pcos
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of PCOS:
Polycystic Ovary Syndrome (PCOS)
Definition & Epidemiology
PCOS is the most common endocrine disorder in women of reproductive age, affecting 5–10% of women worldwide. It is also the most common cause of hyperandrogenism (HA), hirsutism, and anovulatory infertility in developed countries. First described by Stein and Leventhal in 1935 (bilateral polycystic ovaries + obesity + amenorrhea), it is now understood as a heterogeneous syndrome with reproductive, metabolic, and cardiovascular consequences. Its genetic basis is likely polygenic and multifactorial.
Pathophysiology
Three interrelated disturbances drive the syndrome:
1. Hypothalamic-Pituitary Dysregulation
- Increased LH pulse frequency and amplitude, leading to a raised LH:FSH ratio (in ~⅔ of patients)
- Excess LH stimulates ovarian theca cells → excess androgen production
- Insufficient FSH → arrested follicular development → anovulation
2. Hyperandrogenism
- Elevated androgens (testosterone, androstenedione, DHEAS) arise from both the ovaries and adrenal glands
- Androgens are converted peripherally (especially in adipose tissue) to estrogens, which exerts positive feedback on LH — creating a self-perpetuating cycle
- Skin 5α-reductase converts testosterone → DHT, causing hirsutism and acne (activity varies by ethnicity, explaining why hirsutism appears in ~70% of US patients vs. only 10–20% in Japan)
3. Insulin Resistance & Hyperinsulinemia
- Present in the majority, independent of obesity
- Hyperinsulinemia directly stimulates ovarian androgen production and suppresses sex hormone-binding globulin (SHBG), increasing free androgen levels
- PCOS typically arises at puberty; obesity worsens the phenotype by amplifying hyperinsulinemia
Clinical Features
| Domain | Features |
|---|---|
| Menstrual | Oligomenorrhea, amenorrhea (rarely primary); irregular cycles from menarche |
| Androgen excess | Hirsutism (~70%), acne, male-pattern alopecia |
| Metabolic | Obesity (>50%, android/central distribution), insulin resistance, dyslipidemia |
| Ovarian | Polycystic ovary morphology on ultrasound |
| Reproductive | Anovulatory infertility, increased miscarriage risk |
| Psychological | Depression, anxiety (screen at diagnosis) |
Diagnosis
PCOS is a diagnosis of exclusion. The 2003 Rotterdam Criteria (most widely used) require 2 of 3:
- Oligo-ovulation or anovulation
- Clinical and/or biochemical hyperandrogenism (hirsutism, acne, alopecia; or elevated free testosterone)
- Polycystic ovarian morphology on ultrasound — ≥20 follicles (2–9 mm) in either ovary and/or ovarian volume >10 mL
In adolescents, diagnosis requires both persistent anovulation and clinical/biochemical HA (PCO morphology alone is insufficient).
Differential Diagnoses to Exclude:
- Non-classic congenital adrenal hyperplasia → 17-OHP (follicular phase) to screen
- Cushing syndrome → 24-hr urinary cortisol / overnight dexamethasone suppression
- Hyperprolactinemia → serum prolactin
- Androgen-secreting neoplasm → imaging if testosterone very high
- Thyroid disease → TSH
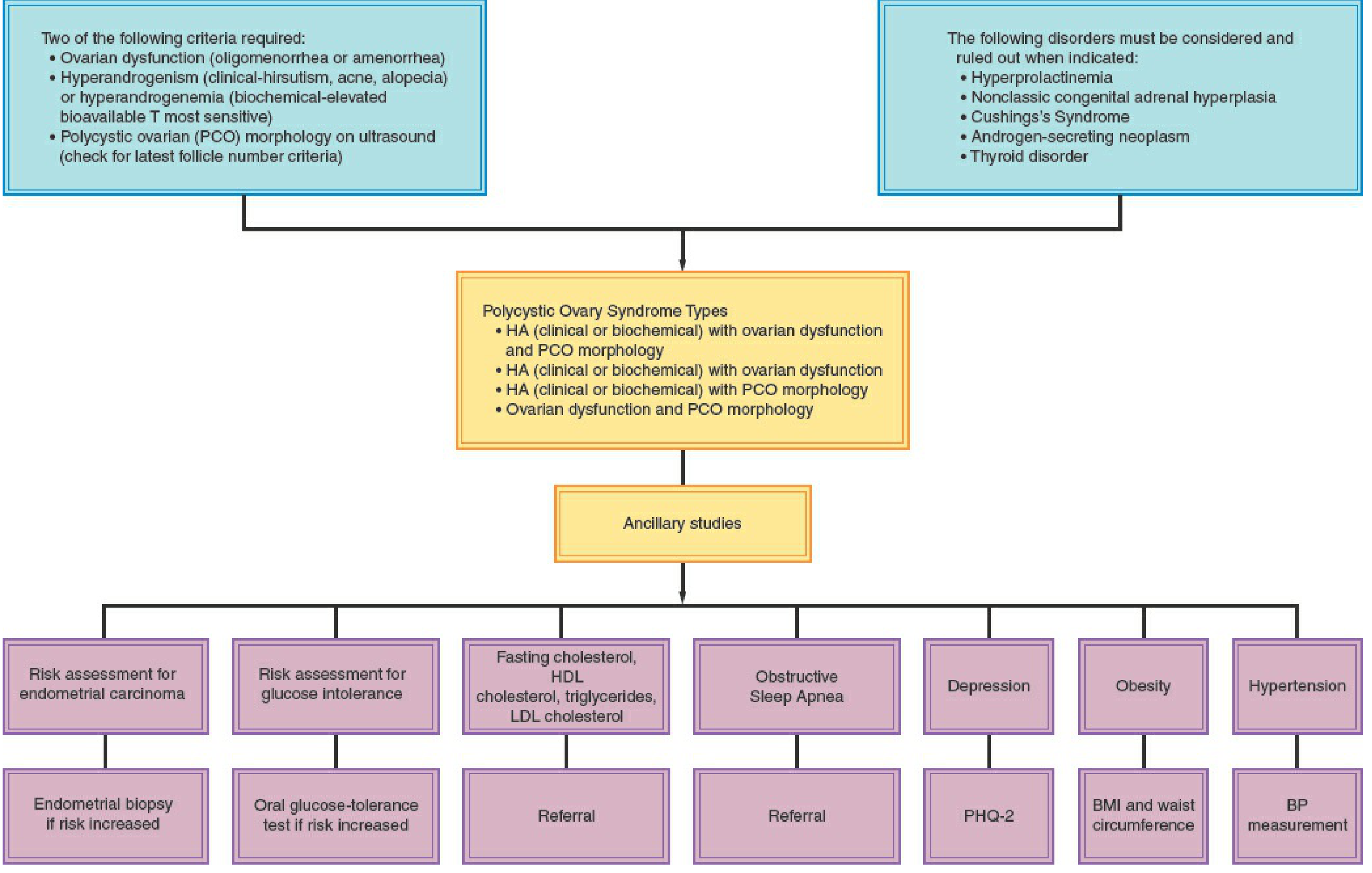
Ancillary Workup at Diagnosis:
- Fasting glucose / oral GTT (screen for impaired glucose tolerance/T2DM)
- Fasting lipid profile (overweight/obese women)
- BMI, waist circumference, blood pressure
- PHQ-2 (depression screen)
- Consider endometrial biopsy if prolonged anovulation (endometrial hyperplasia risk)
Management
Treatment is tailored to the patient's primary concern (menstrual irregularity, hyperandrogenism, infertility, or metabolic risk).
All Patients — Universal
- Lifestyle modification (diet + exercise): first-line for all women; even modest weight loss (5–10%) improves menstrual regularity, hyperandrogenism, and insulin sensitivity
- Screen and monitor: obesity, hypertension, glycemic control, depression, anxiety — at diagnosis and at regular intervals
Women Not Seeking Pregnancy
| Goal | Therapy |
|---|---|
| Menstrual regulation + androgen control | Combined oral contraceptive pill (COCP) — first-line; increases SHBG, suppresses LH/androgens |
| Inadequate response to COCP after 6 months | Add antiandrogens: spironolactone, flutamide |
| Endometrial protection (if OCP not used) | Cyclic progestin (MPA 10 mg or progesterone 200 mg × 10–14 days every ≥3 months) or levonorgestrel IUD |
| Cardiometabolic risk reduction | Metformin — especially for overweight/obese women |
Women Seeking Pregnancy (Ovulation Induction)
- Letrozole (aromatase inhibitor) — first-line for ovulation induction in PCOS
- Clomiphene citrate ± metformin — second-line
- Injectable gonadotropins — used judiciously (risk of ovarian hyperstimulation syndrome is higher in PCOS)
- Metformin — adjunct with diet/exercise in obese women; alone is not recommended for infertility treatment
Metformin is not recommended as monotherapy for endometrial protection, treatment of hyperandrogenic symptoms, prevention of pregnancy loss, or prevention of gestational diabetes.
Complications & Long-term Risks
Reproductive
- Anovulatory infertility — most common endocrine cause
- Increased risk of early miscarriage, gestational diabetes, gestational hypertension, preeclampsia, preterm birth
- Prepregnancy counseling and lifestyle management recommended before conception
Metabolic / Cardiovascular
- Type 2 diabetes and impaired glucose tolerance — screen with oral GTT
- Dyslipidemia (elevated LDL, triglycerides; low HDL) → increased long-term cardiovascular disease risk
- Obstructive sleep apnea — increased prevalence, refer if suspected
- Non-alcoholic fatty liver disease
Oncological
- Endometrial carcinoma — chronic anovulation leads to unopposed estrogen stimulation; endometrial biopsy if at increased risk
Psychiatric
- Higher rates of depression and anxiety — screen at diagnosis and regularly
Recent Evidence (2024–2025)
- Inositol (myo-inositol + D-chiro-inositol) was evaluated in a 2024 meta-analysis for the 2023 updated PCOS guidelines — modest evidence for improving metabolic and reproductive outcomes (PMID: 38163998)
- Lifestyle interventions remain foundational: a 2025 systematic review confirmed significant improvements in insulin resistance, androgen levels, and menstrual regularity with structured exercise and diet (PMID: 39861440)
- Pregnancy outcomes: A 2024 meta-analysis in Nature Communications quantified increased risks of gestational diabetes, preeclampsia, and preterm birth, reinforcing preconception counseling (PMID: 38965226)
Sources: Berek & Novak's Gynecology; Harrison's Principles of Internal Medicine, 22e; Goldman-Cecil Medicine
inguinal hernia
Reading File
Finding Sources
Searching PubMed
"inguinal hernia"[MeSH Terms] AND repair
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Inguinal Hernia
Definition & Epidemiology
An inguinal hernia is the protrusion of abdominal contents through a defect in the inguinal region. 75% of all hernias occur in the inguinal region, making it the most common hernia type. About two thirds are indirect and one third are direct. There is a strong male predominance (~10:1 over females for inguinal hernias), and they are more common on the right side.
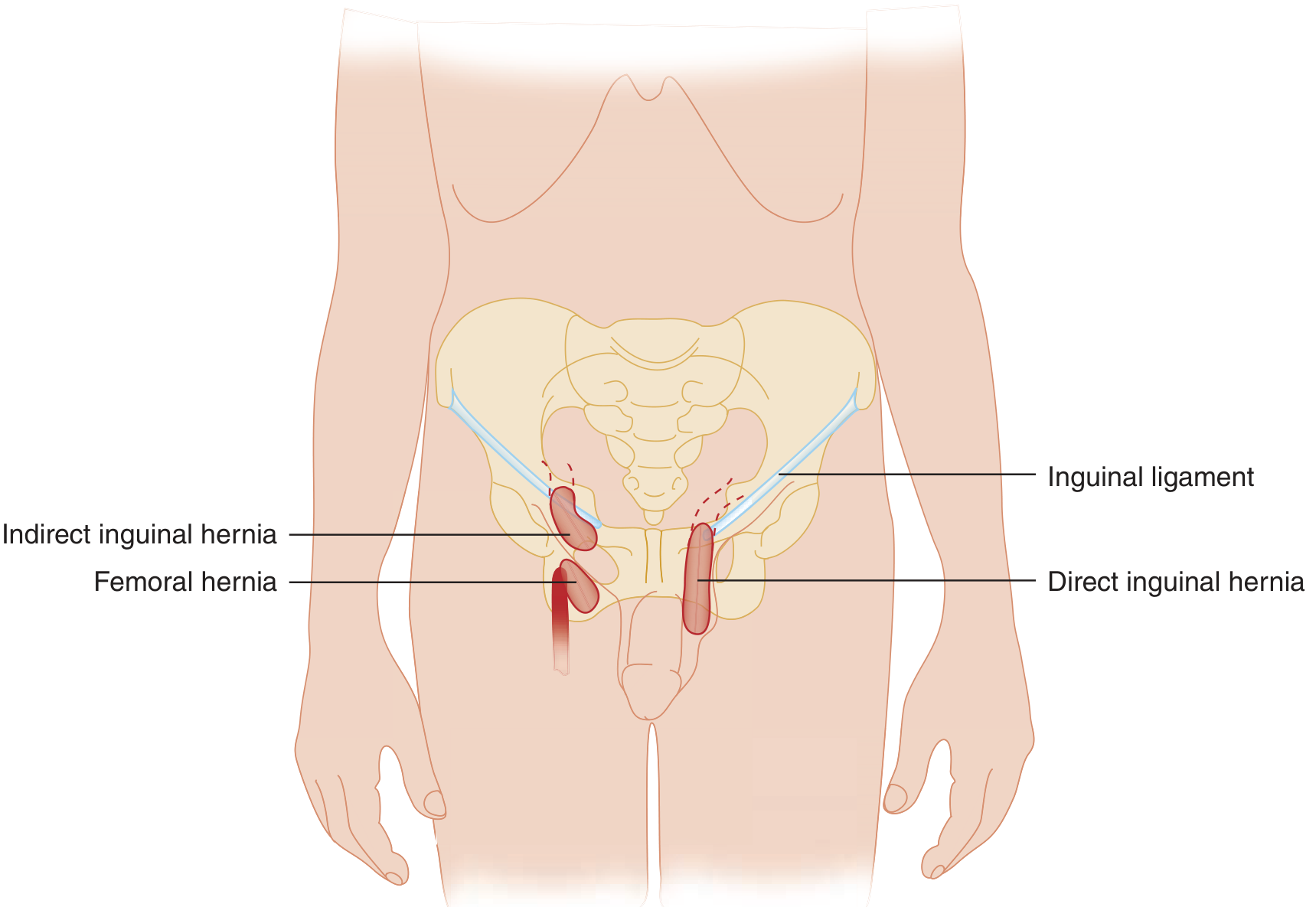
Relevant Anatomy
The inguinal canal is a 4 cm oblique passage through the lower abdominal wall, running from the deep (internal) inguinal ring to the superficial (external) inguinal ring. Key boundaries:
- Floor: inguinal ligament
- Roof: internal oblique and transversus abdominis muscles
- Anterior wall: external oblique aponeurosis
- Posterior wall: transversalis fascia
The Hesselbach triangle is bounded by:
- Medially: rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
Content of the canal: spermatic cord (male) or round ligament (female).
Classification
| Type | Mechanism | Key Feature |
|---|---|---|
| Indirect inguinal | Passes through deep inguinal ring → along canal → exits superficial ring → may enter scrotum | Lateral to inferior epigastric vessels; within spermatic cord; most common type (~67%) |
| Direct inguinal | Protrudes directly through posterior wall of canal (Hesselbach's triangle) | Medial to inferior epigastric vessels; rarely enters scrotum; caused by posterior wall weakness |
| Femoral | Passes through femoral canal, below inguinal ligament | More common in women; high incarceration/strangulation risk |
Memory aid — "MDs don't LIe": Medial = Direct; Lateral = Indirect
Special Hernia Variants
- Richter hernia: only the antimesenteric border of intestine herniates (partial wall circumference) → may strangulate without overt bowel obstruction; no vomiting
- Reduction en masse: hernia reduced manually but bowel remains strangulated inside the peritoneal cavity within the sac — a dangerous, rare complication of ED reduction
Pathogenesis
Indirect (Congenital/Pediatric)
- Failure of closure of the processus vaginalis — a peritoneal diverticulum that follows the testis as it descends into the scrotum
- All pediatric inguinal hernias are by definition indirect
- Partial closure → hydrocele; complete patency → hernia
- High incidence in premature infants (closure normally occurs before birth)
Direct (Acquired/Adult)
- Acquired weakness of the transversalis fascia (posterior inguinal wall)
- Associated with increased intra-abdominal pressure (chronic cough, constipation, heavy lifting), connective tissue disorders, and aging
Clinical Presentation
- Groin bulge — most common; appears on standing/Valsalva, reduces with recumbency
- Aching or dragging sensation in the groin, worsened by exertion
- Scrotal swelling — in large indirect hernias extending into the scrotum
- On exam: thickened spermatic cord on the affected side; impulse felt on cough at the external ring
Complications
| Complication | Description | Management |
|---|---|---|
| Reducible | Contents return spontaneously or with manual pressure | Elective repair |
| Incarcerated | Contents irreducible; no vascular compromise yet; firm non-tender or mildly tender bulge | Attempt manual reduction in ED; urgent surgical repair |
| Strangulated | Vascular compromise → ischemia → necrosis; tender, erythematous, hard bulge; bowel obstruction, systemic toxicity | Emergency surgery |
Diagnosis
Primarily clinical. Investigations are adjuncts:
- Ultrasound: operator-dependent; identifies hernia sac, contents, reducibility; free fluid in sac = sensitive for incarceration/strangulation; best for children and pregnant women (no radiation)
- Doppler US: insensitive for venous/lymphatic compromise; can detect arterial flow
- CT scan: best overall imaging modality — identifies uncommon types (Spigelian, obturator), confirms incarceration/strangulation, demonstrates bowel obstruction
- Plain films: non-diagnostic for hernia; may show bowel obstruction
- Herniography (peritoneography): fluoroscopic contrast exam — reserved for occult hernias when other imaging is inconclusive; sensitive with high negative predictive value
Key differentials for scrotal/groin swelling: hydrocele, lymphadenopathy, femoral hernia, lipoma of cord, varicocele, undescended testis
| Feature | Hydrocele | Indirect Inguinal Hernia |
|---|---|---|
| Transillumination | Positive | Negative |
| "Get above it" | Yes | No |
| Reducibility | Non-reducible | Often reducible |
| Cough impulse | Absent | Present |
Management
Adults — Elective Repair Indications
- Symptomatic hernia → elective repair
- Femoral hernia → repair recommended regardless of symptoms due to very high strangulation risk (22% at 3 months, 45% at 21 months)
- Asymptomatic inguinal hernia in elderly/high-risk patients → watchful waiting may be considered
Surgical Repair Options
Open Approach
- Lichtenstein tension-free mesh repair — gold standard for open repair; prosthetic mesh placed over the inguinal floor; low recurrence (~1%)
- Herniorrhaphy (children) — high ligation of hernia sac only; no floor reconstruction needed
- Mesh plug repair — alternative open method; higher recurrence for inguinal, acceptable for femoral
Laparoscopic Approach
- TEP (Total ExtraPeritoneal) — mesh placed extraperitoneally; avoids peritoneal entry
- TAPP (TransAbdominal PrePeritoneal) — transabdominal, mesh placed preperitoneally
- European Hernia Society recommends Lichtenstein or TEP as the standard approaches; comparable outcomes but laparoscopic has less postoperative pain and earlier return to work
- Preferred when: bilateral hernias, recurrent hernias, unclear femoral vs. inguinal type, or prior lower abdominal surgery makes anatomy clearer laparoscopically
Anesthesia
- All repairs can be performed under local, spinal, epidural, or general anesthesia
- Laparoscopic repairs require general anesthesia
- In premature infants: spinal anesthesia preferred to reduce postoperative apnea risk vs. general anesthesia
ED Management of Incarcerated Hernia
- NPO status
- Adequate IV narcotic analgesia
- Apply cold packs to reduce swelling
- Manual reduction: grasp and elongate the hernia neck with one hand; apply firm steady pressure to the proximal hernia at the neck with the other hand (NOT the distal end — pushing distally causes ballooning at the neck)
- After successful reduction: observe for serial abdominal exams; watch for reduction en masse
- Failed reduction or any sign of strangulation → immediate surgery; IV antibiotics + fluid resuscitation + surgical consult
Strangulated Hernia
- IV broad-spectrum antibiotics
- Fluid resuscitation
- Urgent/emergency surgical repair
- May require bowel resection
Pediatric Considerations
- Male:female ratio 10:1; right > left (right testis descends later)
- Spontaneous resolution does not occur → all confirmed pediatric inguinal hernias require surgical repair
- Premature infants at highest risk for incarceration due to narrow inguinal ring
- Usually performed as open herniorrhaphy (high ligation of sac); no floor repair needed
- Laparoscopic approach increasingly adopted (<2 years) — also allows simultaneous inspection of contralateral side
- Contralateral exploration: ~30% have patent processus vaginalis on the opposite side; options include laparoscopic inspection at time of repair
- Recurrence <1% in children (vs. ~1–5% in adults with mesh repair)
Complications of Surgical Repair
- Recurrence: ~1% with Lichtenstein mesh; higher with tissue repair
- Chronic groin pain (neuropathic): injury to ilioinguinal, iliohypogastric, or genitofemoral nerves
- Wound infection
- Seroma/hematoma
- Testicular atrophy: injury to testicular artery or vas deferens
- Mesh complications: infection, migration, erosion
- Overall complication rate: up to 20%
Sources: Schwartz's Principles of Surgery, 11e; Tintinalli's Emergency Medicine; Yamada's Textbook of Gastroenterology, 7e; Gray's Anatomy for Students
diabetes mellitus
Reading File
Finding Sources
Searching PubMed
"diabetes mellitus type 2"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"type 2 diabetes" AND treatment guidelines
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Create a comprehensive DM study guide
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Search for and compile medical images of diabetic complications
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
diabetes
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.