Fetal therapy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fetal therapy"[MeSH Terms] AND review
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Fetal Therapy
Fetal therapy encompasses all interventions directed at the fetus in utero - from medical treatments delivered transplacentally, to minimally invasive procedures, to open fetal surgery. The field has evolved from a controversial concept into standard-of-care management for several fetal anomalies.
1. Historical Background
The first open fetal surgical intervention was performed in 1981 by Dr. Michael Harrison at the University of California, San Francisco (UCSF), in a fetus with obstructive uropathy. Placement of a fetal vesicoamniotic shunt proved that intrauterine operation could be safe and maintain the pregnancy. Earlier limited procedures had existed since the 1960s, including fetal blood transfusion and amniocentesis. The successful randomized trial of placental laser coagulation in twin-twin transfusion syndrome (TTTS) later prompted widespread clinical acceptance of fetoscopy.
Today, maternal-fetal surgery takes three forms: open intervention via hysterotomy, minimally invasive fetoscopy, and percutaneous fetal access under ultrasound guidance.
(Sabiston Textbook of Surgery, 2025 ed.; Creasy & Resnik's Maternal-Fetal Medicine)
2. Conditions Amenable to Fetal Intervention
| Condition | Approach |
|---|---|
| Myelomeningocele (MMC) | Open repair or fetoscopic repair |
| Twin-twin transfusion syndrome (TTTS) | Fetoscopic laser photocoagulation |
| Twin reversed arterial perfusion (TRAP) | Radiofrequency ablation (RFA) / cord coagulation |
| Congenital diaphragmatic hernia (CDH) | Fetoscopic endoluminal tracheal occlusion (FETO) |
| Lower urinary tract obstruction | Vesicoamniotic shunt / fetal cystoscopy |
| Sacrococcygeal teratoma (SCT) | Open debulking or RFA |
| Congenital pulmonary airway malformation (CPAM) | Open resection or EXIT procedure |
| Fetal anemia | Intrauterine transfusion |
| Congenital high airway obstruction (CHAOS) / neck masses | EXIT procedure |
| Amniotic band syndrome | Fetoscopic band release |
| Congenital heart disease | Percutaneous balloon valvuloplasty |
| Renal agenesis / anhydramnios | Serial amniotransfusion (investigational - RAFT trial) |
(Sabiston Textbook of Surgery, Box 118.1)
3. Medical (Non-Surgical) Fetal Therapy
Treatment for infections, fetal cardiac arrhythmias, compromised thyroid function, and similar disorders is usually given to the mother and reaches the fetus by crossing the placenta. In selected cases, agents may be administered directly to the fetus by intramuscular injection into the gluteal region or via the umbilical vein.
Examples include:
- Fetal supraventricular tachycardia: digoxin, flecainide, or amiodarone given transplacentally or via cordocentesis
- Congenital adrenal hyperplasia: dexamethasone to suppress fetal adrenal androgen production
- Fetal thyroid disorders: transplacental levothyroxine or antithyroid drugs depending on the condition
(Langman's Medical Embryology)
4. Intrauterine (Fetal) Transfusion
In fetal anemia from maternal antibodies (hemolytic disease of the fetus) or other causes, ultrasound-guided needle insertion into the umbilical cord vein allows direct intravascular transfusion. This was historically the first fetal intervention (1960s) and remains a cornerstone of managing Rh isoimmunization.
5. Surgical Approaches
5a. Open Fetal Surgery
Open fetal surgery is performed between 18 and 30 weeks of gestation via laparotomy and hysterotomy under general endotracheal anesthesia (halogenated agents provide concurrent uterine relaxation). Key technical points:
- The uterus is opened with specially designed absorbable staples (Premium Poly CS 57) to prevent maternal hemorrhage
- The fetus is partially exteriorized, monitored by ultrasound, pulse oximetry, or fetal ECG
- Atropine + pancuronium/vecuronium are given directly to the fetus (via IM or umbilical vessels) to immobilize it and blunt the fetal stress response
- The fetus is kept warm by intrauterine Ringer's lactate infusion at body temperature
- Postoperatively, magnesium sulfate tocolysis is started; intraamniotic antibiotics are administered; the hysterotomy is covered with an omental flap
Risks of open fetal surgery:
- Preterm contractions, PROM, chorioamnionitis, maternal pulmonary edema
- Uterine dehiscence/rupture in subsequent pregnancies - 9.6% rate reported by the North American Fetal Therapy Network (NAFTNet) after prior open MMC repair
- All future deliveries must be by cesarean section after open maternal-fetal surgery
5b. Fetoscopic (Minimally Invasive) Surgery
Small-diameter endoscopes access the amniotic cavity through small maternal abdominal incisions. Compared to open surgery:
- Lower rate of uterine dehiscence (0% vs. ~11% in open MMC repair)
- Higher rate of PROM and dehiscence at the fetal repair site
- Patients can generally labor and deliver vaginally in current and future pregnancies
- Many procedures can be done under local anesthesia: fetoscopic laser for TTTS, RFA, fetal transfusion, shunt insertion, FETO
5c. Percutaneous Procedures (Ultrasound-Guided)
Needle-based interventions without fetoscopy: intrauterine transfusion, vesicoamniotic shunting, amniocentesis, amnioinfusion.
6. Specific Conditions in Detail
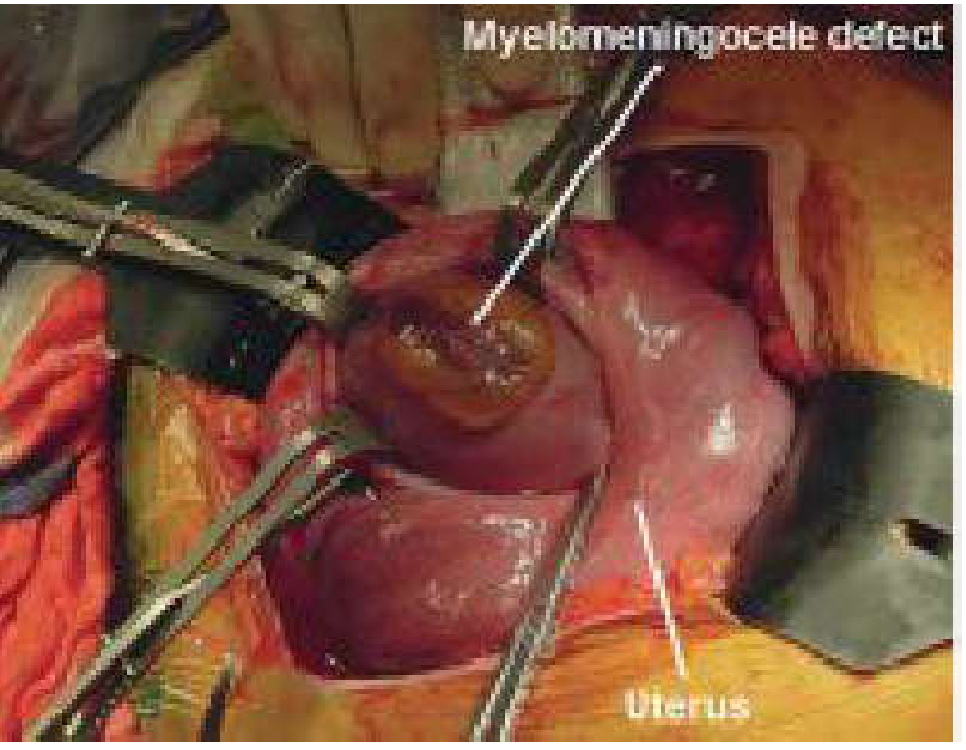
Myelomeningocele (MMC)
MMC is one of the most common congenital defects causing lifelong morbidity (approximately 4 children born daily in the US). The neural tube fails to close, exposing spinal cord tissue and leaking CSF. This leads to:
- Hindbrain herniation (Arnold-Chiari II malformation) and hydrocephalus
- Lifelong paralysis and bowel/bladder incontinence depending on spinal level
- Cognitive complications from cortical anomalies
Two-hit hypothesis: The first hit is the anomalous neural placode; the second hit is progressive spinal cord injury from mechanical trauma of the uterine wall and toxicity of amniotic fluid.
The MOMS Trial (Management of Myelomeningocele Study): This landmark RCT demonstrated that open prenatal repair reduced the need for VP shunting and improved motor outcomes, reversing hindbrain herniation. It revived open fetal surgery. In utero repair is now standard of care for selected patients.
Fetoscopic alternatives to open MMC repair have been developed to reduce the risk of uterine rupture in subsequent pregnancies, at the cost of higher PROM rates.
Twin-Twin Transfusion Syndrome (TTTS)
In monochorionic twins, abnormal arteriovenous anastomoses across the shared placenta cause a hemodynamic imbalance - the donor twin becomes hypovolemic/growth-restricted while the recipient becomes hypervolemic/hydropic. Staging (Quintero staging I-IV) guides management.
Fetoscopic laser photocoagulation of communicating placental vessels is the treatment for advanced TTTS (stages II-IV). It can be performed from 16 to 26 weeks' gestation. RCTs demonstrated:
- Survival of at least one twin improved from ~50% to ~75%
- Decreased neurologic complications compared to amnioreduction
- Increased risk of PROM and preterm delivery
Stage I TTTS management is debated; observational studies support expectant management, but 60% of stage I cases progress to needing urgent intervention - reinforcing the need for close monitoring.
Congenital Diaphragmatic Hernia (CDH)
Herniation of abdominal viscera into the thorax causes pulmonary hypoplasia and pulmonary hypertension. Fetoscopic Endoluminal Tracheal Occlusion (FETO) uses a balloon to temporarily occlude the fetal trachea, stimulating lung growth by accumulation of lung fluid. Early open CDH repair was abandoned due to high morbidity; FETO remains investigational with evolving evidence.
Lower Urinary Tract Obstruction (LUTO)
Posterior urethral valves or other obstructions lead to progressive renal dysplasia and oligohydramnios causing pulmonary hypoplasia. Goals of intervention:
- Vesicoamniotic shunt: percutaneously placed, diverts fetal urine to the amniotic cavity; 2-year survival ~40%
- Fetal cystoscopy: allows direct visualization and laser ablation of posterior urethral valves
- Serial amnioinfusion: investigational (RAFT trial - NCT03101891) for bilateral renal agenesis-related anhydramnios
Sacrococcygeal Teratoma (SCT)
Large SCTs may cause high-output cardiac failure and fetal hydrops. Open surgery aims to debulk the tumor and prevent cardiac failure. RFA can be used to interrupt tumor blood supply in selected cases.
Ex Utero Intrapartum Treatment (EXIT) Procedure
EXIT is a specialized cesarean delivery in which the fetus is partially delivered while uteroplacental circulation is preserved, allowing time to secure a fetal airway before complete delivery. Indications include:
- Laryngeal atresia / congenital high airway obstruction syndrome (CHAOS)
- Large cervical teratomas or head/neck tumors
- Micrognathia requiring complex intubation
- EXIT-to-ECMO for selected cardiac defects or CDH
- EXIT-to-resection for large CPAM
Performed under deep inhalational anesthesia for maximal uterine relaxation. Requires extensive multidisciplinary preparation with pre-assigned team roles.
7. Anesthesia and Perioperative Considerations
Pregnant patients undergoing fetal surgery have significant physiologic changes to account for:
- Increased cardiac output, decreased systemic vascular resistance
- Increased minute ventilation and oxygen consumption, decreased FRC
- Physiologic anemia from dilution; increased renal blood flow and GFR
- Risks of aspiration, difficult airway, and aortocaval compression in supine position
Tocolysis is administered before, during, and after surgery. Volatile agents (sevoflurane, isoflurane) are preferred for their dual role of anesthesia and uterine relaxation. Postoperative pain management typically uses epidural or bilateral quadratus lumborum blocks. Fetal heart rate and uterine activity are monitored continuously for 24-48 hours post-procedure.
(Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anesthesia 10e; Sabiston Textbook of Surgery)
8. Novel and Future Directions
In Utero Stem Cell Transplantation
Because the fetus lacks immunocompetence before ~18 weeks, tissue/cell transplantation before this window does not trigger rejection. Research focuses on hematopoietic stem cells for immunodeficiency and hematologic disorders (e.g., sickle cell disease, thalassemia, SCID).
In Utero Gene Therapy
Inherited metabolic diseases (e.g., Tay-Sachs, cystic fibrosis) are targets. The prenatal window offers advantages: smaller fetal size (lower vector dose needed), pre-immune state reducing immune response, and correction before irreversible organ damage.
Fetal Tissue Engineering
Placenta-derived mesenchymal stem cells (PMSCs) combined with extracellular matrix scaffolds are being studied for MMC repair. In a fetal sheep model, PMSC-ECM patches restored motor function. The first in-human clinical trial for fetal intervention in MMC with placental-derived stem cells was FDA-approved in 2020.
Transamniotic Stem Cell Therapy (TRASCET)
Concentrated amniotic mesenchymal stem cells delivered via intraamniotic injection have been shown to reduce bowel damage in rodent gastroschisis models, taking advantage of the dual wound-damage/wound-healing properties of amniotic fluid.
(Sabiston Textbook of Surgery, 2025; Langman's Medical Embryology)
9. Ethical Considerations
Maternal-fetal surgery involves two patients simultaneously - the fetus and the pregnant woman. The pregnant patient assumes all procedural risks for the sake of fetal benefit. Historically, interventions were restricted to uniformly lethal conditions to justify maternal risk. As safety improved, indications broadened. Informed consent must include detailed counseling about maternal risks (including uterine rupture risk in all future pregnancies after open surgery), fetal risks, and alternatives, including postnatal repair or expectant management.
The overall mortality rate of open fetal surgery is approximately 6%; the Achilles' heel remains control of preterm labor - prematurity must be weighed against any potential benefit of prenatal intervention.
Key References:
- Sabiston Textbook of Surgery, Chapter 118 - Maternal-Fetal Surgery
- Creasy & Resnik's Maternal-Fetal Medicine, Chapter 34 - Fetal Surgery
- MOMS Trial (Adzick et al., 2011) - landmark RCT for MMC repair
- Langman's Medical Embryology - Fetal Therapy overview
- Miller's Anesthesia 10e - Anesthesia for Open Fetal Surgery
Create a summary table of fetal therapy indications and outcomes
Here is a comprehensive summary table of fetal therapy indications and outcomes, synthesized from the textbook sources reviewed:
Fetal Therapy: Indications, Interventions & Outcomes
| Condition | Pathophysiology | Intervention | Timing (Gestation) | Key Outcomes | Main Risks/Complications |
|---|---|---|---|---|---|
| Myelomeningocele (MMC) | Incomplete neural tube closure → exposed spinal cord; Arnold-Chiari II + hydrocephalus; progressive spinal cord injury from amniotic fluid toxicity ("2nd hit") | Open hysterotomy repair (MOMS trial) or fetoscopic MMC repair | 18-26 weeks | Reduced VP shunt need; improved motor function; reversal of hindbrain herniation; lower incidence of Chiari malformation | PROM, preterm labor; 9.6% uterine rupture in subsequent pregnancy after open repair; overall mortality ~6%; fetoscopic = higher PROM but no uterine rupture |
| Twin-Twin Transfusion Syndrome (TTTS) | Arteriovenous placental anastomoses → donor hypovolemia / recipient hypervolemia and hydrops | Fetoscopic laser photocoagulation of communicating placental vessels | 16-26 weeks | Survival of at least one twin improved from ~50% to ~75%; decreased neurologic complications vs. amnioreduction | PROM, preterm delivery; stage I may be managed expectantly but 60% progress to requiring intervention |
| Twin Reversed Arterial Perfusion (TRAP) sequence | Acardiac twin acts as parasitic pump, causing high-output failure in co-twin | Radiofrequency ablation (RFA) or fetoscopic cord coagulation | 2nd trimester | Cessation of blood flow to acardiac mass; improved pump twin survival | PROM, preterm delivery, fetal loss |
| Congenital Diaphragmatic Hernia (CDH) | Herniation of abdominal viscera → pulmonary hypoplasia + pulmonary hypertension | Fetoscopic Endoluminal Tracheal Occlusion (FETO) - balloon tracheal occlusion to stimulate lung growth | 27-30 weeks (balloon); removed ~34 weeks | Increased lung volume; evidence still evolving from RCTs (TOTAL trial); benefit mainly in severe CDH | PROM, preterm labor; EXIT-to-ECMO also used perinatally; early open repair was abandoned due to high morbidity |
| Lower Urinary Tract Obstruction (LUTO) | Posterior urethral valves / obstruction → renal dysplasia, oligohydramnios → pulmonary hypoplasia | Vesicoamniotic shunt (percutaneous) or fetal cystoscopy + laser ablation of posterior urethral valve | 2nd trimester | 2-year pooled survival ~40% after shunting; cystoscopy allows direct valve ablation restoring bladder cycling | Shunt dislodgement/migration; PROM; irreversible renal damage if delayed; poor renal function despite intervention |
| Fetal Anemia (Rh isoimmunization / hemolytic disease) | Maternal alloantibodies → fetal hemolysis → severe anemia, hydrops fetalis | Intrauterine intravascular transfusion (IUT) via umbilical vein under ultrasound guidance | From ~18 weeks onward; repeated as needed | Corrects anemia; reversal of hydrops; survival >90% in non-hydropic fetuses; ~70-80% in hydropic fetuses | Bradycardia, fetal distress, cord hematoma, PROM, infection |
| Sacrococcygeal Teratoma (SCT) | High-output cardiac failure / hydrops from vascular steal by large tumor | Open surgical debulking or RFA to interrupt tumor vascularity | Late 2nd / early 3rd trimester (only if hydrops developing) | Prevention of cardiac failure and fetal death in selected hydropic cases; most non-hydropic cases managed postnatally | High fetal mortality if hydrops present; significant maternal morbidity with open approach |
| Congenital Pulmonary Airway Malformation (CPAM) | Large lesion → mediastinal shift, hydrops, pulmonary hypoplasia | Open fetal lobectomy (if hydrops); EXIT-to-resection at delivery | 2nd trimester (open); at delivery (EXIT) | Hydrops reversal and survival in selected cases; most small CPAMs managed postnatally | High risk with open approach; prematurity |
| Congenital High Airway Obstruction / Neck Masses (CHAOS, cervical teratoma) | Airway obstruction at birth; can't intubate or ventilate after delivery | EXIT (Ex Utero Intrapartum Treatment) procedure - partial delivery preserving uteroplacental circulation while airway is secured | At delivery (~37-38 weeks) | Successful airway establishment before clamping cord; survival where otherwise fatal | Maternal hemorrhage; uterine atony; very complex multidisciplinary logistics required |
| Amniotic Band Syndrome | Fibrous bands cause limb/digit/facial constriction or amputation | Fetoscopic band release | 2nd trimester | Limb/digit salvage; improved function if done before ischemic damage | Technically demanding; PROM; fetal loss |
| Fetal Cardiac Arrhythmias (SVT, atrial flutter) | Re-entrant or ectopic tachycardia → fetal hydrops | Transplacental antiarrhythmics (digoxin, flecainide, sotalol, amiodarone) ± direct fetal drug administration | Any trimester when diagnosed | Conversion to sinus rhythm in ~60-80% with transplacental therapy; direct therapy reserved for refractory cases or hydrops | Drug toxicity (maternal + fetal); incomplete conversion; recurrence |
| Congenital Adrenal Hyperplasia (CAH) | 21-hydroxylase deficiency → fetal androgen excess → virilization of female genitalia | Maternal dexamethasone (transplacental) started before 9 weeks | Before 9 weeks (must start before sex determination) | Reduces virilization of affected female fetuses; must start empirically before karyotype result | Treatment of 7 out of 8 fetuses unnecessarily (only 1/8 = affected female); maternal side effects; long-term fetal safety debated |
| Fetal Thyroid Disorders | Fetal hypothyroidism or hyperthyroidism (maternal antibodies or drug effect) | Intraamniotic levothyroxine (for hypothyroid) or maternal antithyroid drugs adjustment (for hyperthyroid) | 2nd-3rd trimester | Normalization of fetal thyroid function; improved neurodevelopment; reduced goiter | Technically challenging; requires serial monitoring |
| Renal Agenesis / Anhydramnios (bilateral) | No urine production → lethal pulmonary hypoplasia | Serial amniotransfusion (investigational - RAFT trial NCT03101891) | 2nd trimester | Restoration of amniotic fluid; potential for lung development - efficacy still under investigation | PROM, infection, preterm labor; renal failure remains if kidneys absent |
| Gastroschisis (novel approach) | Abdominal viscera outside cavity; amniotic fluid toxicity damages bowel | Transamniotic Stem Cell Therapy (TRASCET) - intraamniotic injection of mesenchymal stem cells (preclinical/early trials) | 2nd trimester | Reduced bowel damage in rodent models; early human feasibility being explored | Investigational only; safety profile in development |
Key Principles Governing Patient Selection
- The condition must have a predictable natural history that is uniformly severe or lethal without intervention
- No reasonable postnatal alternative should exist that could achieve equivalent outcomes
- Intervention must offer demonstrable fetal benefit that outweighs maternal and fetal procedural risk
- Prematurity risk must be weighed against benefit - preterm birth remains the primary Achilles' heel of all fetal surgery
- Procedures should only be performed in specialist centers with trained multidisciplinary teams (fetal medicine, MFM surgery, neonatology, anesthesia, NICU)
(Sources: Sabiston Textbook of Surgery 2025, Creasy & Resnik's Maternal-Fetal Medicine, Langman's Medical Embryology, Mulholland & Greenfield's Surgery 7e)
Exit procedure
Finding Sources
Searching PubMed
"ex utero intrapartum treatment" AND airway
Reading File
Finding Sources
Reading Article
PMID: 40746351
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive detail from multiple textbooks. Here is the full structured answer.
The EXIT Procedure (Ex Utero Intrapartum Treatment)
Definition and Core Concept
The EXIT procedure is a specialized cesarean delivery technique in which the fetus is only partially delivered through a uterotomy, with the umbilical cord kept intact and uteroplacental circulation fully preserved, while the surgical team secures the fetal airway or performs other interventions. Only once a safe, functional airway is established is the cord clamped and the baby fully delivered.
The essential principle is "placental bypass" - the placenta continues to provide fetal gas exchange while the team works, eliminating the time pressure of postnatal asphyxia.
The concept was first developed in 1990, when a fetus underwent laryngoscopy and intubation prior to umbilical cord clamping. Previously, an ENT/airway team would simply be "on standby" to establish the airway under extreme time pressure after normal delivery - a far more dangerous scenario.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Creasy & Resnik's Maternal-Fetal Medicine)
Indications
EXIT was initially used to remove tracheal occlusion balloons placed in fetuses with congenital diaphragmatic hernia (CDH) who had undergone fetoscopic tracheal occlusion (FETO) to stimulate lung growth. Its indications have since expanded substantially.
Primary Indications (Airway Obstruction)
| Condition | Notes |
|---|---|
| Congenital High Airway Obstruction Syndrome (CHAOS) | Laryngeal atresia, laryngeal web, subglottic stenosis - tracheostomy required at delivery |
| Cervical teratoma | Large, often displacing or compressing the trachea; worse prognosis than compressible masses |
| Cystic hygroma / lymphatic malformation | Compressible; better prognosis than solid teratomas |
| Lymphangioma / hemangioma | If causing significant airway compression |
| Micrognathia (severe) | May require bronchoscopy and complex intubation |
| Cervical neuroblastoma / other neck masses | Any mass causing predicted airway compromise |
Extended Indications
| Condition | Approach |
|---|---|
| Removal of FETO balloon (CDH after tracheal occlusion) | Original historical indication |
| CPAM (congenital pulmonary airway malformation) | EXIT-to-resection; cord pH/CO2 remain normal even after >2.5 hours |
| Sacrococcygeal teratoma | EXIT-to-resection in selected large lesions |
| Congenital cardiac defects | EXIT-to-ECMO - ECMO circuit established before cord clamping |
| Conjoined twins | Complex separation requiring cardiac/pulmonary support at delivery |
An EXIT procedure for airway-obstructing neck masses reduces mortality from 10-57% to 8%, a dramatic improvement over conventional delivery.
(Scott-Brown's Otorhinolaryngology; Miller's Anesthesia 10e; Creasy & Resnik)
Comparison: EXIT vs. OOPS (Operation on Placental Support)
These are the two main interventional delivery strategies - it is important to distinguish them:
| Feature | EXIT | OOPS |
|---|---|---|
| Delivery extent | Head (+ possibly one shoulder) only, partially delivered | Whole baby delivered onto a Mayo table; cord left intact |
| Anaesthetic | Traditionally inhalational GA (greater uterine relaxation); regional also possible | Regional anaesthetic or short GA |
| Uterine relaxation | Deep - achieved by high-dose volatile agent | Minimal - cord spasm limits time anyway |
| Time window available | 20-50 minutes | 5-20 minutes (cord goes into spasm) |
| Maternal haemorrhage risk | Higher (uterine atony from deep anaesthesia) | Lower |
| Conversion | Can be converted to OOPS if needed | Cannot be converted to EXIT |
| Preferred when | Complex airway anticipated; longer procedure needed | Simpler airway cases; regional anaesthetic preferred |
A third option - delivery then attempted intubation/tracheostomy - is reserved for situations where maternal haemorrhage risk is prohibitive (e.g., large uterine fibroids), and the paediatric airway team is simply standing by after standard caesarean section.
Anesthesia for EXIT
This is one of the most complex anaesthetic scenarios in all of obstetrics, requiring simultaneous management of two patients with conflicting needs.
Goals
- Deep uterine relaxation - to maintain uterine volume, prevent placental separation, and preserve uteroplacental blood flow during the entire procedure
- Maternal safety - prevent haemorrhage, maintain maternal haemodynamics
- Fetal analgesia/immobility - prevent fetal movement during airway intervention
Technique
- Inhalational general anaesthesia is the classical approach: high-dose volatile agents (sevoflurane, isoflurane, desflurane) provide both anaesthesia and profound uterine relaxation
- Regional anaesthesia (spinal or combined spinal-epidural) can be used if supplemented with tocolytics (e.g., nitroglycerin, magnesium sulfate) to achieve uterine relaxation - this reduces maternal haemorrhage risk but requires careful planning
- Maternal risks from GA include: uterine atony and haemorrhage (the most important), failed/difficult airway, aspiration
- Large-bore IV access and preparation for massive transfusion are mandatory
Fetal Management
- Fetal analgesics and immobilizing agents (atropine + pancuronium/vecuronium) given IM or via umbilical vessels
- Continuous fetal heart rate monitoring throughout
- Fetal pulse oximetry or intermittent echocardiography
Preoperative Planning: The MDT Approach
EXIT is emphatically a team procedure. Thorough pre-EXIT rehearsal and planning are mandatory. The multidisciplinary team includes:
- Fetal medicine / MFM surgeon - uterotomy and maternal monitoring during the procedure
- Obstetric anaesthetist - maternal GA/regional, uterine relaxation
- Paediatric anaesthetist (ENT-specialist preferred) - primary intubator
- ORL/ENT surgeon(s) - recommended to have two consultants:
- One "intubating" consultant (with rigid bronchoscopy skills)
- One "tracheostomy" consultant (ready to act if intubation fails, with fresh focus)
- Neonatology / PICU team - postnatal resuscitation and transport
- Paediatric surgeon - if resection planned (EXIT-to-resection)
- Perfusionist / cardiac surgery - if EXIT-to-ECMO planned
- Scrub nurses and ODP with experience in the procedure
The team meets before seeing the parents to agree on the birth plan. A contingency plan for emergency presentation in spontaneous labour before the planned date must also be prepared, with on-call MDT awareness.

Step-by-Step Surgical Sequence
- Prenatal diagnosis confirmed by high-resolution ultrasound and fetal MRI (for extent of airway compression, tracheal displacement, lung volume)
- Corticosteroids administered before planned delivery to promote fetal lung maturation
- Planned elective LSCS at 36-38 weeks (earlier if polyhydramnios increases preterm labour risk)
- Maternal GA induced with high-dose volatile agent for deep uterine relaxation
- Laparotomy and uterotomy (lower segment); placental position determined in advance
- Partial delivery - fetal head (+/- shoulder) delivered; umbilical cord kept intact; uterine volume maintained to preserve uteroplacental perfusion
- Airway intervention performed (20-50 minute window):
- Direct laryngoscopy
- Rigid bronchoscopy
- Endotracheal intubation
- Tracheostomy (if intubation impossible)
- Surfactant administration
- Tumour/mass debulking or resection if planned
- Airway confirmed secure (CO2 detection, chest rise, SpO2)
- Cord clamped - baby fully delivered
- Neonatal team takes over - NICU/PICU resuscitation
- Uterotomy closed; oxytocin administered to deliver placenta; manage uterine atony
Timing of Delivery
| Situation | Timing |
|---|---|
| Standard planned EXIT | 36-38 weeks (after antenatal corticosteroids) |
| Polyhydramnios present | Earlier delivery - increased preterm labour risk |
| Rapidly enlarging mass with worsening compression | Earlier, guided by fetal wellbeing and lung maturity |
| FETO balloon removal | Balloon removed at ~34 weeks, then delivery planned |
Outcomes and Prognosis
- Overall mortality for airway-obstructing neck masses falls from 10-57% to ~8% with EXIT vs. conventional delivery
- Isolated airway obstruction (no other anomaly) - good prognosis with experienced team
- Multiple fetal anomalies or lung hypoplasia present - prognosis is less favourable
- Lymphatic malformations (cystic hygromas) - better prognosis than cervical teratomas (compressible vs. solid)
- EXIT-to-ECMO and EXIT-to-resection for CPAM - normal umbilical cord gas values documented even after surgical times exceeding 2.5 hours, demonstrating the safety of the uteroplacental window
Risks and Complications
Maternal
- Uterine atony and haemorrhage - the primary risk; greater with GA than regional
- Difficult maternal airway (pregnancy-related airway changes)
- Aspiration
- Prolonged hysterotomy increases risk vs. standard caesarean
Fetal/Neonatal
- Placental abruption / placental separation if uterine volume not maintained
- Fetal bradycardia
- Failed airway - managed by immediate tracheostomy (hence the two ENT consultants)
- Prematurity complications if delivered early
Key Points Summary
- EXIT = partial delivery + intact cord + secured airway, then full delivery
- Time window: 20-50 minutes (vs. 5-20 min for OOPS)
- Requires deep uterine relaxation - high-dose volatile GA is standard; regional + tocolytics is an alternative
- Two ENT consultants recommended - one intubating, one ready for tracheostomy
- Delivery planned at 36-38 weeks after corticosteroids
- Mortality for airway neck masses reduced from up to 57% → 8% with EXIT
- Must only be performed in specialist centres with full MDT including ECMO capability
(Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2; Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anesthesia 10e; Sabiston Textbook of Surgery 2025; Gaffuri et al., Front Pediatr 2025 - PMID 40746351)
This is a shared conversation. Sign in to Orris to start your own chat.