Development of fore hind and mid gut
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full, well-structured answer.
Development of the Foregut, Midgut, and Hindgut
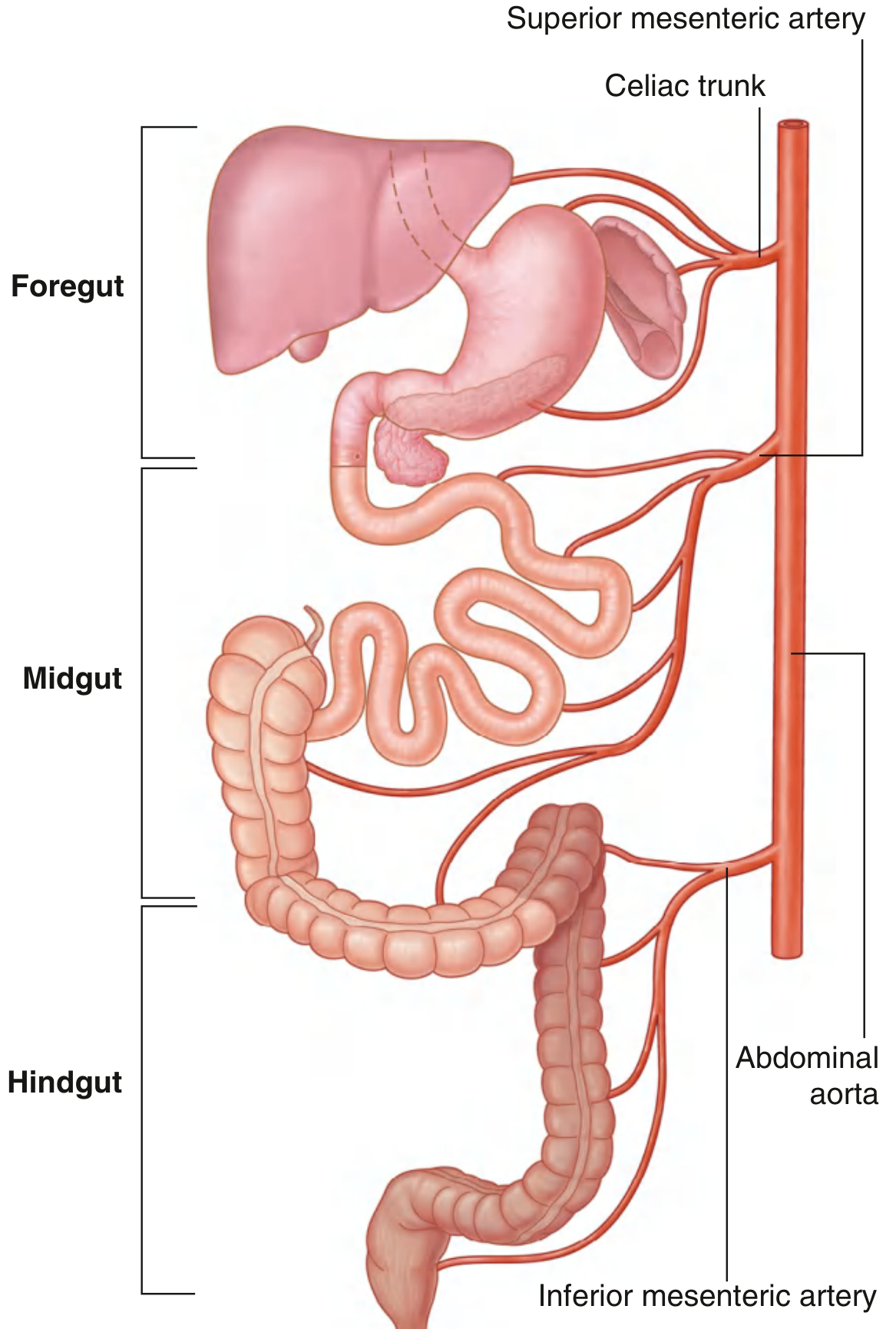
Blood supply to the three divisions of the primitive gut - celiac trunk (foregut), superior mesenteric artery (midgut), inferior mesenteric artery (hindgut)
Overview: Primordial Gut Formation
The alimentary system forms from the primordial gut, which develops during the 4th week of embryogenesis when the head fold, caudal (tail) fold, and lateral folds incorporate the dorsal part of the umbilical vesicle (yolk sac). Initially, the gut is closed at:
- The cranial end by the oropharyngeal membrane
- The caudal end by the cloacal membrane
The gut wall is formed from endoderm (epithelium and glands) + splanchnic mesoderm (smooth muscle, connective tissue, blood vessels). The epithelium at the cranial and caudal extremities is derived from ectoderm of the stomodeum and proctodeum (anal pit), respectively.
Regional differentiation of the primordial gut is regulated by Hox and ParaHox genes, and signaling molecules Shh, BMP, and Wnt.
1. FOREGUT
Extent and Blood Supply
The foregut extends from the oropharyngeal membrane to just beyond the opening of the bile duct into the duodenum. It is supplied by the celiac trunk (artery of the foregut).
Derivatives
| Structure | Notes |
|---|---|
| Primordial pharynx | Pharyngeal arches/pouches |
| Lower respiratory system | Larynx, trachea, lungs (via respiratory diverticulum) |
| Esophagus | Caudal to pharynx |
| Stomach | Fusiform dilation of foregut |
| Duodenum (proximal to bile duct opening) | Derived from caudal foregut + cranial midgut |
| Liver and biliary apparatus | Hepatic buds from caudal foregut endoderm |
| Pancreas | Dorsal and ventral buds from caudal foregut |
Esophagus
- Develops from the foregut immediately caudal to the pharynx
- The tracheoesophageal septum partitions the respiratory diverticulum from the esophagus (4th week)
- Initially short; elongates rapidly due to descent of the heart and lungs; reaches final length by week 7
- Lumen temporarily obliterated by epithelial proliferation, then recanalizes by week 8
- Upper 1/3 muscularis: striated muscle (from pharyngeal arch mesenchyme), innervated by vagus nerve (CN X)
- Lower 1/3 muscularis: smooth muscle (from splanchnic mesenchyme)
- Key anomaly: Esophageal atresia (1:3000-4500 births) - associated with tracheoesophageal fistula in >90% of cases
Stomach
- Begins as a fusiform dilation of the foregut in week 4, in the primitive thoracic region
- Undergoes two rotations:
- Rotation around longitudinal axis (90° clockwise): left side becomes anterior (greater curvature); right side becomes posterior (lesser curvature) - this also explains why the left vagus nerve becomes the anterior gastric nerve
- Rotation around dorsoventral axis: gastric antrum shifts upward to the right, while fundus shifts down and left - gives the stomach its final position
- Forms the omental bursa (lesser sac) as it rotates
- Key anomaly: Hypertrophic pyloric stenosis (1:150 males) - hypertrophy of pyloric musculature causing projectile vomiting
Duodenum
- Develops from caudal foregut + cranial midgut - junction is just distal to the bile duct origin
- Grows into a C-shaped loop projecting ventrally (week 4), then rotates to the right and becomes retroperitoneal
- Lumen temporarily obliterated (week 5-6) then recanalizes
- Supplied by both celiac trunk and superior mesenteric artery (dual origin)
- Key anomaly: Duodenal atresia - failure of recanalization; associated with Down syndrome and polyhydramnios ("double bubble" sign on X-ray)
Liver and Biliary Apparatus
- The hepatic diverticulum (liver bud) grows from the caudal foregut endoderm into the septum transversum (mesoderm) at ~day 25
- Liver cord cells proliferate into the septum transversum, which thins to form the falciform ligament, lesser omentum, and peritoneum of the liver
- The hematopoietic function begins in week 6; the liver is the main hematopoietic organ in the fetus until week 12, when the spleen takes over
- The gallbladder and cystic duct arise from the hepatic diverticulum
- Key anomaly: Biliary atresia - progressive obliteration of bile ducts; acholic (clay-colored) stools, jaundice, dark urine
Pancreas
- Arises from dorsal and ventral pancreatic buds of the caudal foregut endoderm
- The dorsal bud (larger) appears first; gives rise to most of the pancreas (body, tail, part of head)
- The ventral bud (near bile duct) rotates with the duodenum (clockwise), swings behind and fuses with the dorsal bud
- Ventral bud forms the uncinate process and part of the head
- The main pancreatic duct (of Wirsung) = duct of ventral bud + distal dorsal bud duct
- Accessory duct (of Santorini) = proximal portion of dorsal bud duct
- Key anomaly: Annular pancreas - failure of ventral bud rotation; ring of pancreatic tissue encircles duodenum causing obstruction
2. MIDGUT
Extent and Blood Supply
The midgut extends from just beyond the bile duct opening in the duodenum to the junction of the proximal 2/3 and distal 1/3 of the transverse colon. Supplied entirely by the superior mesenteric artery (SMA) - which forms the axis of the primary intestinal loop.
Derivatives
| Structure |
|---|
| Distal duodenum (below bile duct) |
| Jejunum |
| Ileum |
| Cecum and appendix |
| Ascending colon |
| Right 2/3 of transverse colon |
Primary Intestinal Loop and Physiological Herniation
- Rapid elongation of the midgut forms the primary intestinal loop, connected at its apex to the yolk sac via the vitelline (omphaloenteric) duct
- The loop has a cranial (cephalic) limb - forms distal duodenum, jejunum, and part of ileum
- Caudal limb - forms distal ileum, cecum, appendix, ascending colon, proximal 2/3 transverse colon
- Due to rapid growth of the gut and liver, the abdominal cavity cannot accommodate the intestinal loops - they herniate into the umbilical cord around week 6 (physiological umbilical herniation)
Rotation of the Midgut Loop
The midgut loop undergoes a total 270° counterclockwise rotation (viewed from front) around the axis of the SMA, in three steps of 90° each:
| Step | Rotation | Result |
|---|---|---|
| 1 (weeks 6-10, in cord) | 90° CCW | Cranial limb goes right; caudal limb goes left |
| 2 (return to abdomen, week 10) | 90° CCW | Cecum briefly under liver then descends |
| 3 (final fixation) | 90° CCW | Cecum descends to right iliac fossa |
Retraction and Fixation (Week 10)
- Intestinal loops return to the abdomen as the liver and kidneys grow relatively smaller
- Small intestine occupies the center; colon forms its final positions
- The cecum descends from just below the liver to the right iliac fossa; the appendix develops as a small outgrowth of the cecum
Key Anomalies
- Malrotation: Incomplete 270° rotation (e.g., only 90°); colon and cecum settle on the left; predisposes to volvulus and vascular compromise
- Reversed rotation (90° clockwise): Transverse colon passes behind the duodenum
- Omphalocele: Failure of the gut to return to the abdominal cavity; gut covered by peritoneum/amnion (associated with chromosomal defects)
- Gastroschisis: Protrusion through the body wall lateral to umbilicus; gut NOT covered by peritoneum (not associated with chromosomal defects; increasing in young mothers)
- Meckel's diverticulum: Persistence of the vitelline duct (~2-4% of population); ~40-60 cm from ileocecal valve on anti-mesenteric border; may contain ectopic gastric or pancreatic tissue; "rule of 2s"
- Vitelline fistula: Patent vitelline duct from umbilicus to ileum; fecal discharge at umbilicus
3. HINDGUT
Extent and Blood Supply
The hindgut extends from the distal 1/3 of the transverse colon to the cloacal membrane. Supplied by the inferior mesenteric artery (IMA).
Derivatives
| Structure |
|---|
| Distal 1/3 transverse colon |
| Descending colon |
| Sigmoid colon |
| Rectum |
| Superior part of anal canal (down to pectinate line) |
| Epithelium of bladder and urethra (from cloaca) |
The Cloaca and its Partitioning
- The hindgut terminates in the cloaca - a dilated chamber lined with endoderm, in contact with surface ectoderm at the cloacal membrane
- The urorectal septum (wedge of mesoderm) grows caudally and divides the cloaca into:
- Dorsal part: anorectal canal (future rectum and upper anal canal)
- Ventral part: urogenital sinus (bladder, urethra, lower vagina)
- The urorectal septum fuses with the cloacal membrane by week 7, dividing it into an anal membrane (dorsal) and a urogenital membrane (ventral)
Anal Canal Formation
The anal canal has a dual origin - reflected by the histological landmark of the pectinate (dentate) line:
| Feature | Above Pectinate Line | Below Pectinate Line |
|---|---|---|
| Origin | Hindgut endoderm | Ectodermal proctodeum |
| Epithelium | Simple columnar | Stratified squamous |
| Arterial supply | Superior rectal artery (IMA) | Inferior rectal artery (internal pudendal) |
| Venous drainage | Portal system (internal hemorrhoids above) | Systemic (external hemorrhoids below) |
| Lymph drainage | Internal iliac nodes | Superficial inguinal nodes |
| Nerve supply | Autonomic (pain insensitive) | Somatic (pain sensitive) |
The anal membrane ruptures around week 9, establishing patency of the anal canal.
Key Anomalies
- Anorectal agenesis / imperforate anus: Failure of the anal membrane to rupture, or abnormal development of the urorectal septum; most common anorectal malformation
- Rectovesical, rectovaginal, or rectourethral fistulas: Result from incomplete division of the cloaca by the urorectal septum
- Hirschsprung disease (congenital megacolon): Failure of neural crest cell migration into the hindgut wall (absence of Meissner's and Auerbach's plexuses); functional obstruction, most commonly involving the rectosigmoid
Summary Table
| Division | Arterial Supply | Derivatives |
|---|---|---|
| Foregut | Celiac trunk | Pharynx, esophagus, stomach, proximal duodenum (above bile duct), liver, gallbladder, pancreas, spleen |
| Midgut | Superior mesenteric artery | Distal duodenum, jejunum, ileum, cecum, appendix, ascending colon, proximal 2/3 transverse colon |
| Hindgut | Inferior mesenteric artery | Distal 1/3 transverse colon, descending colon, sigmoid, rectum, upper anal canal, bladder/urethra epithelium |
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.), Ch. 11 - Alimentary System; Langman's Medical Embryology, Ch. 15 - Digestive System
This is a shared conversation. Sign in to Orris to start your own chat.