MITRAL REGURGITATION
Reading File
Finding Sources
Searching PubMed
"mitral regurgitation"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Mitral Regurgitation (MR)
Definition
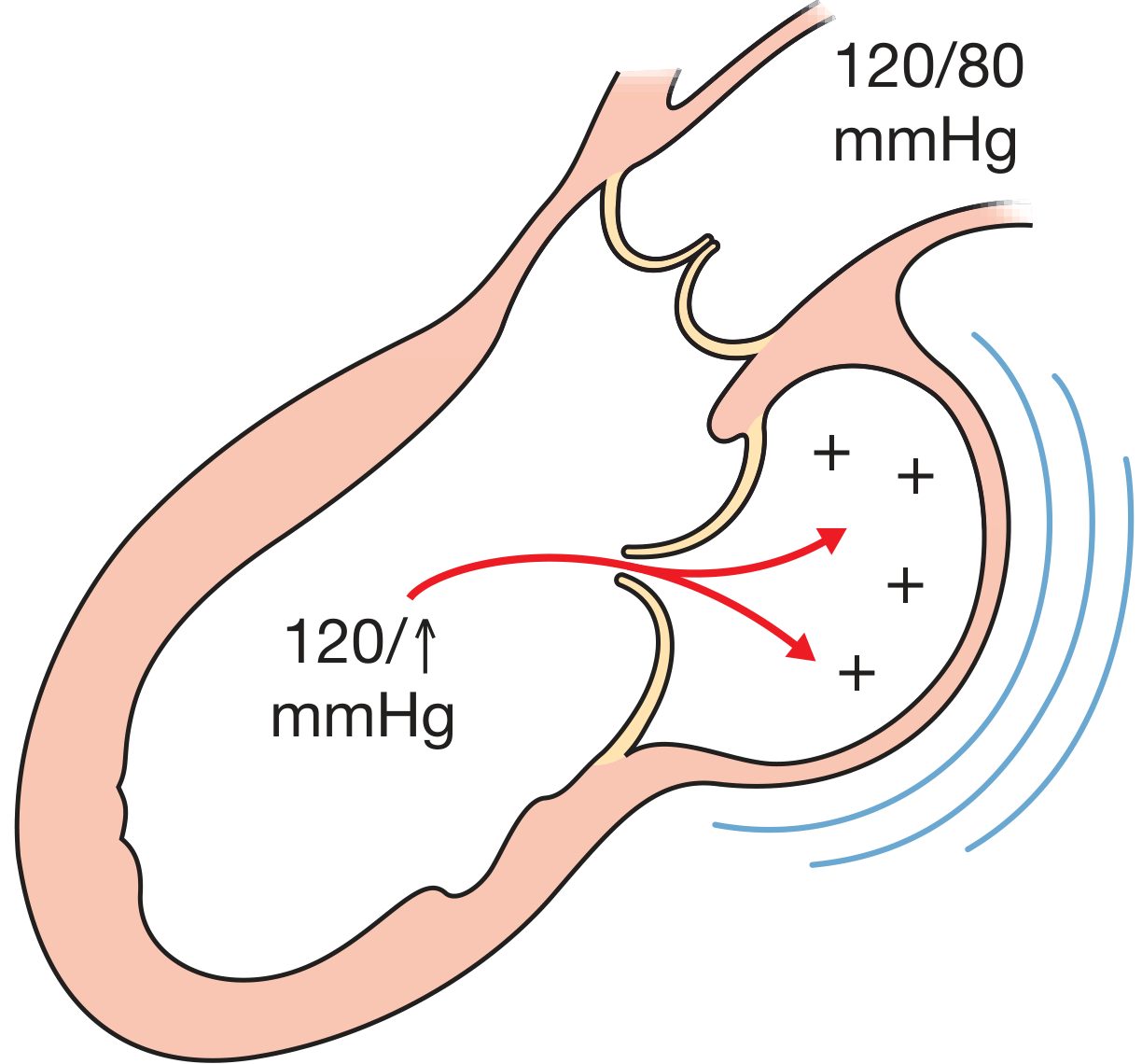
Mitral regurgitation is the abnormal retrograde (systolic) flow of blood from the left ventricle (LV) back into the left atrium (LA) due to failure of the mitral valve leaflets to coapt properly during systole. It is the most common form of valvular heart disease.
Classification
MR is classified into two major categories based on mechanism:
| Type | Mechanism | Examples |
|---|---|---|
| Primary (Organic/Degenerative) | Intrinsic leaflet disease | Mitral valve prolapse (MVP), fibromuscular dysplasia, rheumatic disease, infective endocarditis |
| Secondary (Functional/Ischemic) | Leaflets structurally normal; LV/LA disease displaces or distorts valve | Ischemic cardiomyopathy, dilated cardiomyopathy, atrial myopathy + AF |
- Braunwald's Heart Disease
Etiology
| Category | Causes |
|---|---|
| Degenerative | Barlow's disease (myxomatous degeneration), calcification of leaflets/annulus, Marfan/Ehlers-Danlos syndromes |
| Ventricular/Structural | MI with papillary muscle rupture, cardiomyopathy with annular dilation, transient ischemia |
| Autoimmune/Infective | Rheumatic fever, infective endocarditis |
| Other | Congenital mitral cleft, ergotamine-containing medications, radiotherapy, trauma |
- Bailey & Love's Short Practice of Surgery, 28th Ed.
Pathophysiology
The core mechanism is systolic retrograde ejection into the left atrium, creating a dual-outlet LV. The hemodynamic consequences differ sharply between acute and chronic forms:
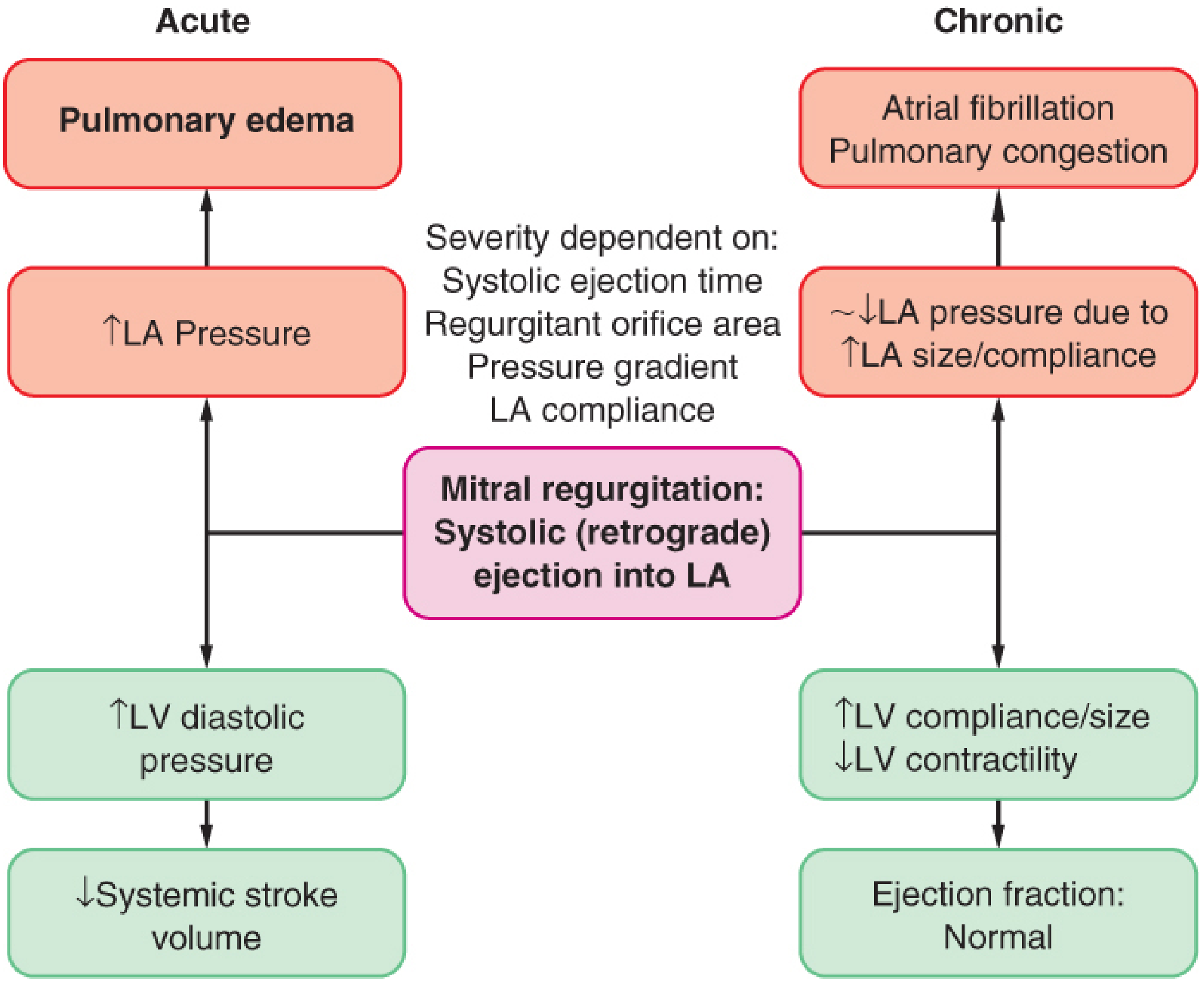
Acute MR
- The LV suddenly ejects blood back into a small, poorly compliant LA
- Abrupt rise in LA pressure → pulmonary venous hypertension → pulmonary oedema
- LV is effectively unloaded (reduced afterload), EF appears supranormal but forward stroke volume falls
- Causes: papillary muscle rupture post-MI, chordal rupture, acute endocarditis
Chronic Compensated MR
- Eccentric hypertrophy of LV develops (sarcomere replication in series)
- LA enlarges, increasing compliance → LA pressure normalized
- LV ejection fraction remains elevated due to reduced afterload and preserved contractile function
- Total stroke volume is increased; forward stroke volume approaches normal
- Patient may remain asymptomatic for years
Chronic Decompensated MR
-
Progressive contractile dysfunction develops → ESV rises, EF falls
-
Further LV dilation worsens regurgitation (annular dilatation, papillary muscle displacement → worse leaflet malcoaptation - a vicious cycle)
-
Despite significant contractile dysfunction, EF may still appear "normal" due to the favorable loading conditions - EF underestimates true myocardial dysfunction
-
Pulmonary congestion reappears; atrial fibrillation common with LA dilation
-
Severe MR causes decreased survival whether symptomatic or not
-
Goldman-Cecil Medicine, International Ed.
Severity of regurgitation depends on:
- Regurgitant orifice area
- LV-LA pressure gradient
- Systolic ejection time
- LA compliance
Clinical Features
Symptoms
- Acute MR: Acute onset pulmonary oedema, severe dyspnea, cardiogenic shock
- Mild chronic MR: Often asymptomatic
- Progressive chronic MR: Fatigue, exertional dyspnea, orthopnoea, palpitations (AF)
- Haemoptysis (with severe pulmonary hypertension)
Signs
- Apex: Displaced, heaving (volume-loaded LV); hyperdynamic apex beat
- Murmur: Pansystolic (holosystolic) murmur, best heard at apex, radiating to the axilla
- S3 gallop (volume overload)
- Signs of AF (irregularly irregular pulse) with LA dilatation
- Features of pulmonary hypertension in advanced disease (loud P2, RV heave)
Investigations
ECG
- P mitrale: bifid P waves (left atrial hypertrophy/dilatation)
- Left ventricular hypertrophy
- Atrial fibrillation (common with severe/longstanding disease)
Chest Radiograph
- Cardiomegaly (absent cardiomegaly suggests mild or acute MR)
- Prominent pulmonary vasculature
- LA enlargement (double shadow at right heart border; splaying of carina)
Echocardiography (Primary Investigation)
- TTE: Defines leaflet anatomy, LV size and function, LA size, estimates regurgitant severity
- Color-flow Doppler: Visualizes regurgitant jet; identifies jet direction, size, area
- Quantitative parameters:
- Vena contracta width (width of narrowest part of regurgitant jet)
- PISA (Proximal Isovelocity Surface Area): Calculates effective regurgitant orifice area (EROA) and regurgitant volume
- Pulmonary vein systolic flow reversal (indicates severe MR)
- TEE: Superior detail of leaflet anatomy; essential when TTE is non-diagnostic or surgery is planned; 3D TEE provides precise anatomy for surgical repair planning
- Severe MR criteria: EROA ≥ 0.40 cm² (primary), regurgitant volume ≥ 60 mL, regurgitant fraction ≥ 50%
Cardiac MRI
- Most accurate quantification of regurgitant volume and fraction
- Increasingly used when echo is insufficient
Cardiac Catheterization
-
For cases of diagnostic doubt regarding severity
-
Coronary angiography mandatory in patients >40 years or with suspected coronary disease prior to surgery
-
Textbook of Clinical Echocardiography; Goldman-Cecil Medicine; Bailey & Love
Management
Medical Therapy
Acute Severe MR:
- Goal: increase forward cardiac output, reduce regurgitant volume
- Arterial vasodilators (sodium nitroprusside): reduce SVR, preferentially increase aortic outflow, decrease regurgitant fraction - cannot use if hypotensive
- Intra-aortic balloon counterpulsation (IABP): used when vasodilators are contraindicated (hypotension) - increases forward output by reducing afterload and augmenting diastolic pressure
- Aim for urgent surgical correction
Chronic Asymptomatic MR:
- Afterload reduction is not definitively indicated in chronic asymptomatic MR with preserved LV function, since afterload is typically not increased
- "Watchful waiting / active surveillance" is appropriate until development of: symptoms, LV dysfunction, new AF, or pulmonary hypertension
- ACE inhibitors/ARBs: used if hypertension co-exists or in secondary MR with LV dysfunction
- Rate control for AF; anticoagulation if AF present
Chronic Symptomatic MR:
- Heart failure medical therapy (ACE inhibitors, beta-blockers, diuretics for symptom control)
- Does not delay surgery if criteria are met
Surgical Therapy
Indications for Surgery (Primary MR):
- Severe MR with symptoms (NYHA II-IV)
- Severe MR with LV dysfunction (EF ≤ 60% or LV end-systolic diameter ≥ 40 mm)
- New-onset atrial fibrillation attributable to MR
- Pulmonary hypertension (PA systolic pressure > 50 mmHg at rest or > 60 mmHg with exercise)
- Severe MR in patients undergoing cardiac surgery for another indication
- Asymptomatic severe MR with high likelihood of successful repair at an experienced center
Valve Repair vs. Replacement:
-
Valve repair is preferred when technically feasible:
- Lower operative mortality (~2% vs ~6% for replacement)
- Lower rate of endocarditis
- Better preserved LV function post-operatively
- Avoids lifelong anticoagulation (if bioprosthetic replacement used)
- Better long-term EF and survival
-
When repair is not feasible: valve replacement with preservation of subvalvular apparatus (chordal-sparing) is preferred
-
For severe ischemic MR: replacement shows less residual MR and less severe heart failure vs. repair at 1-2 years, though clinical outcomes are equivalent
-
Bailey & Love; Goldman-Cecil Medicine; Braunwald's Heart Disease; Symptom to Diagnosis 4th Ed.
Transcatheter / Percutaneous Therapy
For patients with prohibitive or high surgical risk:
-
MitraClip (TEER - Transcatheter Edge-to-Edge Repair): Replicates the Alfieri stitch - clips P2 and A2 segments of posterior and anterior leaflets together, creating a double-orifice mitral valve
- FDA approved for: primary (degenerative) MR with prohibitive surgical risk; secondary MR in heart failure patients with LV dysfunction despite optimal medical therapy (based on COAPT trial)
- EVEREST II: randomized comparison vs. surgery showed MitraClip is safer but less effective at reducing MR
- Performed via transseptal approach under TEE guidance
-
Other emerging devices: annuloplasty rings, leaflet augmentation, and transcatheter MVR devices (TMVR)
-
Braunwald's Heart Disease
Anesthetic Considerations (for MR Patients Undergoing Surgery)
| Parameter | Goal |
|---|---|
| Preload | Slightly increased (↑) |
| Afterload | Decreased (↓) - with vasodilators/anesthetics |
| Contractility | Maintain; titrate depressants carefully |
| Heart Rate | Slightly increased (↑); avoid bradycardia (worsens regurgitation) |
| Rhythm | Control ventricular rate if AF present |
| Post-CPB | Increase inotropy (afterload increases with competent valve after repair) |
- Barash Clinical Anesthesia, 9th Ed.
Natural History and Prognosis
-
Severe MR is associated with decreased survival whether symptomatic or not
-
Within 5 years of detecting severe MR: ~50% of patients develop LV dysfunction, AF, or heart failure requiring surgery
-
In asymptomatic patients with flail leaflets: mortality risk increases with increasing LV end-systolic diameter
-
Patients with secondary MR have worse prognosis, reflecting underlying LV dysfunction compounded by additional volume overload
-
Surgery (especially repair) improves both symptoms and survival when performed before irreversible LV dysfunction develops
-
Braunwald's Heart Disease; Goldman-Cecil Medicine
Sources: Braunwald's Heart Disease (11th Ed.) | Bailey & Love's Short Practice of Surgery (28th Ed.) | Goldman-Cecil Medicine (International Ed.) | Textbook of Clinical Echocardiography | Barash Clinical Anesthesia (9th Ed.) | Miller's Anesthesia (10th Ed.)
Surgical repair??
Finding Sources
Searching PubMed
"mitral valve repair"[MeSH Terms] AND techniques
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have everything needed for a comprehensive, well-illustrated answer on surgical repair of MR.
Surgical Repair of Mitral Regurgitation
Why Repair Over Replacement?
Mitral valve repair is the preferred operation whenever technically feasible for primary MR. Compared to replacement, repair offers:
-
Lower operative mortality (~1-3% vs ~6% for replacement)
-
Better preservation of LV function post-operatively (maintains the subvalvular apparatus)
-
Avoids prosthesis-related complications: no lifelong anticoagulation, lower risk of prosthetic valve endocarditis, no structural valve deterioration
-
Reoperation rates <10% at 10 years when postoperative echo shows mild or absent MR
-
Improved long-term event-free survival and quality of life
-
Sabiston Textbook of Surgery 11th Ed.; Bailey & Love 28th Ed.
Carpentier's Functional Classification (Foundation of Repair Planning)
The Carpentier classification is the essential framework guiding surgical repair - it categorizes MR by leaflet motion amplitude, not just anatomy:
| Type | Leaflet Motion | Lesions | Etiology |
|---|---|---|---|
| Type I | Normal | Annular dilatation; leaflet perforation/tear | Dilated cardiomyopathy, endocarditis, degenerative |
| Type II | Excessive (prolapse/flail) | Elongated/ruptured chordae; papillary muscle elongation/rupture | Fibroelastic deficiency, Barlow's, Marfan, endocarditis, trauma |
| Type IIIa | Restricted (systole AND diastole) | Leaflet thickening/retraction; chordal fusion; commissural fusion | Chronic rheumatic disease, carcinoid |
| Type IIIb | Restricted (systole only) | LV dilatation; papillary muscle displacement; chordal tethering | Ischemic/dilated cardiomyopathy (secondary MR) |
- Sabiston Textbook of Surgery - From Carpentier A, J Thorac Cardiovasc Surg 1983
Operative Setup and Exposure
- Cardiopulmonary bypass (CPB) with cardioplegic arrest
- Mitral valve exposed via:
- Opening the left atrium in the Waterston groove (most common), OR
- Transseptal approach - opening right atrium then interatrial septum
- Systematic valve assessment:
- Nerve hooks probe each segment of anterior and posterior leaflets
- Assess leaflet height, prolapse vs. tethering, leaflet structure
- Examine subvalvular apparatus: ruptured, elongated, or fused primary and secondary chords; papillary muscle status and position
- Water (saline) test: saline flushed into LV cavity identifies and marks prolapsing segments by showing where leaflets fail to coapt
- Fuster & Hurst's The Heart, 15th Ed.
Surgical Repair Techniques
The goal is to restore adequate leaflet coaptation surface - "repair should respect rather than resect tissues."
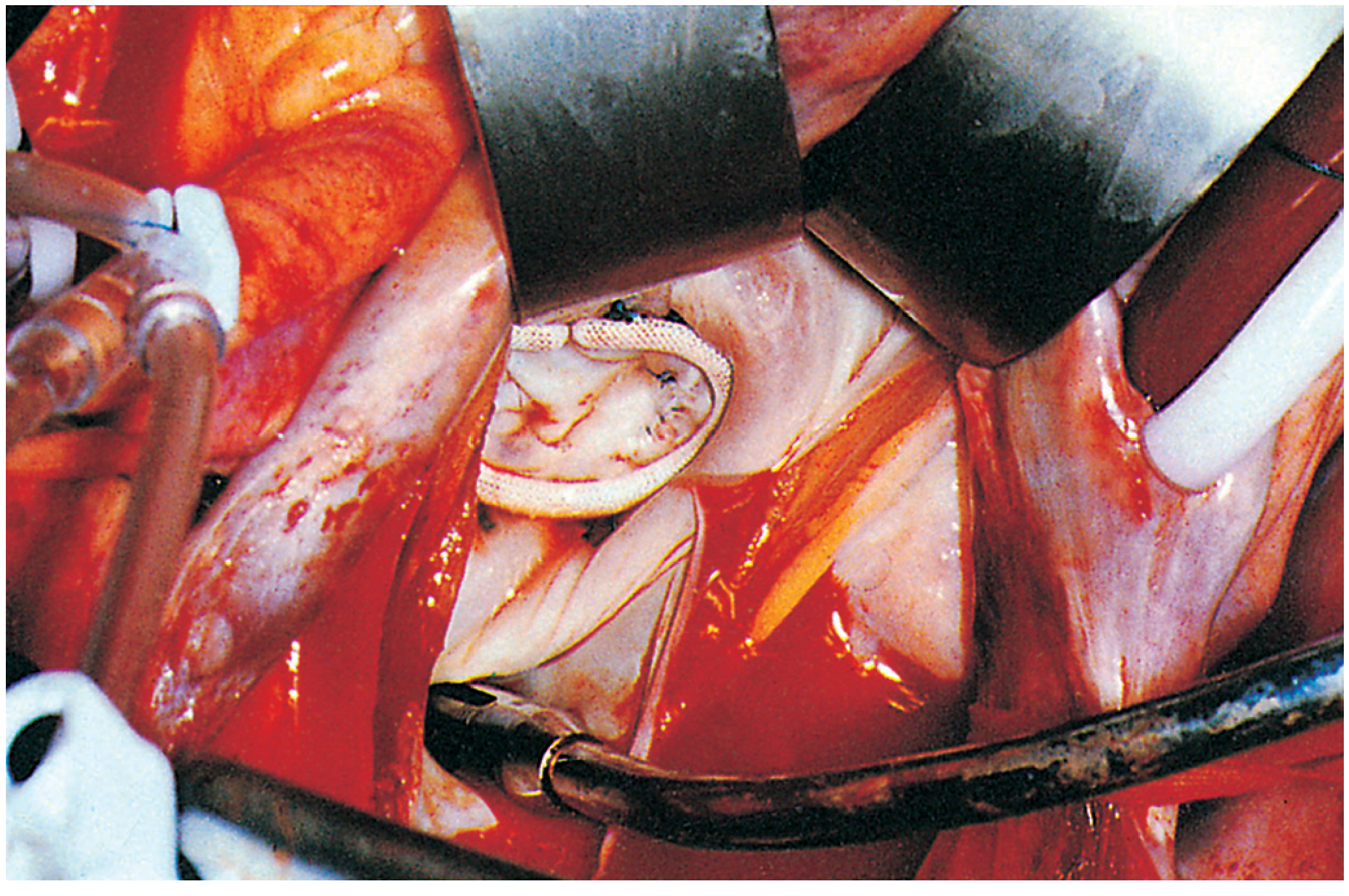
1. Ring Annuloplasty (Performed in EVERY Repair)
The cornerstone of all mitral valve repairs. A prosthetic ring is sutured to the mitral annulus to:
- Reduce annular diameter and restore normal annular geometry
- Restore the natural saddle-shape (3D) of the mitral annulus
- Enhance leaflet coaptation in all segments
- Stabilize and prevent future annular dilation (protects repair durability)
Ring types:
- Complete vs. partial (open) rings
- Flexible vs. semi-rigid vs. rigid
- Flat vs. 3D contoured (saddle-shaped)
- Sizing is based on measuring the height and surface area of the anterior leaflet
Ring annuloplasty alone may suffice for Type I MR (pure annular dilation with normal leaflets), but most repairs require additional leaflet techniques.
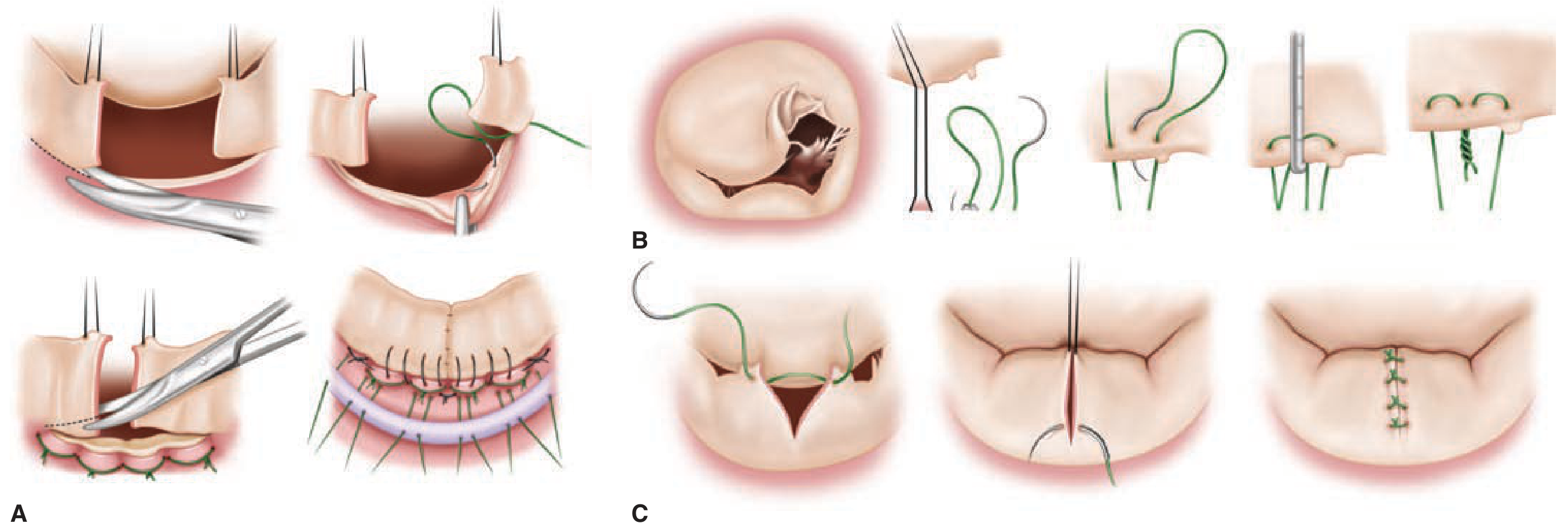
2. Posterior Leaflet Resection (for Type II - Posterior Leaflet Prolapse/Flail)
The most common repair technique. Used when a segment of the posterior leaflet prolapses/flails due to ruptured or elongated chordae.
Techniques:
A. Quadrangular Resection (Carpentier's "French Correction")
- A rectangular segment of the prolapsing posterior leaflet is excised
- The leaflet edges are sutured back together
- A sliding plasty may be added: relaxing incisions along the posterior leaflet base allow the leaflet to slide, reducing tension on the repair and decreasing posterior leaflet height
- Sliding plasty reduces the risk of SAM (see complications below)
B. Triangular Resection
- Smaller, more conservative resection of the prolapsing tip
- Increasingly preferred over quadrangular resection as it conserves more leaflet tissue
C. Sliding Leaflet Plasty (used with quadrangular resection)
- Reduces posterior leaflet height after resection
- Prevents post-repair SAM (systolic anterior motion)
3. Neochordae Implantation (PTFE Chordal Replacement)
Now the dominant technique for prolapse/flail, particularly for anterior leaflet and complex disease.
- Artificial chordae created from Gore-Tex (PTFE) sutures (CV-4 or CV-5)
- Sized to the appropriate height (measured from the annulus to the free leaflet edge at correct coaptation)
- One end attached to the papillary muscle head, the other to the free edge of the prolapsing leaflet
- Provides stable long-term leaflet support and prevents recurrent prolapse
- Advantages over resection: preserves leaflet tissue, lower risk of SAM, more versatile (can address multiple segments, anterior leaflet prolapse)
- Can be done with pre-looped PTFE "chordal loops" for standardization
4. Chordal Transfer (for Anterior Leaflet Prolapse)
- A secondary chord from the posterior leaflet (which has redundant chordae) is transferred to support the prolapsing free edge of the anterior leaflet
- Useful when neochordae are not preferred or in experienced centers as an alternative
5. Edge-to-Edge (Alfieri) Suture
- The free edges of the anterior and posterior leaflets at the site of prolapse/malcoaptation are sutured together, creating a double-orifice valve
- Replicates the surgical basis of the transcatheter MitraClip
- Used as a primary technique for commissural prolapse or as a "bail-out" if other techniques fail
- Must always be combined with annuloplasty ring
6. Leaflet Augmentation (Patch Repair)
- Leaflet defects (perforations from endocarditis, retracted rheumatic leaflets) are repaired using autologous pericardium or bovine pericardial patches
- Used in Type IV pathology (endocarditis, rheumatic disease, severe annular calcification)
- For rheumatic disease (Type IIIa): leaflet mobilization with pericardial augmentation to increase leaflet area and improve coaptation
7. Subvalvular Repair Techniques (for Secondary/Ischemic MR - Type IIIb)
- Papillary muscle approximation ("sling" procedure): sutures or bands drawn between the two papillary muscle heads to reapproximate them and reduce lateral tethering
- Papillary muscle repositioning: addresses the primary cause of tethering
- However, ring annuloplasty alone (undersized/downsized ring) has high recurrence rates (59% moderate-severe MR at 2 years) - this is why chordal-sparing replacement may be preferred for secondary MR (ACC/AHA 2020 guidelines: Class IIb)
Summary of Repair Techniques by Carpentier Type
| Carpentier Type | Repair Approach |
|---|---|
| Type I (normal motion) | Ring annuloplasty alone; patch for perforations |
| Type II (excessive motion) | PTFE neochordae; triangular/quadrangular resection + sliding plasty; chordal transfer; edge-to-edge; + ring |
| Type IIIa (restricted - rheumatic) | Leaflet mobilization; pericardial augmentation; subvalvular release; ring |
| Type IIIb (restricted - ischemic) | Undersized ring annuloplasty (high recurrence); subvalvular repair; or replacement preferred |
| Grade 4 (endocarditis, severe MAC) | Pericardial patch reconstruction; radical annular reconstruction; ring |
Pathoanatomic Grading System (Alreshidan/Herron)
A more detailed 4-grade system for repair planning:
| Grade | Pathology | Repair Options |
|---|---|---|
| 1 | Annular dilation; isolated posterior leaflet prolapse or single-segment flail | Focal resection/valvuloplasty; PTFE neochords; ring annuloplasty |
| 2 | Diffuse myxomatous disease, predominantly posterior leaflet (forme fruste Barlow's) | Partial resection + sliding plasty; multi-segment PTFE neochords; ring |
| 3 | Diffuse bi-leaflet myxomatous (Barlow's); anterior leaflet flail; multi-segment flail; focal posterior annular calcification | Partial resection + sliding plasty; multi-segment PTFE neochords; chordal transfer; focal calcium resection; ring |
| 4 | Endocarditis ± perforation/abscess; rheumatic Type IIIa; severe tethering Type IIIb; severe annular calcification | Pericardial patch augmentation; subvalvular mobilization; radical annular reconstruction; ring |
- Fuster & Hurst's The Heart 15th Ed. - From Alreshidan M et al., Semin CardioThorac Vasc Anesth 2019
Intraoperative Assessment of Repair Success
- Saline water test (after repair, before coming off CPB): saline injected into LV to check leaflet coaptation
- Intraoperative TEE (mandatory before weaning from bypass):
- Must demonstrate mild or no residual MR for repair to be deemed successful
- Adequate leaflet coaptation height and surface
- No systolic anterior motion (SAM) of the anterior leaflet
- No significant mitral stenosis (adequate valve opening area)
- If residual moderate or severe MR: repair must be revised or conversion to replacement
- Fuster & Hurst's The Heart 15th Ed.
Key Complication: Systolic Anterior Motion (SAM)
SAM is a post-repair complication where the anterior mitral leaflet is displaced into the LV outflow tract (LVOT) during systole, causing dynamic LVOT obstruction.
Mechanism: Occurs when excess leaflet tissue (especially with oversized posterior leaflet after resection) is pushed into the outflow tract by a Venturi effect.
Management:
-
Increase preload and afterload (fluid loading)
-
Negative inotropy (reduce/stop inotropes)
-
Beta-blockers (negative chronotropy)
-
If irreversible: return to bypass for corrective surgery - larger annuloplasty ring and/or reduction of posterior leaflet height (Alfieri stitch or re-resection)
-
Fuster & Hurst's The Heart 15th Ed.
Outcomes
| Metric | Data |
|---|---|
| Operative mortality | 1-3% |
| Freedom from reoperation at 10 years | >94% (experienced centers) |
| Freedom from MR >2/4 at 1 month | 98.7% |
| Freedom from MR >2/4 at 5 years | ~82% |
| Freedom from MR >2/4 at 10 years | ~65% |
| MR recurrence at 5 years | Up to 30% overall; higher with Barlow's (6%/year) vs. fibroelastic deficiency (2.6%/year) |
Recurrence is related to: which leaflet is repaired, amount of foreign material (patch) used, severity of underlying pathoanatomy, and center experience.
Contemporary mitral valve repair in experienced surgeons' hands remains the gold standard treatment for primary MR. - Fuster & Hurst's The Heart 15th Ed.
When Replacement is Preferred Over Repair
- Severe annular calcification (MAC) precluding ring placement
- Extensive rheumatic disease with subvalvular fusion not amenable to repair
- Severe secondary (ischemic) MR - chordal-sparing replacement has superior MR reduction vs. ring annuloplasty alone (ACC/AHA Class IIb)
- Failed prior repair
- Complex anatomy at non-expert center (repair durability requires surgical experience)
Sources: Sabiston Textbook of Surgery 11th Ed. | Fuster & Hurst's The Heart 15th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed. | Miller's Anesthesia 10th Ed. | Braunwald's Heart Disease 11th Ed. | Barash Clinical Anesthesia 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.