Myopectineal orifices
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have rich content from three authoritative surgical textbooks. Let me compile a comprehensive answer.
Myopectineal Orifice (MPO) of Fruchaud
Definition and Historical Background
The myopectineal orifice is the medial aspect of the superior gap between the pelvis and the thigh - a large, musculoaponeurotic "weak spot" in the lower abdominal wall. In 1956, the French anatomist and surgeon Henri René Fruchaud first described the term and the concept that weakening of this orifice is the underlying cause of all hernias in the inguinal region (direct inguinal, indirect inguinal, and femoral).
Wide reinforcement of the MPO has become the foundation of modern groin hernia repair in adults.
- Sabiston Textbook of Surgery, p. 1683
Anatomy
The MPO is bounded by:
| Border | Structure |
|---|---|
| Superior | Aponeurotic arch of the transversus abdominis and internal oblique muscles |
| Inferior | Pectineal line (pecten pubis / Cooper's ligament) |
| Medial | Lateral edge of the rectus abdominis |
| Lateral | Iliopsoas muscle |
The inguinal ligament (Poupart's ligament) crosses the orifice obliquely but does NOT form a true anatomical barrier - it is merely an anterior fascial structure and does not close off the gap, which is why it cannot prevent herniation.
The iliopectineal arch (a condensation of the iliopsoas fascia) divides the inferior part into:
- Lateral (muscular) space - transmits the iliopsoas complex and femoral nerve
- Medial (vascular) space - transmits the femoral artery, vein, and the femoral canal (the potential space for femoral hernias)
The classic anatomical diagram:
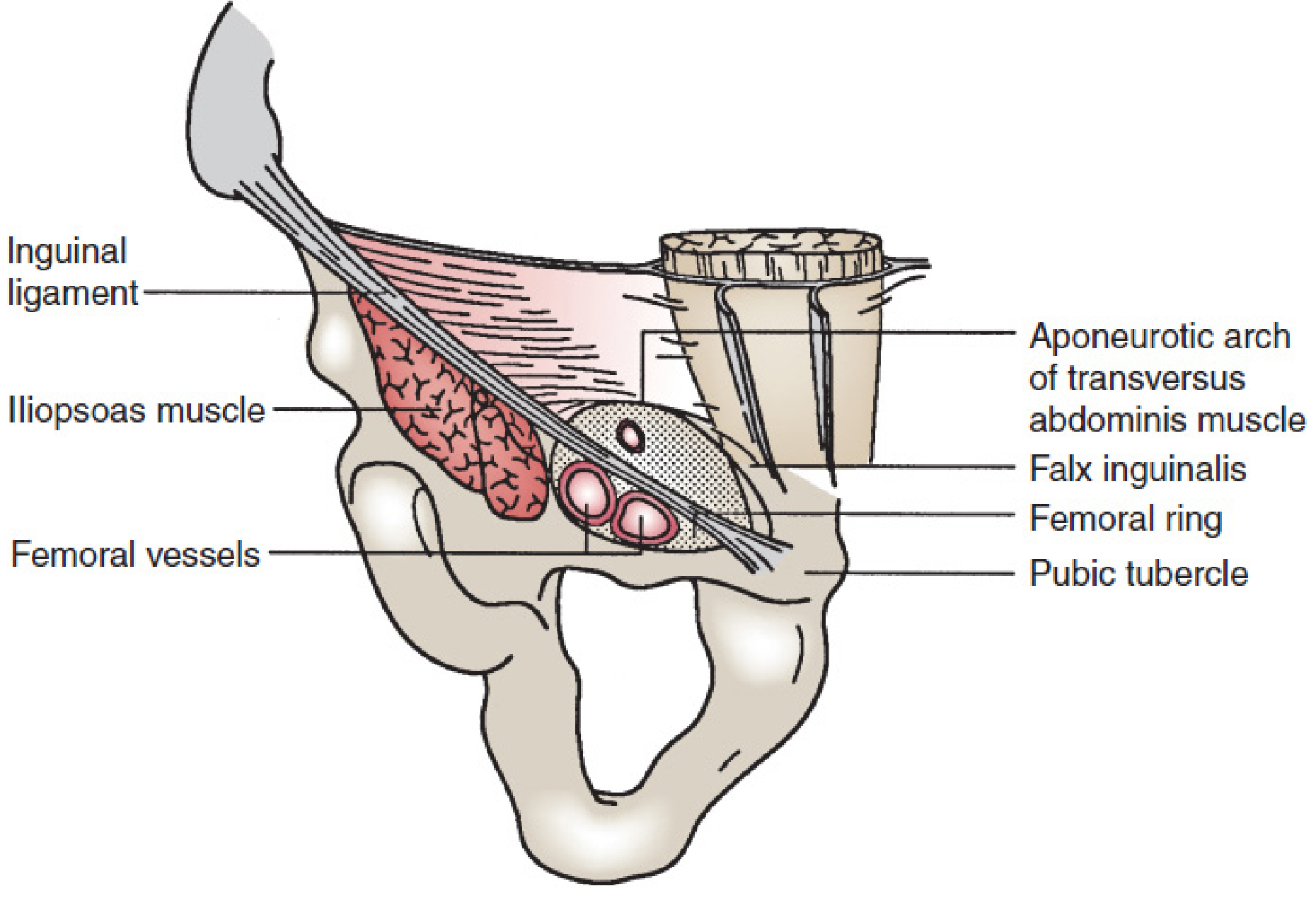
The MPO - superior to the inguinal ligament includes Hesselbach's (inguinal) triangle; inferior to the ligament, the orifice transmits the iliopsoas muscle, femoral nerve and vessels, and the femoral canal/sheath. (From Wantz GE, Atlas of Hernia Surgery, Raven Press, 1991)
- Mulholland and Greenfield's Surgery, p. 3632
Hernia Types Through the MPO
All groin hernias pass through the MPO:
| Hernia Type | Location within MPO |
|---|---|
| Indirect inguinal | Through the internal (deep) inguinal ring - lateral to inferior epigastric vessels |
| Direct inguinal | Through Hesselbach's triangle - medial to inferior epigastric vessels, above inguinal ligament |
| Femoral | Through the femoral canal - below the inguinal ligament, medial to the femoral vein |
This unifying concept is why a single large mesh covering the entire MPO (rather than separate repairs for each defect) forms the basis of preperitoneal hernia repair.
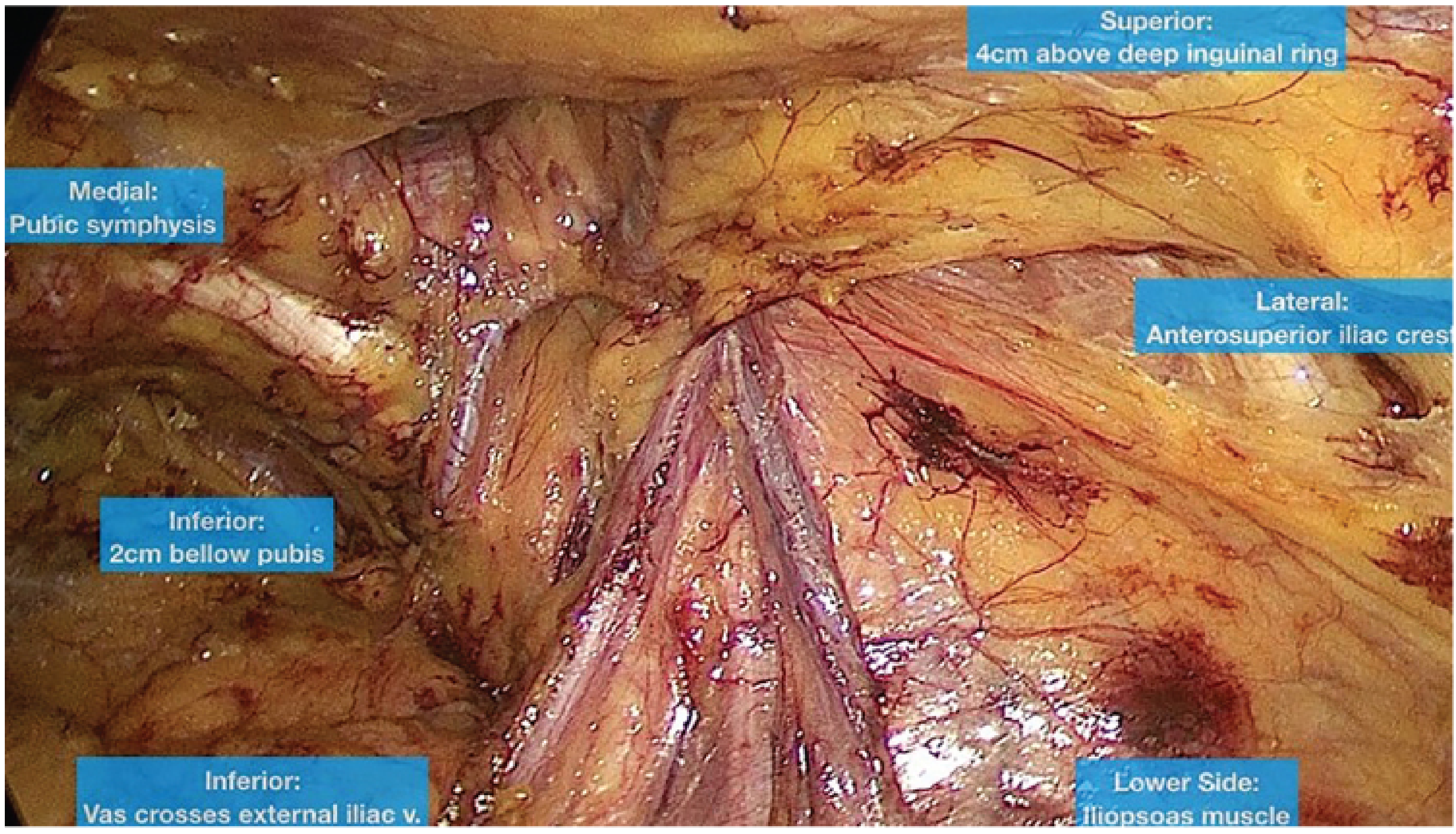
Surgical Significance: The Critical View of the MPO
The Critical View of the Myopectineal Orifice (CV-MPO) - first described by Daes and Felix (2017) - is the standardized anatomic exposure that must be achieved before mesh placement in any minimally invasive inguinal hernia repair (laparoscopic TEP or TAPP). It ensures no hernia is missed and reduces complications and recurrence.
The MPO is conceptually divided into three zones for this purpose:
| Zone | Contents |
|---|---|
| Zone 1 (Lateral) | Indirect/lateral space - psoas muscle, cord structures, deep inguinal ring |
| Zone 2 (Medial) | Direct space - Hesselbach's triangle, Cooper's ligament, pubic symphysis, Space of Retzius |
| Zone 3 (Inferior/Vascular) | Femoral space - femoral canal, external iliac vein, corona mortis area |
The 9 Steps to Achieve the Critical View:
- Identify and dissect the pubis across the midline and Cooper's ligament (Zone 2)
- Rule out a direct hernia by clearing fat from Hesselbach's triangle
- Dissect at least 2 cm between Cooper's ligament and the bladder (Space of Retzius)
- Rule out femoral hernia by dissecting between Cooper's ligament and the external iliac vein (Zone 3)
- Thoroughly dissect peritoneum and indirect hernia sac off the spermatic cord/round ligament
- Identify the vas deferens and gonadal vessels - parietalize the cord (reduce the indirect sac)
- Dissect peritoneum laterally toward ASIS to create Space of Bogros (Zone 1 lateral space)
- Visualize the entire MPO including all critical structures in Zones 1, 2, and 3
- Only then - place mesh (minimum 15 x 10 cm, no creases or folds)
The intraoperative appearance after achieving the Critical View:
- Fischer's Mastery of Surgery, 8th ed., p. 6101
Mesh Coverage
For both TEP and TAPP repair, the mesh must cover the entire MPO with adequate overlap:
- Medial: At least to the pubic symphysis (across to contralateral Cooper's ligament if direct hernia present)
- Superior: 3-4 cm above the internal inguinal ring onto the anterior abdominal wall
- Inferior: 1-2 cm below the pubis, into the Space of Retzius
- Lateral: Lying against the psoas muscle
- Minimum size: 15 x 10 cm (some guidelines recommend 14 x 11 cm or larger)
- The mesh must not be split around the cord
Repairs performed in the preperitoneal space (TEP, TAPP, Stoppa) that cover the entire MPO make the traditional distinction between direct, indirect, and femoral hernias surgically irrelevant - all are addressed simultaneously by covering the single defective fascial region.
- Mulholland and Greenfield's Surgery, p. 3814
- Sabiston Textbook of Surgery, p. 1685
Key Anatomical Hazards Within the MPO
When dissecting in the preperitoneal space to expose the MPO, several structures demand respect:
- Corona mortis - aberrant obturator artery/vein crossing Cooper's ligament, connecting inferior epigastric and obturator vessels; can bleed catastrophically if injured
- Triangle of Doom - between vas deferens (medially) and gonadal vessels (laterally); contains the external iliac vessels - no staples or tacks here
- Triangle of Pain - lateral to the gonadal vessels; contains the femoral branch of the genitofemoral nerve and the lateral femoral cutaneous nerve - no fixation here
- Genitofemoral nerve (genital and femoral branches) run posterior to the transversalis sling (TS) on the surface of the psoas
- Femoral nerve runs deep within the psoas, emerging laterally beneath the inguinal ligament
Inguinal hernia from basic to detail using more diagrams
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Inguinal Hernia - Basic to Detailed
1. What Is a Hernia?
A hernia is the protrusion of a viscus (or part of one) through a defect in the wall of its containing cavity. An inguinal hernia specifically involves abdominal contents (fat, omentum, bowel) protruding through a weakness in the groin (inguinal) region. It is the most common hernia in both sexes, and about 10 times more common in men than women.
2. Overview: Sites of Abdominal Wall Hernias
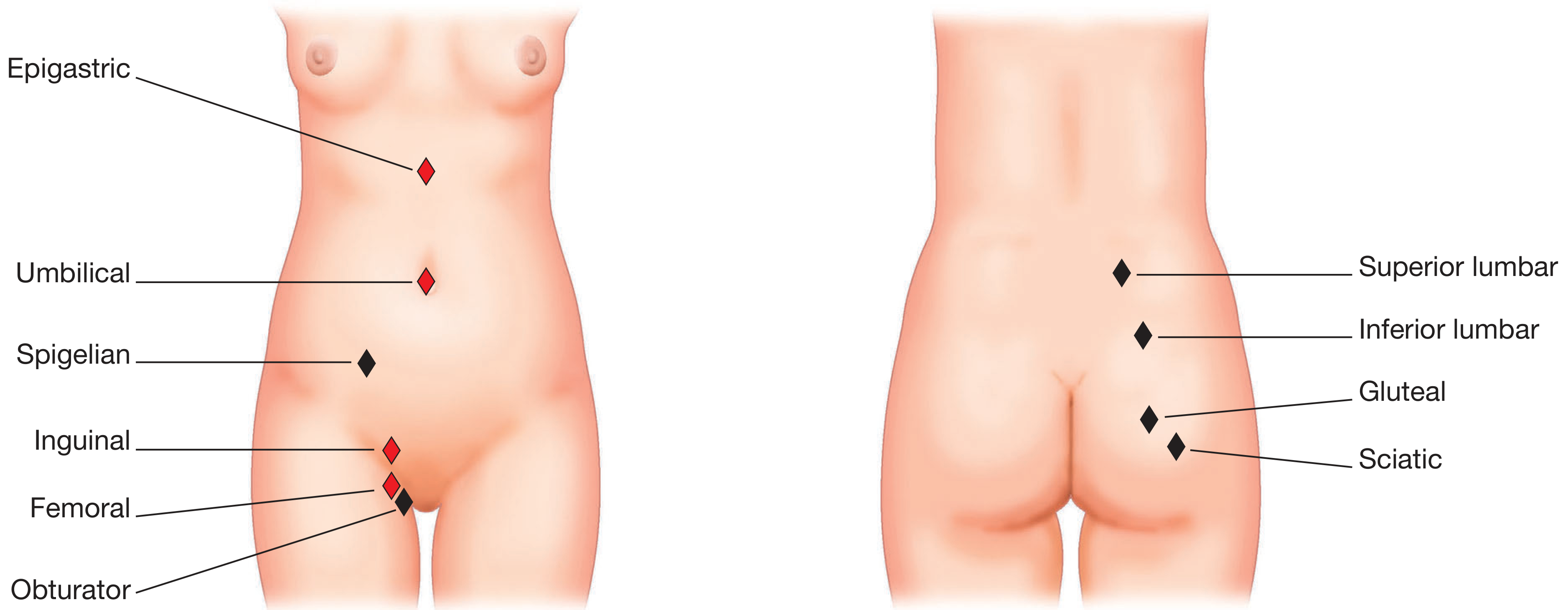
Sites of abdominal wall hernias. Inguinal (shown in red = common) lies in the groin above the inguinal ligament; femoral is just below it. - Bailey & Love's Surgery, 28th ed.
3. Anatomy of the Inguinal Canal
The inguinal canal is an oblique, 4 cm long tunnel through the lower abdominal wall running from the deep (internal) inguinal ring to the superficial (external) inguinal ring. It carries the spermatic cord in males and the round ligament in females.
Walls of the Inguinal Canal
| Wall | Structure |
|---|---|
| Anterior | External oblique aponeurosis (full length); internal oblique muscle (lateral 1/3) |
| Posterior | Transversalis fascia (full length); conjoint tendon (medial 1/3) |
| Roof | Arching fibers of internal oblique and transversus abdominis |
| Floor | Inguinal (Poupart's) ligament; lacunar ligament medially |
Rings
- Deep (internal) inguinal ring: A defect in the transversalis fascia. Lies at the midpoint of the inguinal ligament (midway between ASIS and pubic tubercle), ~2-3 cm above the femoral artery pulse. The inferior epigastric vessels run just medial to this ring - this is the key landmark distinguishing direct from indirect hernias.
- Superficial (external) inguinal ring: An inverted V-shaped defect in the external oblique aponeurosis, just above and medial to the pubic tubercle.
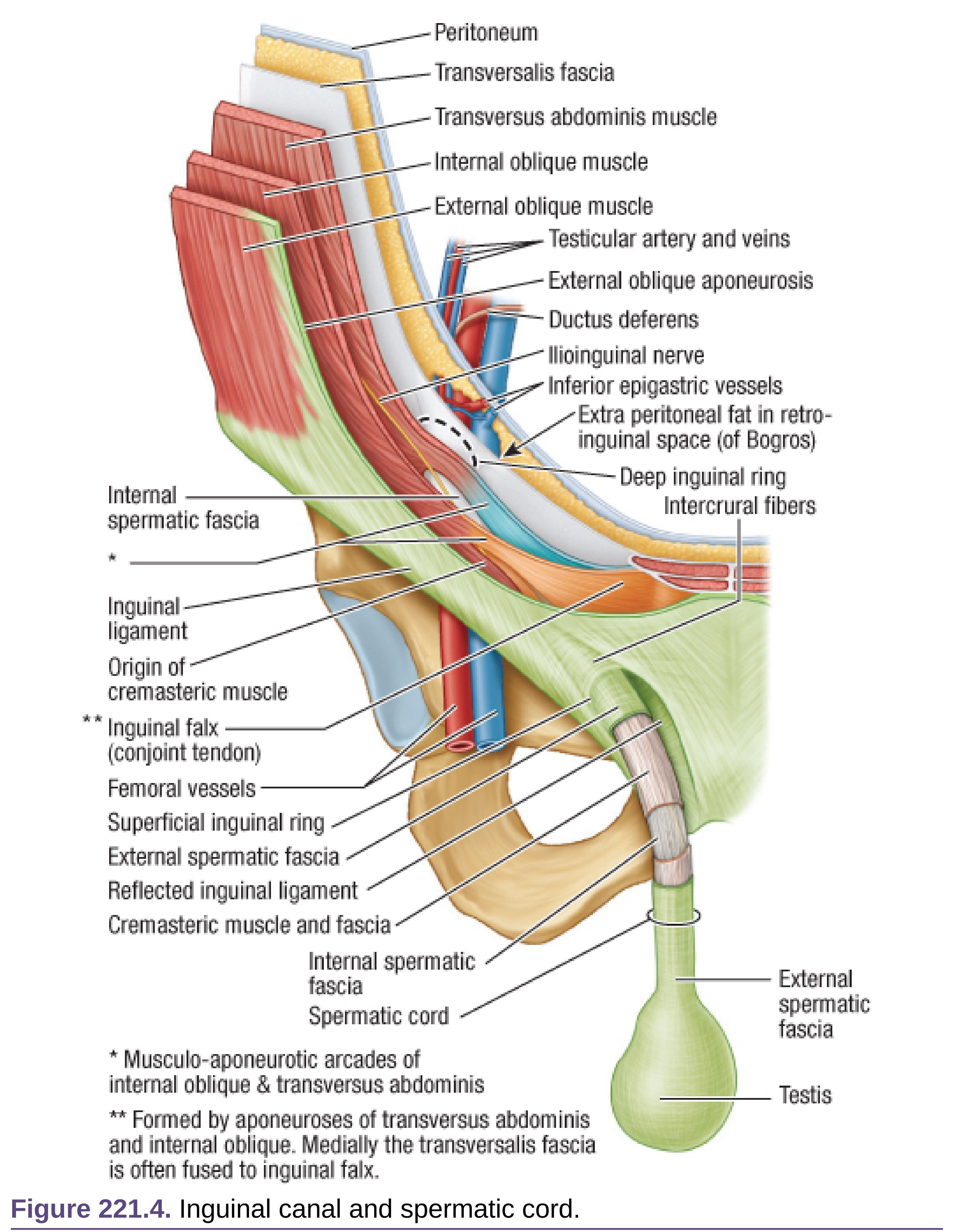
The inguinal canal and spermatic cord in full anatomical detail. Fischer's Mastery of Surgery, 8th ed.
Contents of the Inguinal Canal
In males (spermatic cord):
- Vas deferens
- Testicular artery and veins (pampiniform plexus)
- Cremasteric artery and vein
- Artery to vas deferens
- Genital branch of the genitofemoral nerve
- Cremasteric muscle fibers (from internal oblique)
- Lymphatics from the testis
In both sexes: ilioinguinal nerve (runs inside canal but outside cord)
In females: round ligament of the uterus
4. Hesselbach's Triangle
This is the anatomical weak spot through which direct hernias protrude.
| Border | Structure |
|---|---|
| Medial | Lateral border of the rectus abdominis |
| Superolateral | Inferior epigastric vessels |
| Inferior | Inguinal ligament (iliopubic tract) |
The triangle is weak because the posterior wall here consists of only transversalis fascia covered by the external oblique aponeurosis - no muscle reinforcement.
5. Types of Inguinal Hernia

Close relationships of direct inguinal, indirect inguinal, and femoral hernia sacs. Bailey & Love's Surgery, 28th ed.
Indirect (Lateral / Oblique) Inguinal Hernia
- Exits the peritoneum lateral to the inferior epigastric vessels, through the deep inguinal ring
- Follows the path of testicular descent (along the processus vaginalis)
- The hernia sac is a constituent of the spermatic cord - covered by internal spermatic fascia, cremasteric fascia, and external spermatic fascia
- Can descend all the way into the scrotum (inguinoscrotal hernia)
- Can be congenital (patent processus vaginalis) or acquired
- More common in young males and on the right side (right testis descends later)
Direct (Medial) Inguinal Hernia
- Exits medial to the inferior epigastric vessels, directly through the thinned transversalis fascia in Hesselbach's triangle
- Does NOT enter the inguinal canal - pushes directly forward and out of the superficial ring
- The hernia sac lies adjacent to (not within) the spermatic cord
- Always acquired - due to progressive weakening of the abdominal wall
- More common in elderly males
- Broadly based - rarely strangulates (in contrast to indirect hernias)
- The bladder can be pulled into a direct hernia (sliding direct hernia)
Comparison Table
| Feature | Indirect | Direct |
|---|---|---|
| Origin | Lateral to inferior epigastric vessels | Medial to inferior epigastric vessels |
| Exits through | Deep inguinal ring | Hesselbach's triangle |
| Sac relation to cord | Within spermatic cord | Medial/adjacent to cord |
| Cause | Congenital or acquired | Always acquired |
| Age | Young and old | Middle-aged / elderly |
| Descends to scrotum | Yes | Rarely |
| Strangulation risk | Higher | Low |
| Relation to IEV | Lateral | Medial |
6. Laparoscopic View of the Three Hernia Defects
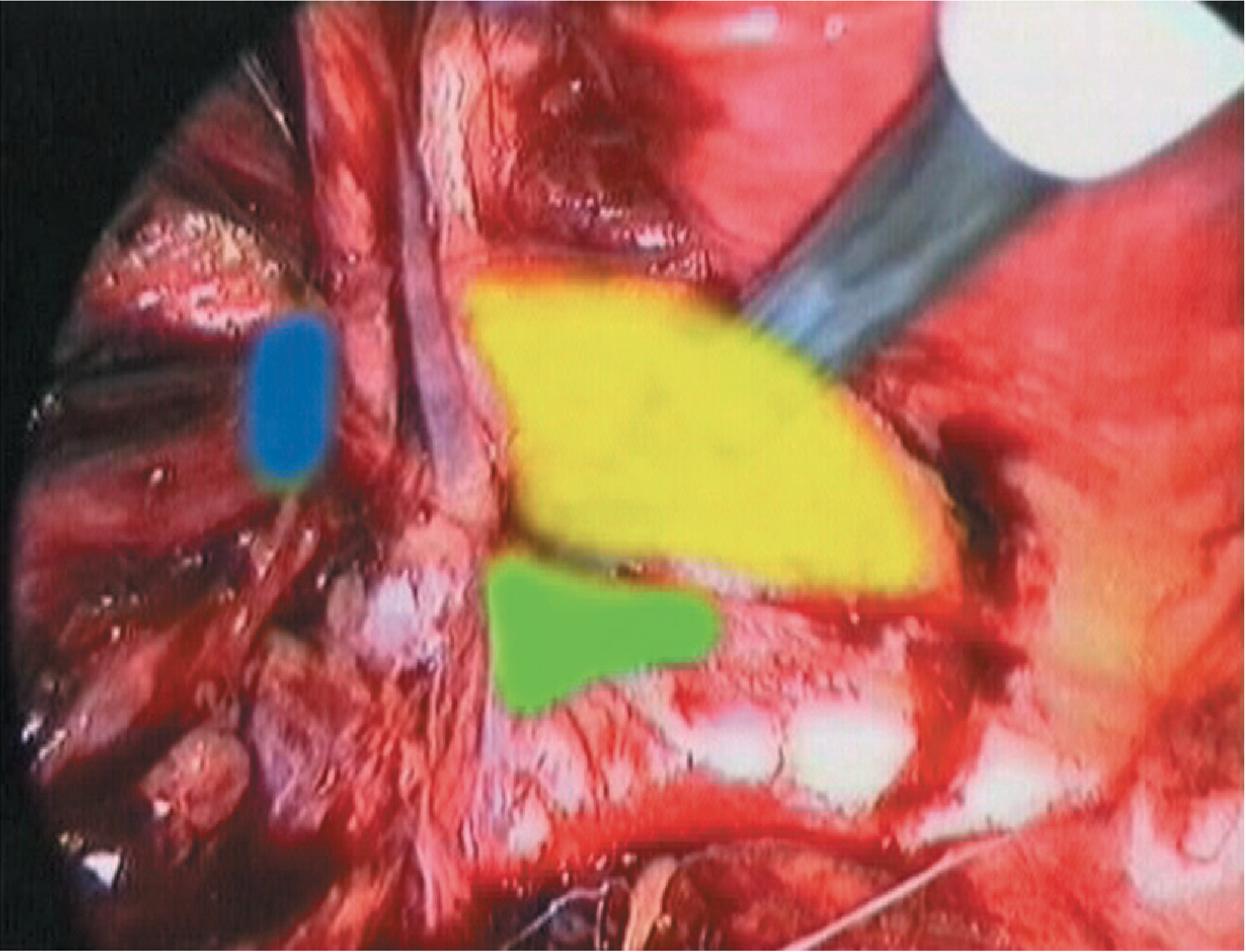
Laparoscopic view of the left inguinal region: yellow = direct (Hesselbach's triangle), blue = indirect (lateral), green = femoral. Bailey & Love's Surgery, 28th ed.
7. Special Types
Sliding Hernia
An acquired indirect hernia where retroperitoneal fat is pushed down and pulls peritoneum with it secondarily - the hernia sac itself forms part of the wall of a viscus (bladder on left side, caecum/sigmoid on respective sides). Extra caution at operation - the bowel forms part of the sac wall.
Pantaloon (Saddlebag) Hernia
Both a direct and an indirect hernia are present simultaneously on the same side, straddling the inferior epigastric vessels like a pair of trousers.
Inguinoscrotal Hernia
A large indirect hernia that has descended into the scrotum. Has no upper limit palpable on scrotal examination (cf. a hydrocele, which does have an upper limit).
Richter's Hernia
Only part of the circumference of the bowel (the antimesenteric wall) is caught in the hernia neck. Partial strangulation can occur without intestinal obstruction.
8. Embryology - Why Indirect Hernias Occur
During fetal development, the testis descends from the retroperitoneum to the scrotum. It carries with it a finger-like projection of peritoneum - the processus vaginalis - which becomes the tunica vaginalis. This processus normally obliterates a few months before birth. If it remains patent (especially in premature infants), bowel within the peritoneal cavity can pass inside the tube toward the scrotum - producing an indirect inguinal hernia.
- This explains why all congenital hernias are indirect
- It explains the higher incidence in premature infants
- Partial closure produces a hydrocele; full patency produces a communicating hydrocele or hernia
9. Detailed Topographic Anatomy of Inguinal Hernias
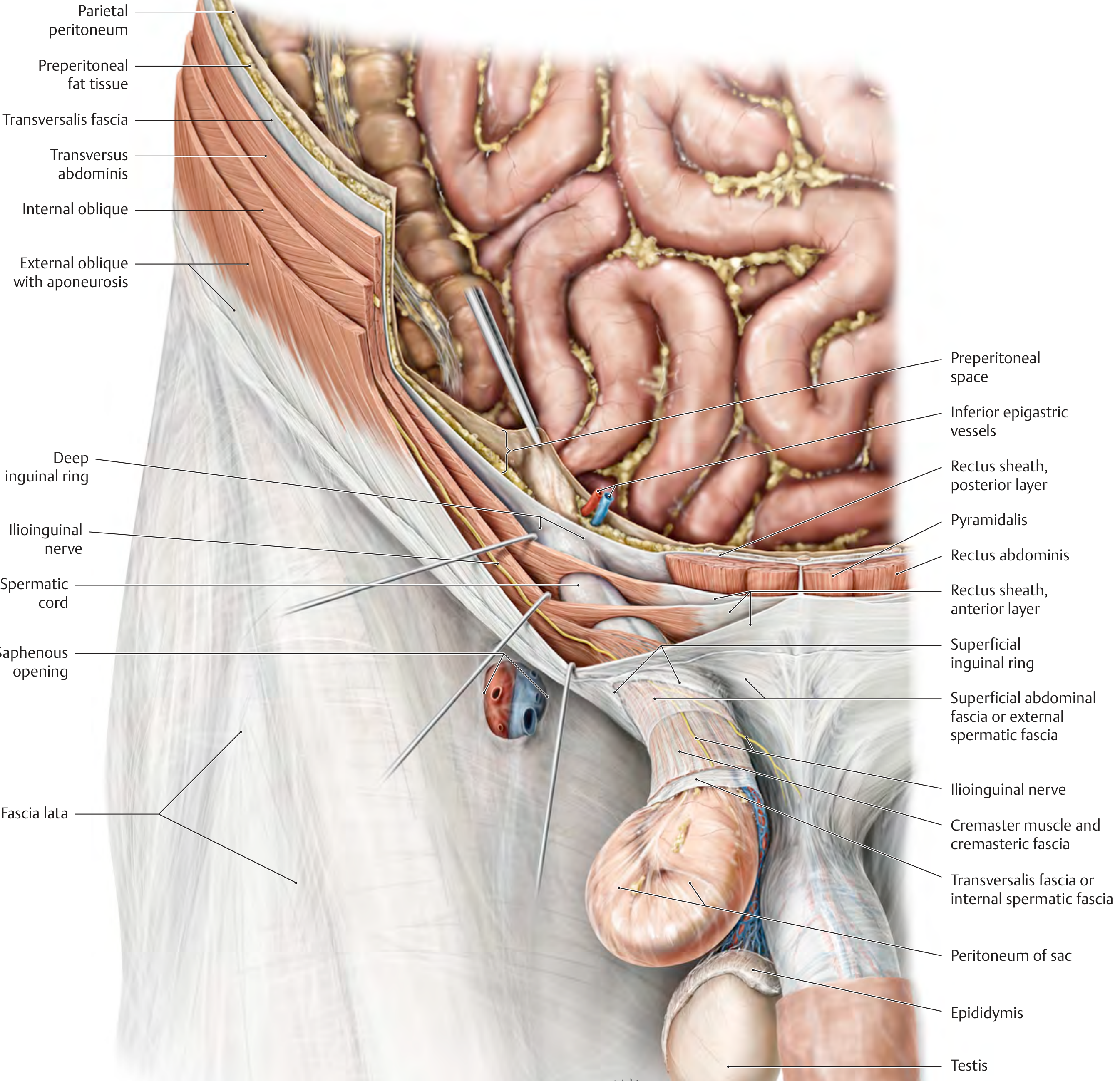
Topographic anatomy of an indirect inguinal hernia in male. THIEME Atlas of Anatomy.
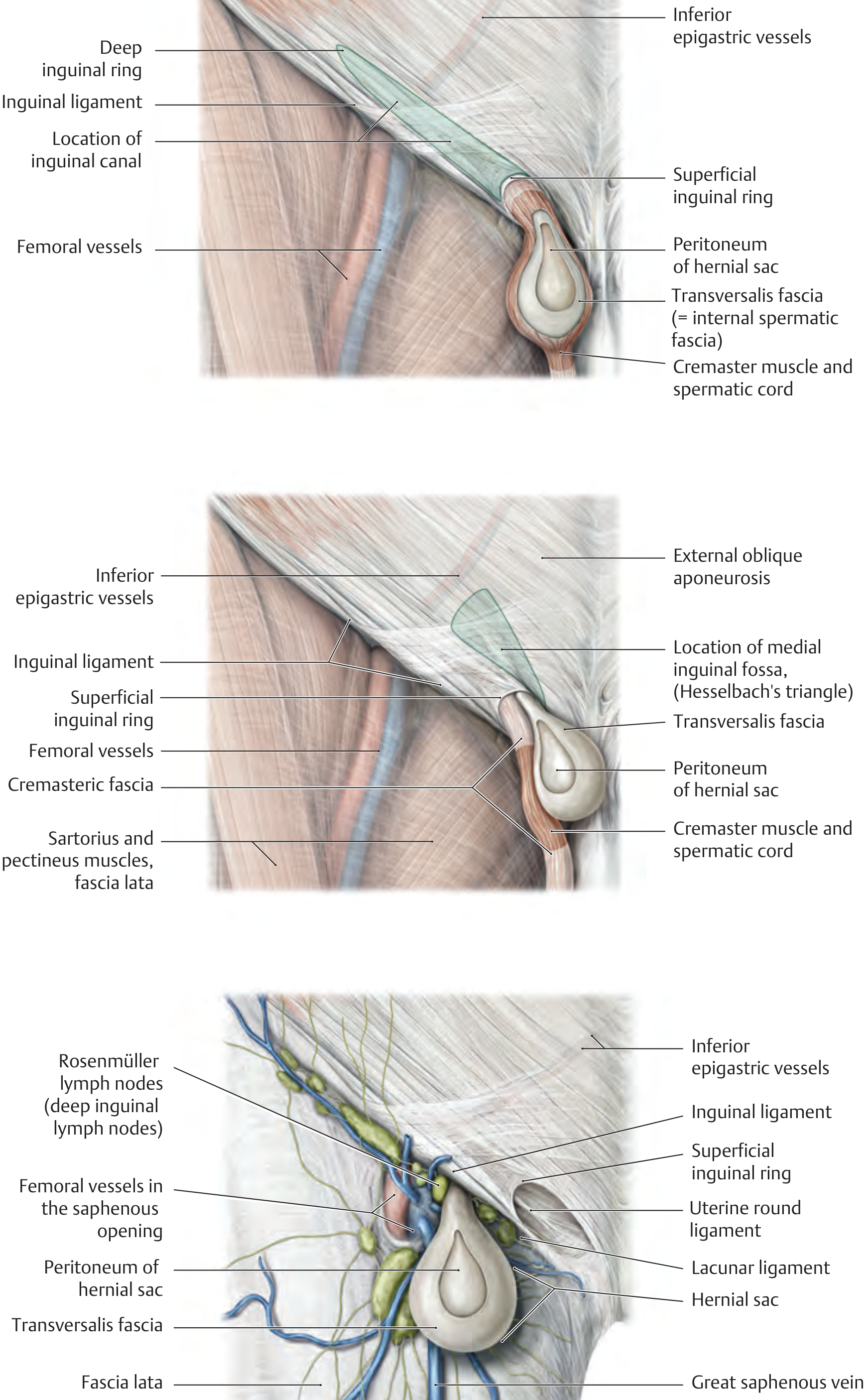
Top: indirect inguinal hernia at deep ring; Middle: direct hernia through Hesselbach's triangle; Bottom: femoral hernia in a female. THIEME Atlas of Anatomy.
10. Diagnosis
Clinical Diagnosis
- History: Groin bulge that appears on standing/coughing, reduces on lying down; aching or dragging discomfort; referred pain to the inner thigh or scrotum
- Inspection: Visible swelling in the groin - increases with Valsalva/coughing
- Deep ring occlusion test: Reduce the hernia, apply finger pressure over the deep ring (midpoint of inguinal ligament). Ask the patient to cough:
- Hernia controlled = indirect (lateral)
- Hernia appears medially despite pressure = direct
Differentiating Direct vs. Indirect Clinically
Even experienced surgeons cannot reliably distinguish these on examination alone. Definitive differentiation is made at operation (or laparoscopy) by the relationship of the sac to the inferior epigastric vessels.
Diagram: Laparoscopic colour-coded defects (yellow=direct, blue=indirect, green=femoral)
(see image in Section 6 above)
Investigations
- Usually not required for straightforward cases
- Ultrasound: First-line imaging for equivocal groin swellings
- CT/MRI: Used when ultrasound is inconclusive, for large or complex hernias, or occult hernias
Differential Diagnosis of a Groin Swelling
| Condition | Key Feature |
|---|---|
| Inguinal hernia | Cough impulse, reducible, above and medial to pubic tubercle |
| Femoral hernia | Below and lateral to pubic tubercle, narrow neck |
| Lymphadenopathy | Multiple, firm nodes, no impulse |
| Hydrocele | Transilluminates, upper limit felt |
| Ectopic / undescended testis | No ipsilateral scrotal testis |
| Saphena varix | Disappears on lying, thrill on coughing, below inguinal ligament |
| Psoas abscess | Fluctuant, below inguinal ligament, may track from spine |
| Lipoma of the cord | Non-reducible, no cough impulse |
11. Classification
European Hernia Society (EHS) Classification
A simplified, practical system:
- P = Primary; R = Recurrent
- L = Lateral (indirect); M = Medial (direct); F = Femoral
- Defect size in fingerbreadths (~1.5 cm each): 1 = ≤1 fb; 2 = 1-3 fb; 3 = ≥3 fb
Example: A primary indirect hernia with a 3 cm defect = PL2
Nyhus Classification (anatomical)
| Type | Description |
|---|---|
| I | Indirect; normal internal ring (pediatric) |
| II | Indirect; enlarged internal ring; posterior wall intact |
| IIIa | Direct; Hesselbach's triangle defect |
| IIIb | Indirect; large sac, incompetent ring, sliding/scrotal |
| IIIc | Femoral |
| IV | Recurrent hernia |
12. Complications
Irreducibility
The hernia contents cannot be returned to the peritoneal cavity. May be due to adhesions within the sac (chronic irreducibility) or sudden entrapment (acute incarceration).
Incarceration (Obstruction)
Bowel within the sac becomes obstructed but blood supply is still intact. Features: tense, tender, irreducible swelling; intestinal obstruction (vomiting, distension, constipation).
Strangulation
Compression of the blood supply at the narrow hernia neck. A surgical emergency. Features: sudden severe pain, irreducible tender swelling, signs of systemic sepsis and bowel ischemia. More common in indirect hernias (narrow neck) and femoral hernias.
13. Management
Non-surgical Management
- Watchful waiting is safe for asymptomatic or minimally symptomatic direct hernias, particularly in elderly patients
- Surgical trusses are not recommended (do not prevent complications, cause skin damage)
Herniotomy (Children Only)
In children with a patent processus vaginalis - simply excise and close the sac at the internal ring. Repair of the floor is not needed as the musculoaponeurotic layers are intact.
14. Open Surgical Repair
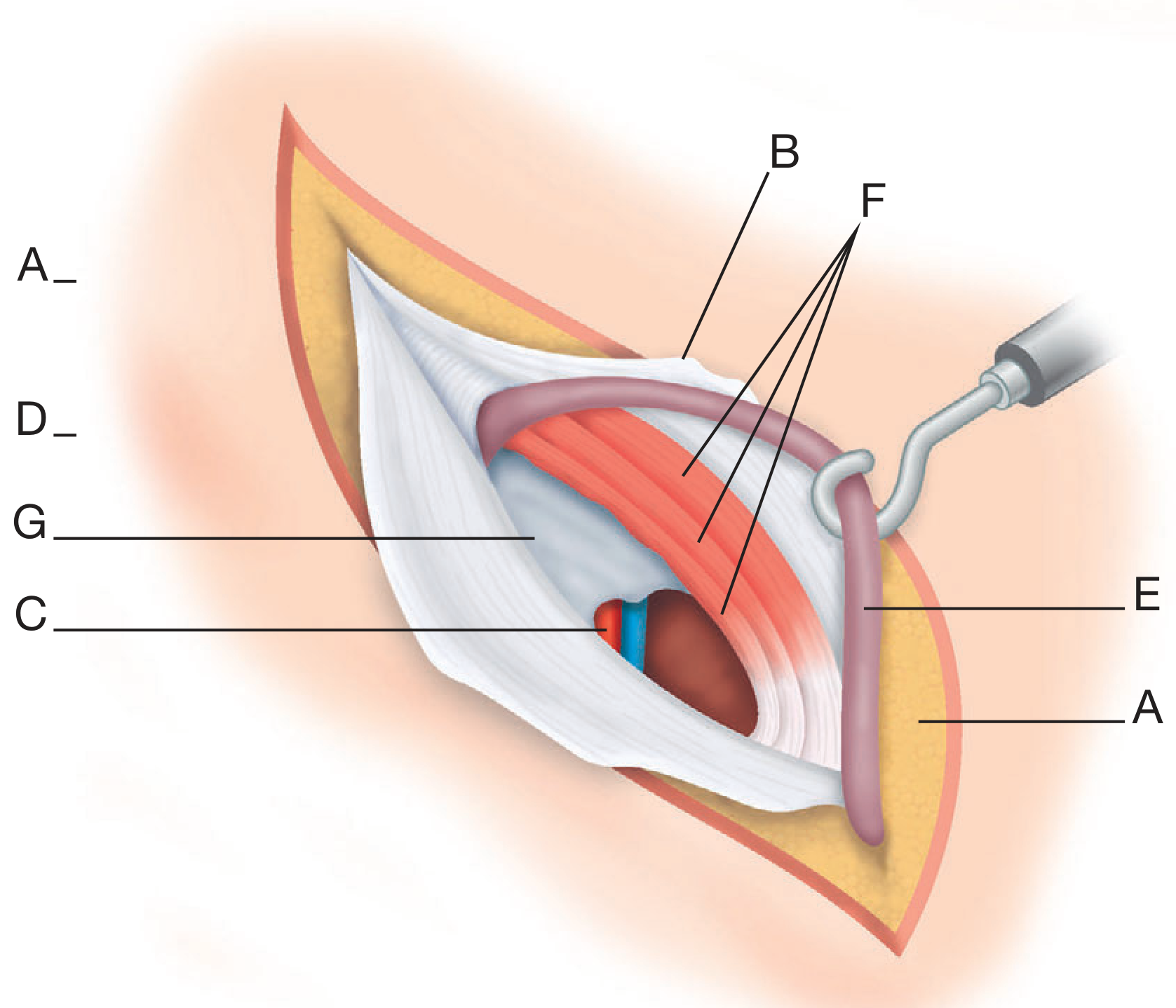
A. Bassini Repair (Historical, 1890)
The inguinal canal is opened. The hernia sac is dealt with. Sutures are placed between the conjoint tendon superiorly and the inguinal ligament inferiorly, from the pubic tubercle to the deep ring. This reconstitutes the posterior wall.
Bassini's original anatomical diagram (1890): A = subcutaneous fat; B = external oblique aponeurosis (opened); C = inferior epigastric vessels; D = Poupart's ligament; E = spermatic cord retracted; F = conjoint tendon; G = transversalis fascia:
B. Shouldice Repair
A more technically demanding suture repair. The transversalis fascia is opened by a central incision from the deep ring to the pubic tubercle and closed in two overlapping layers (double-breasting). The external oblique is closed similarly. Expert centres report lifetime failure rates <2%.
C. Lichtenstein Tension-Free Hernioplasty (Gold Standard Open Repair)
Instead of suturing non-apposing tissue planes under tension, the inguinal floor is reinforced by a flat prosthetic mesh. The mesh (keyhole shaped) is:
- Medial edge overlaps the pubic tubercle by 1.5-2 cm (fixed to anterior rectus sheath)
- Inferior margin fixed to the shelving edge of the inguinal ligament
- Upper edge fixed to the internal oblique
- Lateral tails wrapped around the spermatic cord at the internal ring
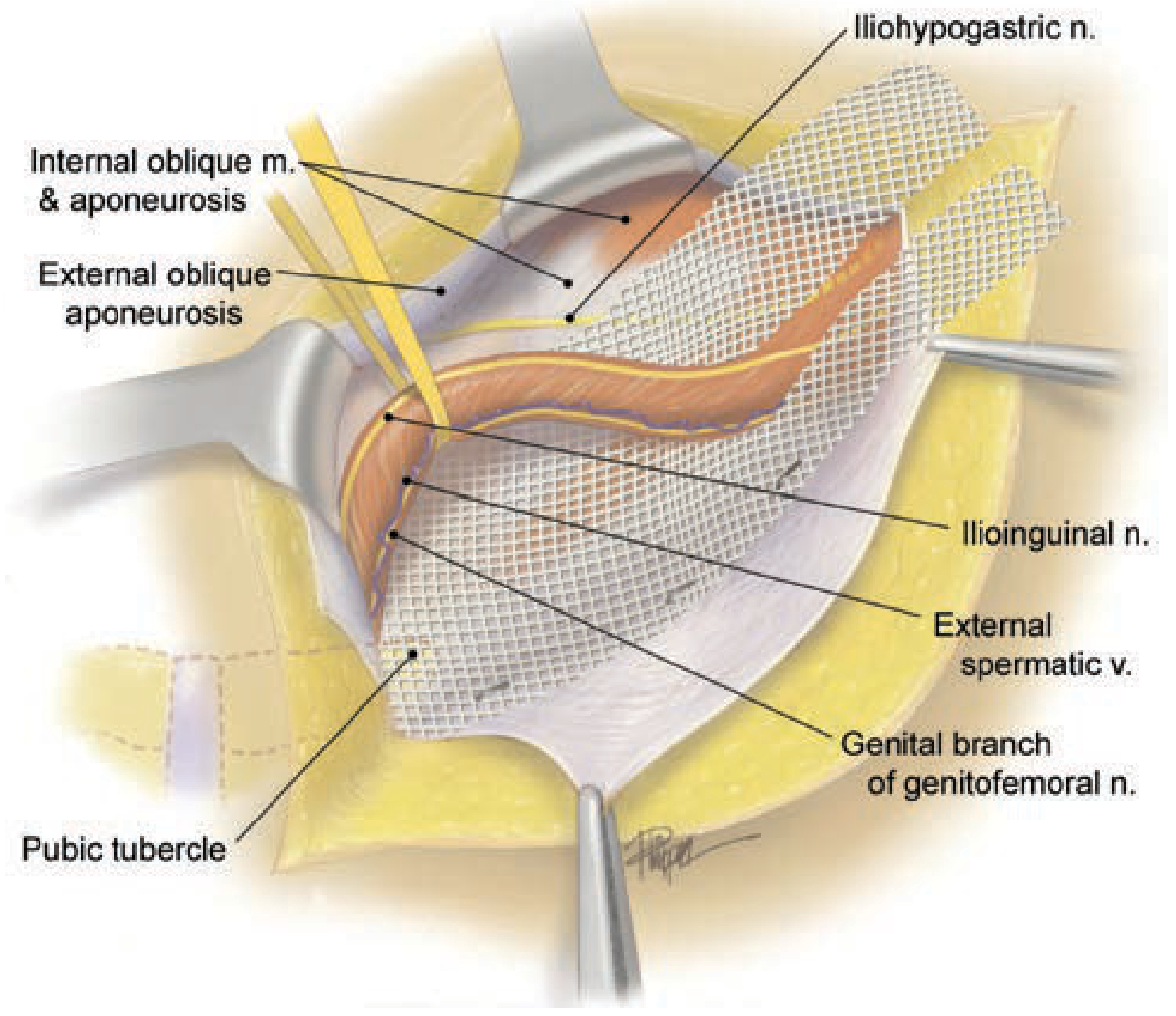
Lichtenstein tension-free hernioplasty with mesh in place. Key nerves must be identified and preserved. Schwartz's Principles of Surgery, 11th ed.
D. Plug-and-Patch (Gilbert/Rutkow-Robbins)
A three-dimensional prosthetic plug is placed into the hernia defect (internal ring for indirect; fixed to Cooper's ligament for direct), followed by a flat mesh patch over the inguinal floor.
15. Laparoscopic / Minimally Invasive Repair
TAPP (Transabdominal Preperitoneal)
- Abdominal cavity is entered first (pneumoperitoneum)
- Peritoneum incised above the hernia defects
- Preperitoneal space dissected to expose the entire myopectineal orifice (MPO)
- Large mesh (≥15×10 cm) placed in the preperitoneal space covering all three hernia spaces (direct, indirect, femoral)
- Peritoneum closed over mesh
TEP (Totally Extraperitoneal)
- The preperitoneal space is accessed directly without entering the peritoneal cavity
- A dissecting balloon creates the preperitoneal working space
- Dissection and mesh placement as for TAPP
- Preferred by many as the peritoneal cavity is not breached
Advantages of Laparoscopic vs. Open
| Factor | Laparoscopic | Open (Lichtenstein) |
|---|---|---|
| Recurrence | Comparable | Comparable |
| Recovery | Faster | Slightly slower |
| Chronic pain | Less | Slightly more |
| Recurrent hernia | Superior | Standard |
| Bilateral hernia | Superior | Two separate incisions |
| Anaesthesia | GA required | Can use LA |
| Learning curve | Steeper | Less steep |
Grade A recommendation (IEHS): TEP or TAPP is preferred over Lichtenstein for recurrent hernias after previous open anterior repair, and for bilateral hernias.
16. Nerves at Risk During Inguinal Hernia Repair
| Nerve | Course | Risk at Operation |
|---|---|---|
| Ilioinguinal nerve | Runs inside canal, outside cord; emerges at superficial ring | Open approach - can be cut or caught in sutures |
| Iliohypogastric nerve | Runs just above inguinal canal | Open approach - can be caught superiorly |
| Genital branch of genitofemoral nerve | Enters canal at deep ring, runs with cord | Both open and laparoscopic |
| Femoral branch of genitofemoral nerve | Lateral to femoral artery | Laparoscopic - "triangle of pain" |
| Lateral femoral cutaneous nerve | Lateral triangle of pain | Laparoscopic - avoid fixation laterally |
The "triangle of doom" (between vas deferens medially and gonadal vessels laterally) contains the external iliac vessels - no staples or tacks must be placed here during laparoscopic repair.
The "triangle of pain" (lateral to the gonadal vessels, inferior to the iliopubic tract) contains the femoral branch of the genitofemoral nerve and the lateral femoral cutaneous nerve - no fixation here.
17. Summary Flowchart
GROIN SWELLING
|
Above inguinal ligament? → YES → INGUINAL HERNIA
|
Medial to IEV? Lateral to IEV?
↓ ↓
DIRECT hernia INDIRECT hernia
(Hesselbach's Δ) (through deep ring)
Always acquired Congenital or acquired
Elderly, broad neck Young, narrow neck
Low strangulation Higher strangulation
risk risk
Sources: Bailey & Love's Short Practice of Surgery 28th ed., Schwartz's Principles of Surgery 11th ed., Fischer's Mastery of Surgery 8th ed., THIEME Atlas of Anatomy (General & Musculoskeletal), Mulholland & Greenfield's Surgery 7th ed.
Inguinal hernia
Asking for Preferences
All
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent - now I have all the additional content needed. Here is the complete, fully illustrated guide building on the previous session:
Inguinal Hernia - Complete Reference (All Topics)
PART 1: EPIDEMIOLOGY & RISK FACTORS
Inguinal hernia is the most common surgical condition worldwide, accounting for ~75% of all abdominal wall hernias. About 27% of men and 3% of women develop a groin hernia at some point in their lifetime.
Risk Factors
Increased intra-abdominal pressure:
- Chronic cough / COPD (strongly linked to direct hernias)
- Constipation / prostatism / bladder outlet obstruction
- Ascites
- Pregnancy
- Heavy lifting / physical exertion
- Valsalva maneuver
Biological / structural:
- Positive family history (8-fold increased lifetime risk)
- Low birthweight (<1500 g)
- Premature birth (patent processus vaginalis)
- Previous right lower quadrant incision (damages ilioinguinal nerve → weakens floor)
- Cigarette smoking (impairs collagen synthesis)
Connective tissue disorders associated with herniation:
- Ehlers-Danlos syndrome
- Marfan syndrome
- Osteogenesis imperfecta
- α1-Antitrypsin deficiency
- Androgen insensitivity syndrome (very high incidence)
Note on obesity: Obesity is actually somewhat protective against inguinal hernia in men (fat fills the space, and obese patients may be under-diagnosed). However it increases post-operative complications.
- Schwartz's Principles of Surgery, 11th ed., p. 1632
PART 2: EMBRYOLOGY & PROCESSUS VAGINALIS
During fetal development, the testes descend from the retroperitoneum to the scrotum guided by the gubernaculum in the third trimester. They drag with them an outpouching of peritoneum - the processus vaginalis - which passes through the inguinal canal. Between 36-40 weeks' gestation, the processus vaginalis should obliterate, sealing the peritoneal communication at the internal ring.
Degrees of Failure to Close
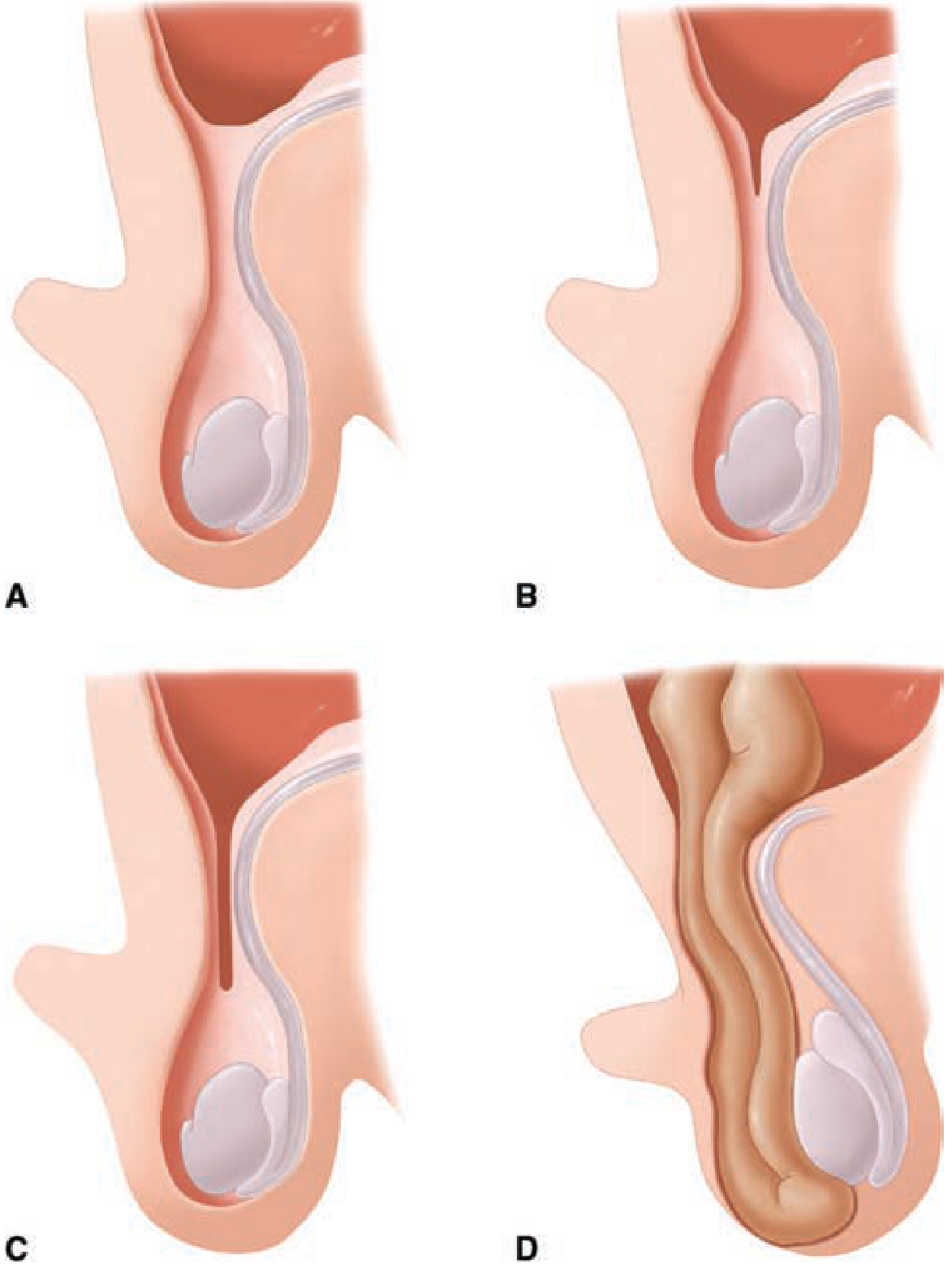
Varying degrees of closure of the processus vaginalis. A = Closed (normal); B = Minimally patent (hydrocele); C = Moderately patent (large hydrocele); D = Fully patent (inguinoscrotal hernia). Schwartz's Principles of Surgery, 11th ed.
| Degree of Patency | Clinical Result |
|---|---|
| Complete obliteration | Normal |
| Minimal patency | Simple hydrocele (fluid-filled, non-communicating) |
| Moderate patency | Communicating hydrocele (enlarges during the day, empties at night) |
| Complete patency | Indirect inguinal hernia ± inguinoscrotal hernia |
PART 3: ANATOMY OF THE INGUINAL CANAL (DETAILED)
Layers of the Abdominal Wall at the Groin (Outside → In)
- Skin
- Scarpa's fascia (deep layer of superficial fascia)
- External oblique muscle and aponeurosis
- Internal oblique muscle
- Transversus abdominis muscle
- Transversalis fascia
- Preperitoneal fat (Space of Bogros laterally; Space of Retzius medially)
- Parietal peritoneum
Walls of the Inguinal Canal
| Wall | Structure |
|---|---|
| Anterior | External oblique aponeurosis (whole length) + Internal oblique muscle (lateral 1/3) |
| Posterior | Transversalis fascia (whole length) + Conjoint tendon (medial 1/3) |
| Roof (superior) | Arching fibers of internal oblique + Transversus abdominis |
| Floor (inferior) | Inguinal ligament (Poupart's) + Lacunar ligament medially |
Inguinal Canal Contents
Male: Spermatic cord (vas deferens, testicular artery, pampiniform venous plexus, cremasteric artery/vein, artery to vas, lymphatics, autonomic nerves, genital branch of genitofemoral nerve, cremasteric muscle) + ilioinguinal nerve (outside cord)
Female: Round ligament of uterus + ilioinguinal nerve
PART 4: HESSELBACH'S TRIANGLE (INGUINAL TRIANGLE)
The boundaries define the location of direct inguinal hernias:
| Border | Structure |
|---|---|
| Medial | Lateral border of rectus abdominis |
| Superolateral | Inferior epigastric vessels |
| Inferior | Inguinal ligament (iliopubic tract) |
The triangle is weak because no muscle reinforcement exists here - only transversalis fascia covered by external oblique aponeurosis.
PART 5: TYPES OF INGUINAL HERNIA
The Key Landmark: Inferior Epigastric Vessels
The inferior epigastric artery and vein arise from the external iliac vessels just above the inguinal ligament and run superomedially to enter the posterior rectus sheath. Their position lateral to the deep inguinal ring is the single most important anatomical landmark:
- Hernia lateral to them = indirect
- Hernia medial to them = direct
Internal Hernia Openings (Posterior View)
| Hernia Type | Internal Opening | External Opening |
|---|---|---|
| Direct inguinal | Medial inguinal fossa (Hesselbach's triangle) | Superficial inguinal ring |
| Indirect inguinal | Lateral inguinal fossa (deep inguinal ring) | Superficial inguinal ring |
| Supravesical | Supravesical fossa | Superficial inguinal ring |
| Femoral | Femoral ring (below inguinal ligament) | Saphenous opening |
- THIEME Atlas of Anatomy
PART 6: NERVES OF THE INGUINAL REGION
Sensory Dermatomes - Why Nerve Injury Matters Clinically
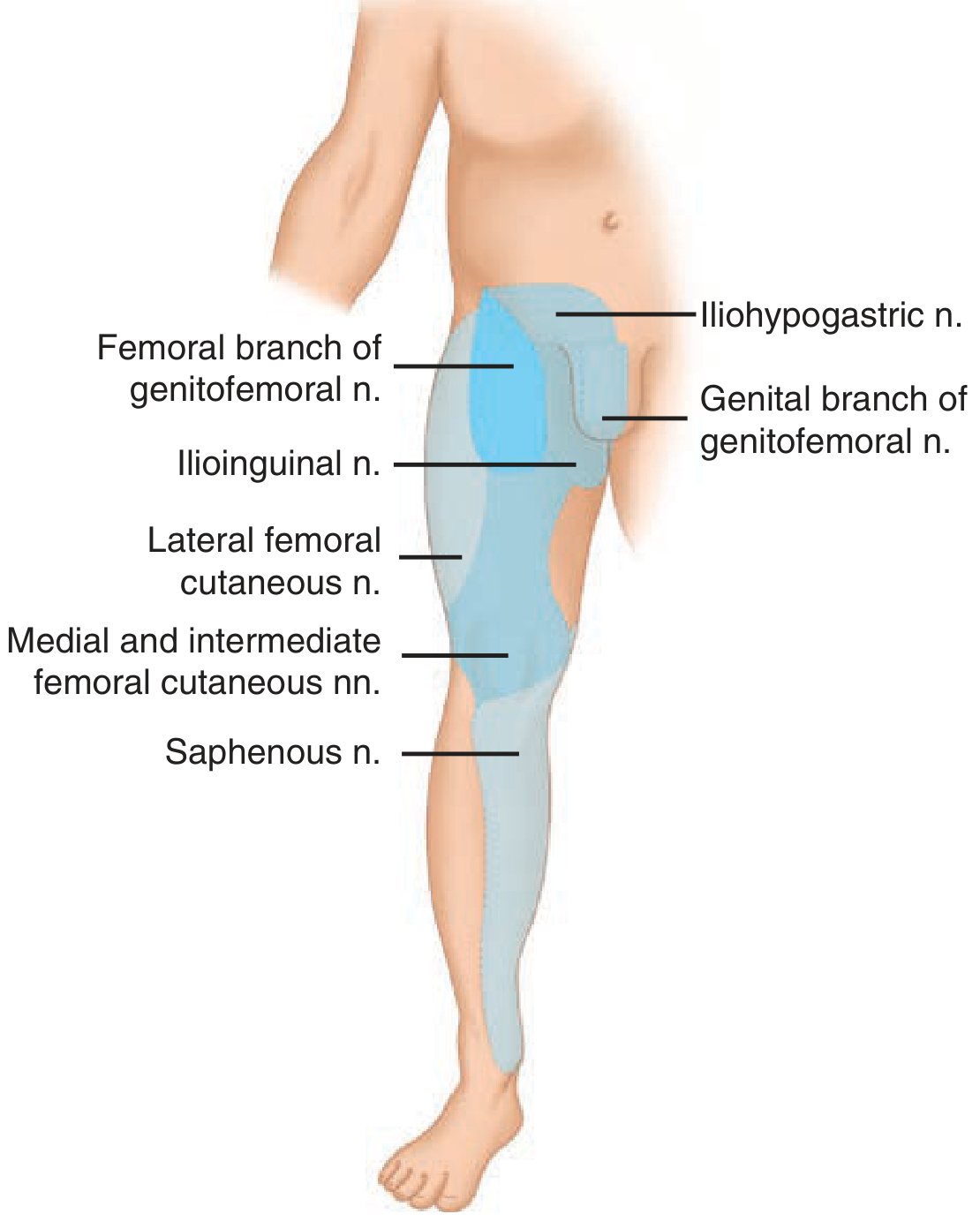
Sensory dermatomes of the major nerves in the groin - critical for understanding hernia repair complications. Schwartz's Principles of Surgery, 11th ed.
Five Key Nerves
| Nerve | Origin | Course | Sensory Distribution | Risk |
|---|---|---|---|---|
| Iliohypogastric | T12-L1 | Pierces transversus abdominis; runs ~2-3 cm above deep ring | Suprapubic skin | Open repair (sutures superiorly) |
| Ilioinguinal | L1 | Runs in canal on anterior surface of cord | Upper medial thigh, scrotum/labia | Open repair |
| Genital branch of GFN | L1-L2 | Enters deep ring with cord; runs with cord | Scrotum/labia majora + cremaster | Open and laparoscopic |
| Femoral branch of GFN | L1-L2 | Passes under inguinal ligament lateral to femoral artery | Upper anterior thigh | Laparoscopic (Triangle of Pain) |
| Lateral femoral cutaneous n. | L2-L3 | Passes near ASIS under inguinal ligament | Lateral thigh | Laparoscopic (Triangle of Pain) |
Triangle of Doom and Triangle of Pain
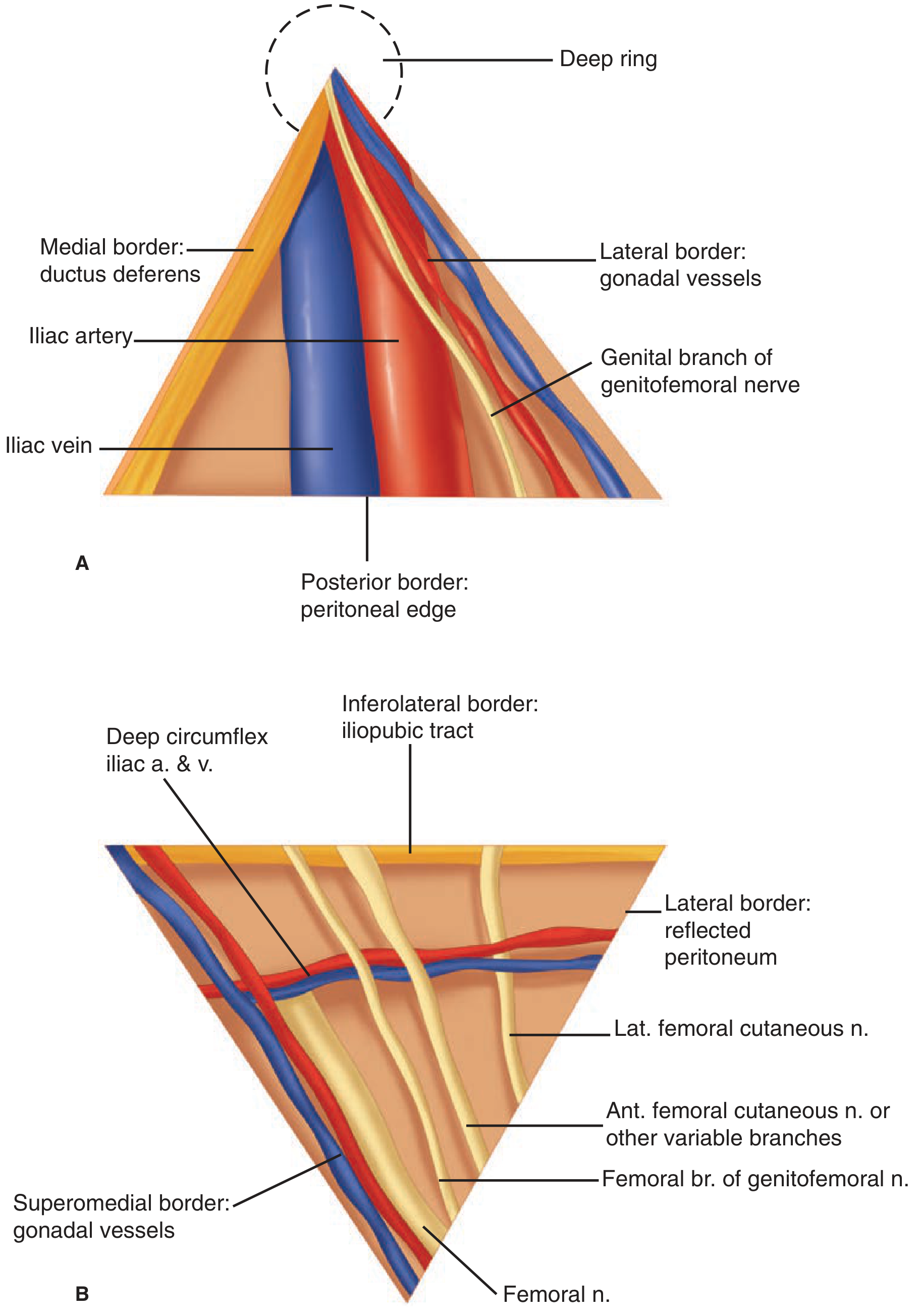
Triangle of Doom (A) contains the external iliac vessels - NEVER place tacks/staples here. Triangle of Pain (B) contains sensory nerves - NEVER place fixation here. Schwartz's Principles of Surgery, 11th ed.
Triangle of Doom:
- Medial border: Vas deferens
- Lateral border: Gonadal vessels
- Apex: Deep inguinal ring
- Contains: External iliac artery and vein
- Risk: Catastrophic vascular injury if tacked during laparoscopic repair
Triangle of Pain:
- Superior border: Iliopubic tract
- Lateral border: Reflected peritoneum
- Superomedial: Gonadal vessels
- Contains: Femoral branch of GFN, lateral femoral cutaneous nerve, femoral nerve
- Risk: Nerve entrapment causing chronic neuropathic pain if tacked
PART 7: PEDIATRIC INGUINAL HERNIA
Key Differences from Adults
| Feature | Pediatric | Adult |
|---|---|---|
| Type | Always indirect (congenital PPV) | Direct, indirect, or femoral |
| Cause | Patent processus vaginalis | Wall weakness / increased IAP |
| Surgery | Herniotomy (sac ligation only; no floor repair) | Hernioplasty (floor repair needed) |
| Urgency | All require repair (indication for surgery = presence of hernia) | Asymptomatic direct = watchful waiting acceptable |
| Incarceration risk | High (narrow ring in infants) | Lower |
| Contralateral risk | High - explore contralateral side (especially <2 years) | ~50% lifetime risk |
Incarceration in Children
- Features: Firm, tense, non-reducible groin mass; irritability in infants; intestinal obstruction signs if bowel involved
- Management:
- Attempt gentle reduction (from below, toward internal ring) - may need light sedation
- If reduced: admit for observation, operate within 24h
- If cannot be reduced or strangulation suspected: emergency operation
- Strangulation: edematous, tender, erythematous swelling → emergency op with possible bowel resection
Bilateral Exploration in Children
- Incidence of bilateral PPV is ~60% at birth but falls with age
- Laparoscopic evaluation of the contralateral side through the hernia sac is now standard in many centers
PART 8: CLINICAL FEATURES & EXAMINATION
Symptoms
- Groin bulge - appears on standing, coughing, straining; disappears on lying (reducible)
- Dragging ache in the groin / lower abdomen, worse during the day with activity
- Referred pain to inner thigh, scrotum, or labia (ilioinguinal nerve)
- Sudden onset of severe pain = complication (incarceration/strangulation)
Examination Sequence
1. Inspect with patient standing, then coughing - look for visible bulge above and medial to the pubic tubercle.
2. Palpate the inguinal region - identify ASIS and pubic tubercle to locate the deep inguinal ring (midpoint of inguinal ligament).
3. Deep ring occlusion test (ZIeveri's sign approach):
- Reduce the hernia manually
- Apply firm pressure with finger over the deep inguinal ring (1 cm above midpoint of inguinal ligament)
- Ask patient to cough:
- Controlled by pressure = Indirect (lateral) hernia
- Not controlled, appears medially = Direct (medial) hernia
4. Scrotal/labial examination: Invaginate scrotal skin with the fingertip into the inguinal canal, feel for impulse on coughing. In males: always examine contralateral side, examine testes.
5. Assess for complications: Is the swelling reducible? Tender? Any bowel sounds in the swelling?
Important Clinical Signs
| Feature | Indirect | Direct |
|---|---|---|
| Side | Right > Left (3:1) | Both equally common |
| Deep ring control | Controls hernia | Does NOT control hernia |
| Descends to scrotum | Yes | Rarely |
| Neck | Narrow (strangulation risk) | Wide, broad-based |
| Associated with cord | Hernia IS within cord | Adjacent to cord |
PART 9: INVESTIGATIONS
| Investigation | Indication |
|---|---|
| Ultrasound | First-line for equivocal groin swelling; can demonstrate hernia with dynamic Valsalva maneuver |
| CT scan | Large or complex hernias; suspected internal hernias; ruling out other pelvic pathology |
| MRI | Occult hernias; chronic groin pain (can show osteitis pubis, muscle tears, bursitis) |
| Herniography (contrast into peritoneum) | Rarely used; for occult hernias when other tests inconclusive |
Note: Hernias frequently reduce spontaneously in the supine position (during scanning) - always request dynamic assessment.
PART 10: COMPLICATIONS
1. Irreducibility
Contents cannot be returned to the peritoneal cavity, usually due to adhesions from previous inflammation. The hernia is non-tender and soft (unlike incarceration).
2. Incarceration (Obstruction)
Acute trapping of bowel within the hernia. Blood supply initially intact. Features:
- Sudden onset of pain in a previously painless hernia
- Tense, tender, irreducible swelling
- Signs of intestinal obstruction (vomiting, distension, absolute constipation)
Management: Attempt manual reduction (taxis), then early surgery.
3. Strangulation
Constriction of blood supply at the narrow hernia neck → ischemia → gangrene. A surgical emergency.
Features:
- Severe constant pain (not just colicky)
- Hard, tender, irreducible swelling, overlying skin may be red
- Systemic signs: fever, tachycardia, peritonism
- No bowel sounds may be audible in the hernia
Risk factors for strangulation:
- Narrow neck (indirect > direct; femoral > inguinal)
- Long-standing irreducible hernia
- Elderly female (femoral hernia risk is highest)
Surgical management:
- Emergency operation
- Assess bowel viability: warm pad for 5 minutes, check peristalsis, color, Doppler flow
- Viable bowel: reduce
- Non-viable bowel: resection + anastomosis (or Hartmann's for grossly contaminated field)
- Hernia repair: Mesh placement remains acceptable in clean-contaminated fields (no gross enteric spillage); primary tissue repair for contaminated/dirty fields
4. Richter's Hernia
Only the antimesenteric wall of bowel is caught - so obstruction may be absent even with strangulation. Small femoral or indirect hernias. Easy to miss clinically.
5. Maydl's Hernia (W-hernia)
Two adjacent loops of bowel are in the sac, forming a "W" shape, with the middle loop (the interconnecting segment) strangulating inside the peritoneal cavity. The sac contents may appear viable at operation while the intraperitoneal loop is gangrenous - must inspect the entire bowel loop including that inside the abdomen.
PART 11: SURGICAL REPAIR - ALL TECHNIQUES
Decision Framework
Inguinal hernia confirmed
|
┌─────┴─────┐
Elective Emergency
(reducible) (incarcerated/strangulated)
|
┌──────┴──────┐
Adult Child
| |
Mesh Herniotomy
repair (sac ligation only)
|
┌────────────────────┐
Open Laparoscopic
(Lichtenstein) (TEP or TAPP)
↓ ↓
Local/spinal/GA GA required
↓ ↓
Single hernia Bilateral / recurrent
No prior surgery Previous open repair
OPEN REPAIRS
A. Herniotomy (Pediatric Only)
Excision and ligation of the hernia sac at the deep inguinal ring. No floor repair. Recurrence rate is very low because the musculoaponeurotic layers are intact.
B. Bassini Repair (1890)
- Open external oblique aponeurosis
- Mobilize spermatic cord
- Excise/reduce hernia sac
- Suture conjoint tendon to inguinal ligament from pubic tubercle to deep ring
- Reconstitutes the posterior wall under tension
- High recurrence rate (~15% in most centers)
C. Shouldice Repair
- Superior results to Bassini (recurrence <2% at expert centers, but ~10% in general practice)
- Open and double-breast the transversalis fascia (two layers)
- Repair external oblique in two layers
- Technically demanding - preferred at specialized hernia centers
D. McVay (Cooper's Ligament) Repair
- Suture transversalis fascia/conjoint tendon to Cooper's ligament (pectineal ligament)
- Useful for femoral hernias (unlike Bassini)
- A relaxing incision in the anterior rectus sheath is needed to relieve tension
E. Lichtenstein Tension-Free Hernioplasty (Current Gold Standard Open)
Mesh placed on the inguinal floor without tissue tension.
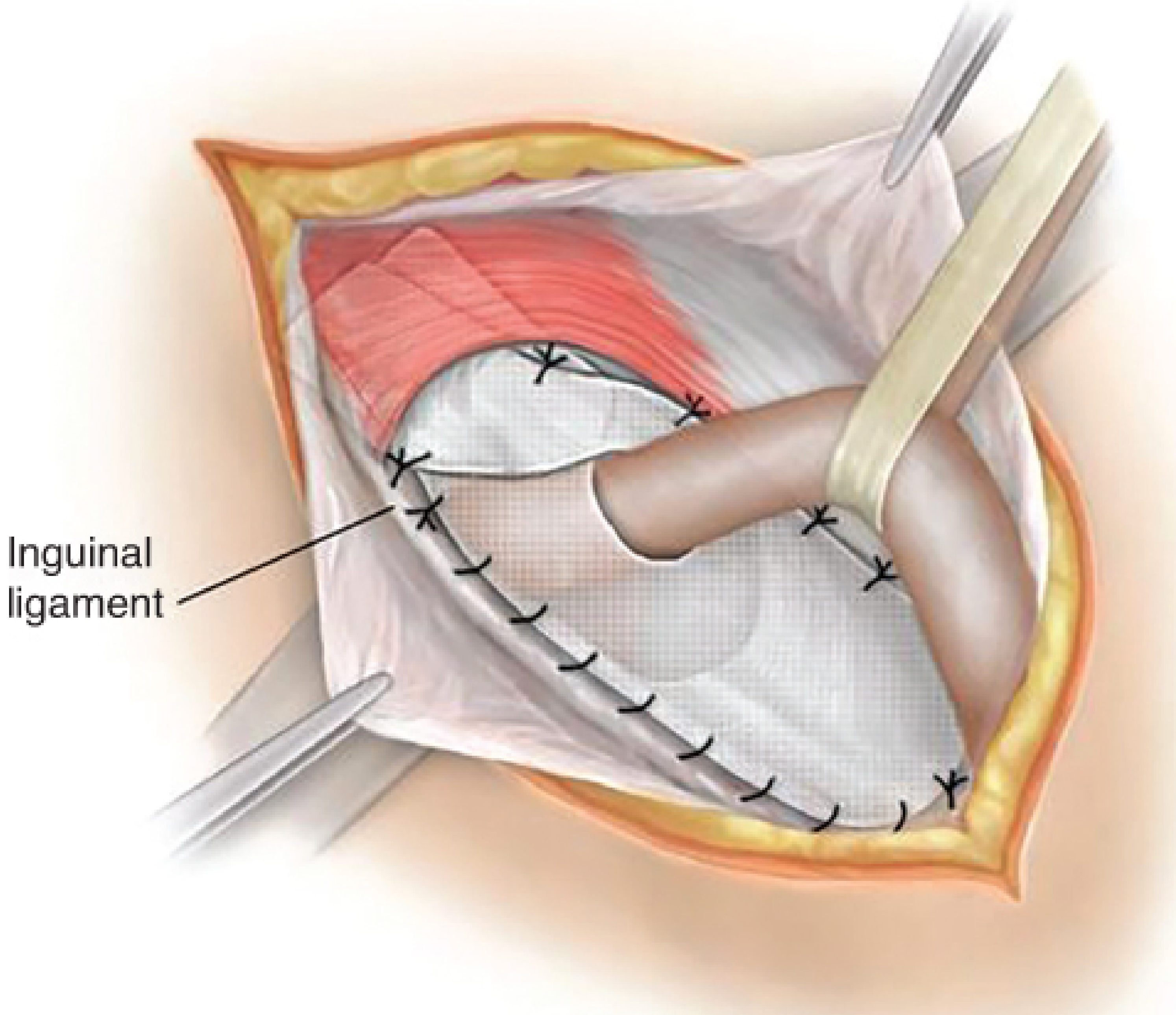
Lichtenstein repair - mesh sutured to the inguinal ligament inferiorly and conjoint tendon/internal oblique superiorly. Fischer's Mastery of Surgery, 8th ed.
Key steps:
- Incise skin from pubic tubercle to just lateral to deep ring
- Open external oblique aponeurosis; identify ilioinguinal nerve
- Mobilize spermatic cord
- Deal with hernia sac (excise/reduce indirect; invert direct)
- Place flat mesh (keyhole for spermatic cord):
- Medial: overlap pubic tubercle by 1.5-2 cm, fix to anterior rectus sheath
- Inferior: fix to shelving edge of inguinal ligament
- Superior: fix to internal oblique
- Lateral tails: wrap snugly around cord at deep ring (not tight)
- Close external oblique aponeurosis over mesh
Mesh sizing: Must extend at least 2-3 cm superior to Hesselbach's triangle. The mesh prevents direct, indirect, and (with inferior extension) femoral hernias.
LAPAROSCOPIC REPAIRS
F. TAPP (Transabdominal Preperitoneal)
- Pneumoperitoneum, 3 ports (umbilical 10 mm + 2×5 mm lateral)
- Patient in Trendelenburg
- Incise peritoneum above the hernia defects (medial umbilical ligament to ASIS)
- Develop preperitoneal space - expose Cooper's ligament, pubic symphysis, deep ring
- Reduce hernia sac from cord (parietalize cord)
- Achieve Critical View of MPO (direct, indirect, femoral spaces all visualized)
- Place mesh ≥15×10 cm covering entire MPO
- Close peritoneum over mesh with tacks or suture
Advantage: Intraperitoneal view useful for bilateral hernias and ambiguous groin pathology. Can assess bowel viability if spontaneous reduction of incarcerated hernia occurs.
G. TEP (Totally Extraperitoneal)
- Small infraumbilical incision to preperitoneal space (anterior rectus sheath opened, retracted)
- Balloon dissector (or digital/blunt dissection) creates working space in preperitoneal plane
- CO₂ insufflation of preperitoneal space (not peritoneal cavity)
- Identical dissection and mesh placement as TAPP
- Peritoneal cavity is never entered
Advantages over TAPP: No peritoneal closure needed; lower risk of port-site hernias and intraperitoneal adhesions; easier port placement.
Disadvantage: If peritoneum tears, conversion to TAPP or open is required. Steeper learning curve.
Mesh Placement in Laparoscopic Repair
Mesh must cover the entire myopectineal orifice (MPO) with adequate overlap:
- Medial: pubic symphysis (contralateral Cooper's ligament for large direct hernias)
- Superior: 3-4 cm above deep ring
- Inferior: 1-2 cm below pubis into Space of Retzius
- Lateral: against psoas muscle
- Minimum size: 15 × 10 cm (14 × 11 cm also acceptable)
- Never split the mesh around the cord
Fixation in Laparoscopic Repair
- Mesh fixation is not mandatory in the preperitoneal space for small to moderate hernias
- When used, fixation should be confined to safe zones (above iliopubic tract medially; avoid triangles of doom and pain)
- Absorbable tacks preferred over permanent to reduce chronic pain risk
PART 12: POSTOPERATIVE COMPLICATIONS
Early Complications
| Complication | Details |
|---|---|
| Wound infection | ~1-2%; higher with emergency repair |
| Seroma | Fluid accumulation in hernia sac remnant; usually resolves spontaneously |
| Hematoma | Especially if anticoagulated; compressive dressings, rarely requires drainage |
| Urinary retention | Especially in elderly males with BPH; catheterize |
| Orchitis / testicular atrophy | Damage to testicular vessels during dissection of large/inguinoscrotal sacs |
| Vas deferens injury | 0.3-0.5% of open repairs; leads to subfertility if bilateral |
Late Complications
1. Recurrence
- Open mesh (Lichtenstein): ~1-5% at 5 years in experienced hands
- Laparoscopic (TEP/TAPP): ~1-4% at 5 years
- Causes: missed hernia defect (especially femoral), inadequate mesh overlap, mesh migration, technical error
For recurrent hernia after open anterior repair: laparoscopic approach is strongly preferred (different tissue planes, avoids scarred anterior field) - Grade A recommendation (IEHS).
2. Chronic Postoperative Inguinal Pain (CPIP)
The most significant long-term complication of modern hernia repair.
- Defined as pain persisting >3-6 months after surgery
- Incidence: up to 15% have some CPIP; ~10% have moderate-severe pain
- Only 1-3% seek medical attention for it
- Two types:
- Neuropathic: Direct nerve injury (cut, crushed, stretched, caught in suture/tack), neuroma formation, mesh pressing on nerve
- Mechanical (somatic): Mesh mass effect (especially plugs), musculoskeletal restriction, tension from tissue repairs
- Management:
- NSAIDs + reassurance (most resolve spontaneously)
- Nerve blocks (diagnostic + therapeutic)
- If severe and immediate (recovery room): re-explore before scarring
- Triple neurectomy (ilioinguinal, iliohypogastric, genital branch GFN) + neuroma excision + adhesiolysis + foreign body removal if required
- Best managed at multidisciplinary pain centers
Risk factors for CPIP:
- Preoperative pain at surgical site
- Open > laparoscopic repair
- Female sex
- Younger age
- High acute postoperative pain
- Psychological factors
PART 13: SPECIAL SITUATIONS
Bilateral Inguinal Hernia
- Lifetime risk of contralateral hernia after unilateral repair is ~50%
- Laparoscopic repair is preferred for simultaneous bilateral repair (single anesthetic, both sides through same ports)
- Open bilateral repair requires two separate groin incisions
Inguinal Hernia in Women
- Much less common (M:F = 10:1), but femoral hernias are proportionally more common in women
- Always check for a femoral hernia component in women
- Laparoscopic view best distinguishes inguinal from femoral hernias
- Round ligament is in the sac (not cord structures); can be divided at operation
- Ovary or fallopian tube can be the hernia contents
Hernia in Pregnancy
- Open tension-free repair under local anesthesia can be safely performed
- Timing: ideally second trimester if repair is needed electively
- Laparoscopic repair is generally avoided in pregnancy
Recurrent Inguinal Hernia
- After previous anterior open repair: use laparoscopic (TEP or TAPP) - Grade A
- After previous laparoscopic repair: use open anterior (Lichtenstein)
- The principle: always approach from the virgin tissue plane
Hernia with Contamination (Emergency with Strangulation)
- Bowel resection is not an absolute contraindication to mesh
- Synthetic mesh acceptable in clean-contaminated fields (no gross spillage)
- Use primary tissue repair (McVay or Bassini) in grossly contaminated/dirty fields
- Biologic meshes (acellular dermal matrix) can be used when primary repair is not feasible in contaminated fields
PART 14: SUMMARY TABLE - DIRECT vs. INDIRECT vs. FEMORAL
| Feature | Indirect | Direct | Femoral |
|---|---|---|---|
| Location | Lateral to IEV | Medial to IEV | Below inguinal ligament |
| Opening | Deep inguinal ring | Hesselbach's triangle | Femoral ring |
| Exit | Superficial inguinal ring | Superficial inguinal ring | Saphenous opening |
| Relation to pubic tubercle | Above and lateral | Above and medial | Below and lateral |
| Age | Any (neonates to adults) | Middle-aged/elderly | Middle-aged women |
| Sex | M >> F | M >> F | F > M (but still uncommon in F) |
| Cause | Congenital or acquired | Always acquired | Always acquired |
| Strangulation risk | Moderate | Low | Highest |
| Descends to scrotum | Yes | No | No |
| Deep ring occlusion | Controls hernia | Does NOT control | Does NOT control |
Sources: Schwartz's Principles of Surgery 11th ed.; Bailey & Love's Short Practice of Surgery 28th ed.; Fischer's Mastery of Surgery 8th ed.; Mulholland & Greenfield's Surgery 7th ed.; Sabiston Textbook of Surgery; THIEME Atlas of Anatomy; Campbell-Walsh Urology.
This is a shared conversation. Sign in to Orris to start your own chat.