recipients). In HIV-AIDS, virtually all PCNSL is EBV-driven.
In Immunocompetent Patients (EBV-negative or EBV-positive PCNSL):
The classic, "textbook" pattern:
| Feature | Finding |
|---|---|
| T1 | Hypointense to isointense |
| T2 | Iso- to hypointense (dense cellularity - unlike most tumors which are T2 bright) |
| T1 + Gadolinium | Vivid homogeneous enhancement (contact of intact blood-brain barrier in immunocompetent patients) |
| DWI | Restricted diffusion (hypercellular tumor - ADC low) |
| Location | Periventricular deep white matter, corpus callosum, basal ganglia; may show subependymal extension |
| Perfusion | Lower CBV than glioblastoma; lower peak height on perfusion curve |
In Immunocompromised Patients (HIV-associated EBV-driven PCNSL):
The pattern is different and more heterogeneous - mimics toxoplasmosis:
| Feature | Finding |
|---|---|
| Enhancement | Ring-enhancement (not homogeneous) - due to necrosis |
| T2 | Hyperintense necrotic core with peripheral iso/hypointense rim |
| SWI | Hypointense rim (hemorrhage/hemosiderin) |
| DWI | Peripheral restriction (ring pattern) |
| Necrosis & hemorrhage | More common than in immunocompetent PCNSL |
| Location | Deep, periventricular, often multiple |
| Size | Typically ≥4 cm (larger than toxoplasmosis lesions which are usually <4 cm) |
EBV-positive vs EBV-negative PCNSL (Lee et al.): Tumor necrosis, hemorrhage, and irregular/ring enhancement are significantly more common in EBV-positive PCNSL (P <0.001). (PMC10494941)
2C. EBV Smooth Muscle Tumors (EBV-SMT) - Rare
Seen in severely immunocompromised patients:
- CT: Iso- to hyperdense dural-based extra-axial lesions with substantial enhancement
- MRI T1: Hypo- to isointense
- T2: Prolongation (bright)
- Enhancement: Variable
- DWI: NO restriction (distinguishes from PCNSL)
- Resemble meningiomas or dural metastases
Comparison Table: CMV vs EBV Brain MRI
| Feature | CMV Encephalitis | EBV Encephalitis | EBV-PCNSL (Immunocompetent) | EBV-PCNSL (Immunocompromised) |
|---|---|---|---|---|
| Pattern | Periventricular | Cortical/BG/WM | Periventricular deep WM | Deep periventricular |
| T2/FLAIR | Periventricular rim | Focal hyperintensity | Iso/hypointense | Hyperintense (necrotic) |
| Enhancement | Subependymal (thin) | Meningeal ± parenchymal | Vivid homogeneous | Ring enhancement |
| DWI | Not prominently restricted | +/- restriction (24%) | Restricted | Peripheral restriction |
| Hemorrhage | Rare | SWI changes ~15% | Rare | Common |
| Mass effect | Minimal | Variable | Present | Present |
| Ventriculomegaly | Yes (especially ventriculoencephalitis) | No | No | No |
| Host | CD4 <50, HIV/AIDS | Children, immunocompetent | Immunocompetent adults | HIV/AIDS, transplant |
| Key biomarker | CSF CMV PCR | CSF EBV PCR / serology | CSF cytology / biopsy | CSF EBV PCR (nearly 100% sensitive in HIV-PCNSL) |
Sources: Bradley and Daroff's Neurology in Clinical Practice (p. 1639-1641); Harrison's Principles of Internal Medicine 22E (p. 1471); Kaplan & Sadock's Comprehensive Textbook of Psychiatry (p. 1868); Dartmouth CNS Infection Radiology Review; Unpacking CNS Manifestations of EBV - PMC
This is a shared conversation. Sign in to Orris to start your own chat.