Russell silver syndrome
Reading File
Finding Sources
Searching PubMed
Russell Silver syndrome
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Searching Images
Russell Silver syndrome clinical features child triangular face
Loading Image
Finding Sources
I now have sufficient information from the textbooks and literature to deliver a comprehensive answer on Russell-Silver Syndrome.
Russell-Silver Syndrome (RSS / SRS)
Russell-Silver syndrome (RSS, also written Silver-Russell syndrome/SRS) is a clinically and genetically heterogeneous congenital growth disorder first described independently by Silver (1953) and Russell (1954).
Clinical Features
Cardinal Features
| Feature | Detail |
|---|---|
| Intrauterine growth restriction (IUGR) | Low birth weight despite normal gestational age |
| Postnatal growth retardation | Short stature persisting after birth |
| Triangular face / small face | Broad forehead tapering to small, pointed chin; micrognathia |
| Relative macrocephaly | Head circumference relatively preserved → "pseudohydrocephalic" appearance |
| Body asymmetry / hemihypoplasia | One side of body (limbs, trunk) smaller than the other |
| Clinodactyly of the 5th finger | Radial curvature of both little fingers |
Additional Features
- Café-au-lait macules (CALMs) — 1–2 spots in up to 20% of patients
- Feeding difficulties, hypoglycemia (especially neonatal)
- Blue sclera (rare association)
- Precocious puberty (listed as a cause of isosexual precocity)
- ART (assisted reproductive technology) increases risk of RSS
Clinical Photos
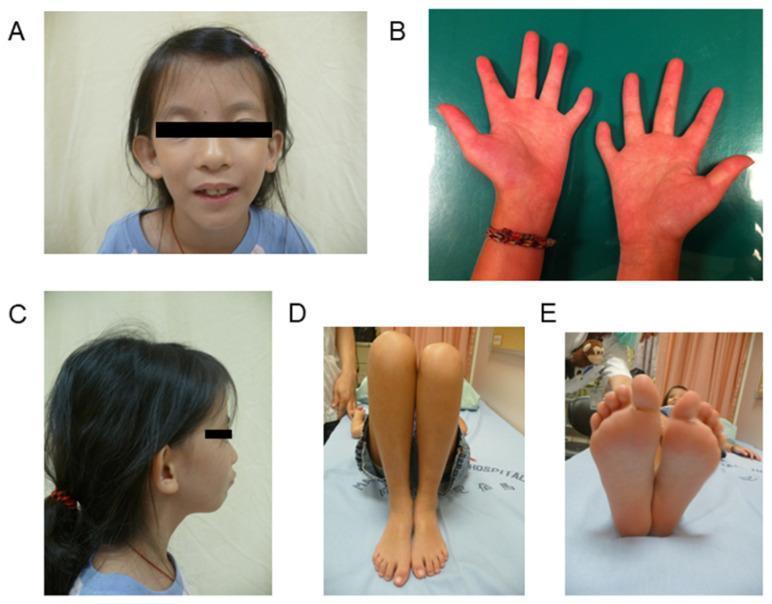
Classic SRS phenotype: triangular face, hemihypoplasia of the right hand, limb length discrepancy, and foot size asymmetry.
Molecular Genetics & Pathogenesis
RSS is a paradigm of genomic imprinting disorders, involving chromosome 11p15.5 and chromosome 7.
Chromosome 11p15.5 (most common — 35–65% of cases)
The 11p15 locus contains two independently regulated imprinted domains (DMR1 and DMR2):
- DMR1 (ICR1) controls IGF2 and H19
- Normally: IGF2 is expressed only from the paternal allele; H19 from the maternal allele
- In RSS: Hypomethylation of H19/ICR1 → loss of IGF2 expression from both alleles → reduced IGF2 → growth retardation
- Contrast with Beckwith-Wiedemann syndrome (BWS): hypermethylation of DMR1 → upregulated IGF2 → overgrowth
- DMR2 (ICR2): No altered methylation has been found in RSS (unlike BWS)
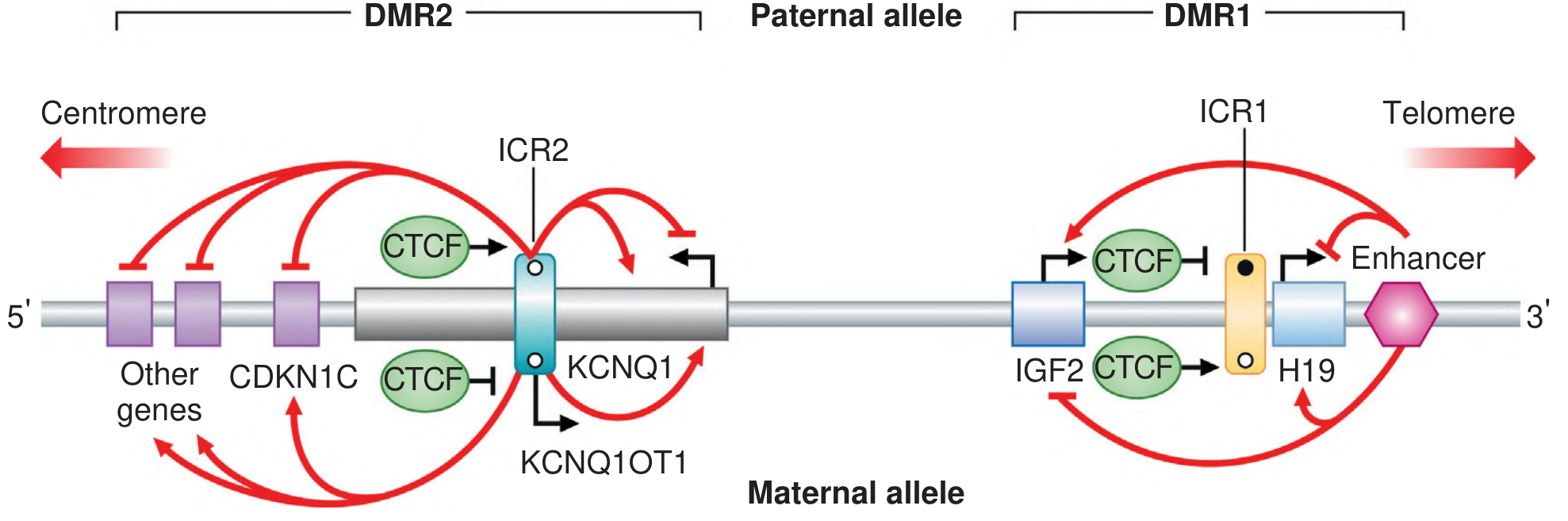
Fig: Imprinted domains at 11p15.5. ICR1 controls IGF2/H19; ICR2 controls KCNQ1/CDKN1C. In RSS, hypomethylation of ICR1 silences IGF2 expression, causing growth restriction.
Chromosome 7 (~10% of cases)
- Maternal uniparental disomy of chromosome 7 (UPD7mat) — patient inherits both chromosomes 7 from the mother
- Candidate regions: 7p11.2–p13, 7q31–qter, 7q21
Maternally derived duplications of 11p15
- Paternally derived duplications of 11p15 → BWS (overgrowth)
- Maternally derived duplications of 11p15 → RSS (growth retardation)
Other causes
- Mutations on chromosome 17q and other loci (minority of cases)
- Many cases remain genetically unexplained
RSS vs. Beckwith-Wiedemann Syndrome — Epigenetic Mirror Images
| Feature | RSS | BWS |
|---|---|---|
| 11p15.5 ICR1 methylation | Hypomethylated (loss) | Hypermethylated (gain) |
| IGF2 expression | Decreased | Increased |
| Growth | Retarded (pre- and postnatal) | Overgrowth |
| Chromosomal mechanism | Mat UPD7 or hypo-ICR1 | Pat UPD11 or hyper-ICR1 |
Diagnosis
RSS is a clinical diagnosis supported by molecular testing. The Netchine-Harbison Clinical Scoring System (NH-CSS) is widely used (≥4/6 criteria suggests RSS; molecular testing warranted if ≥3):
- SGA (small for gestational age) — birth weight and/or length ≤ −2 SD
- Postnatal growth retardation — height ≤ −2 SD at ≥24 months
- Relative macrocephaly at birth — head circumference ≥ 1.5 SD above birth weight/length SD
- Body asymmetry (limb length discrepancy ≥0.5 cm or facial asymmetry)
- Feeding difficulties or BMI ≤ −2 SD at 24 months
- Prominent forehead / frontal bossing
Molecular workup:
- Methylation testing of 11p15.5 (ICR1 hypomethylation)
- UPD7 testing (microsatellite analysis or SNP array)
- Chromosomal microarray
- If negative but high clinical suspicion: exome sequencing
Management
- Growth hormone (GH) therapy: Approved for SRS with short stature — improves adult height; should be started early (typically 2–4 years of age)
- Nutritional support: High-risk for neonatal hypoglycemia; nasogastric feeding may be required in infants
- Orthopedic management: Limb length discrepancy may require shoe lifts or leg-lengthening procedures
- Dental/orthodontic care: Due to micrognathia and crowded dentition
- Monitoring for precocious puberty: Can limit final height gain
- Multidisciplinary team: Pediatric endocrinology, genetics, dietetics, developmental pediatrics, physiotherapy
Inheritance & Recurrence
- Most cases are sporadic
- Familial cases exist with variable inheritance (AD, AR, and imprinting-related mechanisms described)
- ART-conceived children have higher rates of RSS and other imprinting disorders (Angelman, Prader-Willi) — likely due to epigenetic errors during early embryonic development
Key Sources
- Emery's Elements of Medical Genetics and Genomics — Genomic Imprinting chapter
- Fitzpatrick's Dermatology — Silver-Russell Syndrome, p. 1391
- Kurup U et al. "Approach to the Patient With Suspected Silver-Russell Syndrome." J Clin Endocrinol Metab, 2024 [PMID: 38888172]
This is a shared conversation. Sign in to Orris to start your own chat.