The images and content are already in context from the previous searches. Let me compile everything into the full, detailed notes with images embedded inline right now.
CORNEA — DETAILED ANATOMY & PHYSIOLOGY
With Textbook Images | Ophthalmology Resident Level
Sources: Kanski's Clinical Ophthalmology 10th Ed. | Robbins & Kumar Pathologic Basis of Disease | Wheater's Functional Histology | Gray's Anatomy for Students | Krachmer/Mannis/Holland: Cornea
SECTION 1: OVERVIEW
The cornea is a transparent, avascular, densely innervated refractive structure forming the anterior 1/6 of the outer fibrous coat of the eye. It has two fundamental roles:
- Optical - provides ~+43 D of the total ~60 D refractive power of the eye (two-thirds of total)
- Protective - physical and biological barrier between the external environment and the eye
"The cornea is a complex structure which, as well as having a protective role, is responsible for about three-quarters of the optical power of the eye. The normal hydration level is 78%." — Kanski 10th Ed., p. 220
Key Numbers
| Parameter | Value |
|---|
| Horizontal diameter | 12 mm |
| Vertical diameter | 11.5 mm |
| Central thickness (CCT) | ~540 µm (range 490-560 µm) |
| Peripheral thickness | ~700 µm |
| Anterior radius of curvature | ~7.8 mm |
| Posterior radius of curvature | ~6.5 mm |
| Normal hydration | 78% |
| Refractive index (stroma) | 1.376 |
| Refractive power (net) | ~+43 D |
| Endothelial cell density (young adult) | ~2,500-3,000 cells/mm² |
| Critical endothelial density | ~500 cells/mm² |
CCT is a key determinant of IOP measured by Goldmann applanation tonometry. Thin corneas give falsely LOW readings; thick corneas give falsely HIGH readings.
SECTION 2: EMBRYOLOGY
Cell Origins
| Corneal Layer | Embryological Origin |
|---|
| Epithelium | Surface ectoderm overlying the optic cup |
| Bowman layer | Condensation of anterior stroma (fetal keratocytes) |
| Stroma | Neural crest mesenchyme (two migration waves) |
| Keratocytes | Neural crest cells that differentiate in situ |
| Descemet membrane | Neural crest endothelium (ABZ secreted in utero) |
| Endothelium | Second wave of neural crest cells |
Developmental Timeline
- 5-6 weeks: Surface ectoderm separates from lens vesicle → 2-layer primitive corneal epithelium
- 7 weeks: First wave of neural crest → primitive endothelium
- 8 weeks: Second wave of neural crest → keratoblasts; stroma layering begins
- 3rd-5th month: Collagen lamellae organize; proteoglycans accumulate; cornea becomes transparent
- Birth: Corneal diameter ~10 mm; adult size reached by ~2 years of age
Key Developmental Anomalies
| Anomaly | Defect | Features |
|---|
| Peters anomaly | Failure of lens vesicle separation from surface ectoderm | Central corneal opacity; Descemet/endothelial defect; possible lenticulocorneal adhesion; PAX6, PITX2, CYP1B1 mutations |
| Sclerocornea | Failure of corneal differentiation from sclera | Vascularized, opaque cornea; glaucoma association |
| CHED | SLC4A11 mutation; endothelial dysfunction from birth | Diffuse ground-glass oedema; nystagmus; painless |
| Megalocornea | Excessive growth; CHRDL1 gene; X-linked | Diameter >12 mm; normal IOP; distinguish from congenital glaucoma |
| Microcornea | Insufficient anterior segment expansion | Diameter <10 mm; high hyperopia risk |
SECTION 3: GROSS ANATOMY AND SHAPE
The cornea is an oblate ellipsoid - not a perfect sphere:
- Steeper centrally (~48 D at center / 7.8 mm radius of curvature)
- Progressively flatter toward the periphery (~41-42 D / 8.6-9.0 mm radius)
- This progressive flattening = prolate asphericity (Q value ≈ -0.26)
- Prolate shape minimizes spherical aberration by ensuring peripheral and central rays converge at near-identical focal points
Corneal Zones
| Zone | Approx. Diameter | Relevance |
|---|
| Central optical zone | 3-4 mm | Highest refractive power; primary target for refractive surgery |
| Paracentral zone | 4-7 mm | Transition zone |
| Peripheral zone | 7-10 mm | Flatter; site of early degeneration changes |
| Limbus | ~1.5-2 mm wide | Junction with sclera/conjunctiva; LSC niche; vascular arcades |
The Limbus
- Transition zone between transparent cornea and opaque sclera
- Contains trabecular meshwork and Schlemm's canal internally (angle structures)
- Palisades of Vogt: radially oriented fibrovascular ridges at superior and inferior limbus — structural home of limbal stem cells
- Contains limbal crypts and limbal epithelial crypts (LECs) housing LSCs in their niche
- The corneoscleral envelope provides the structural rigidity of the globe
SECTION 4: THE SIX LAYERS — DETAILED
ANTERIOR SURFACE (tear film)
│
├── 1. Epithelium 50-60 µm
├── 2. Bowman Layer 8-12 µm
├── 3. Stroma 450-500 µm ← 90% of total
├── 4. Dua's Layer 10-15 µm
├── 5. Descemet Membrane 10-12 µm
└── 6. Endothelium ~5 µm (single cell layer)
│
POSTERIOR SURFACE (anterior chamber / aqueous)
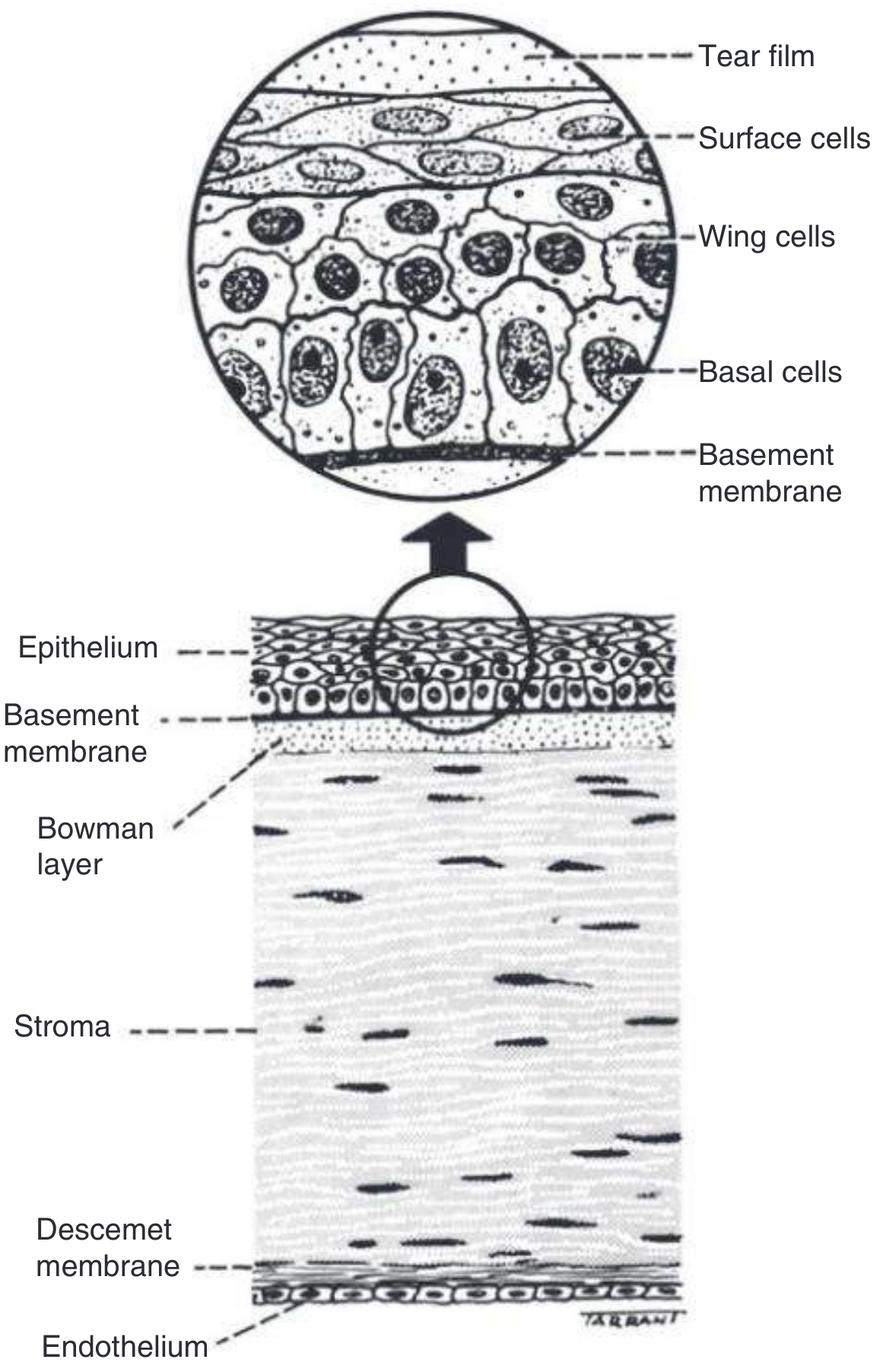
IMAGE 1 — Corneal Layer Diagram
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.1
Reading this diagram: Bottom to top: endothelium (flat monolayer) → Descemet membrane → stroma (wavy horizontal lamellae with flat keratocyte nuclei between) → Bowman layer → epithelial basement membrane → basal cells (columnar, large oval nuclei) → wing cells (polygonal with lateral processes) → surface squamous cells (flat, small nuclei) → tear film at the apex.
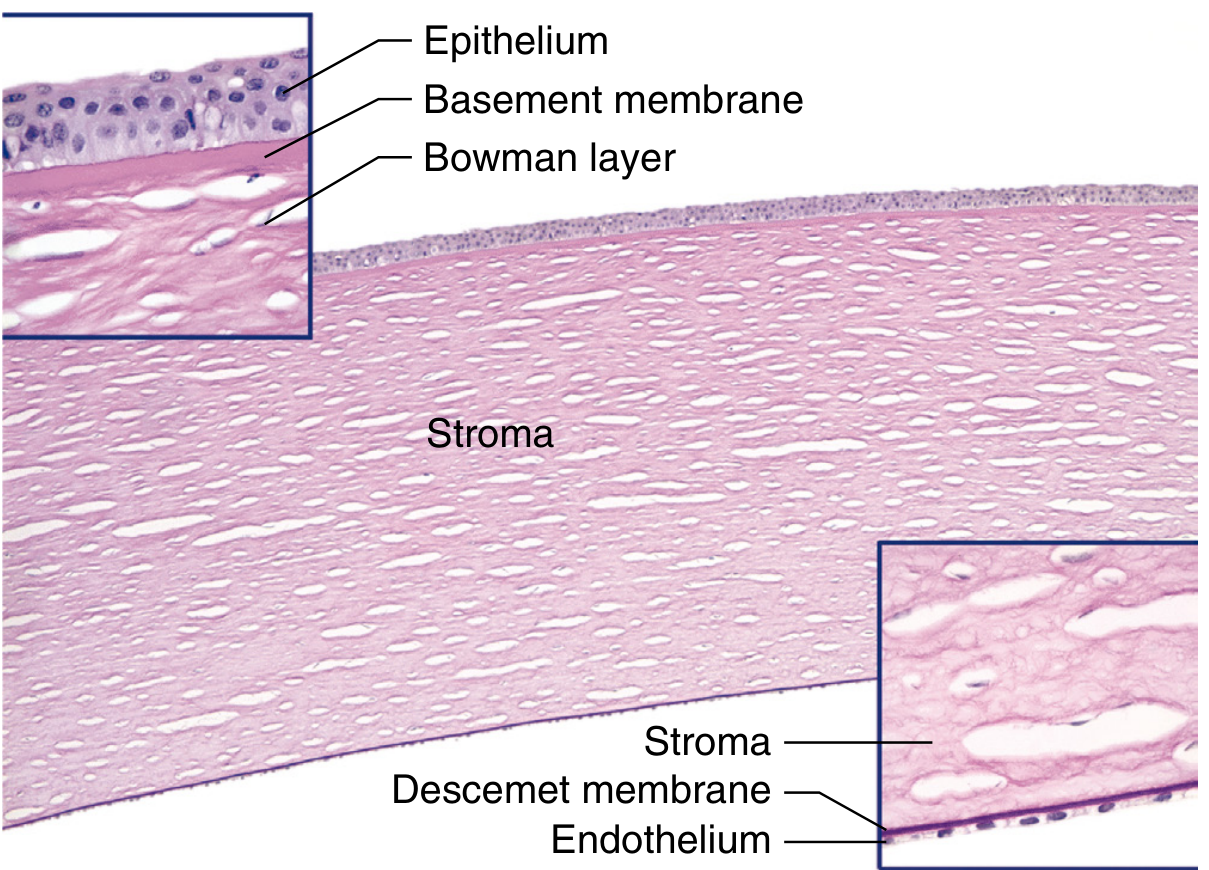
IMAGE 2 — Full-Thickness Cornea, PAS Histology
Robbins, Cotran & Kumar — Pathologic Basis of Disease, Fig. 29.7
Reading this image: PAS stain highlights basement membranes in magenta/pink. Full-thickness cornea at center - the stroma occupies 90% of the width. Upper-left inset: high power of anterior cornea - stratified epithelium on a thin PAS-positive basement membrane above the acellular Bowman layer (clearly no nuclei); Bowman transitions sharply into the stroma. Lower-right inset: high power of posterior cornea - the thick, homogeneous PAS-positive Descemet membrane above the single flat cell layer of the endothelium. The oval/slit spaces in the stroma are artifactual gaps between parallel collagen lamellae - in life these are filled with proteoglycan ground substance.
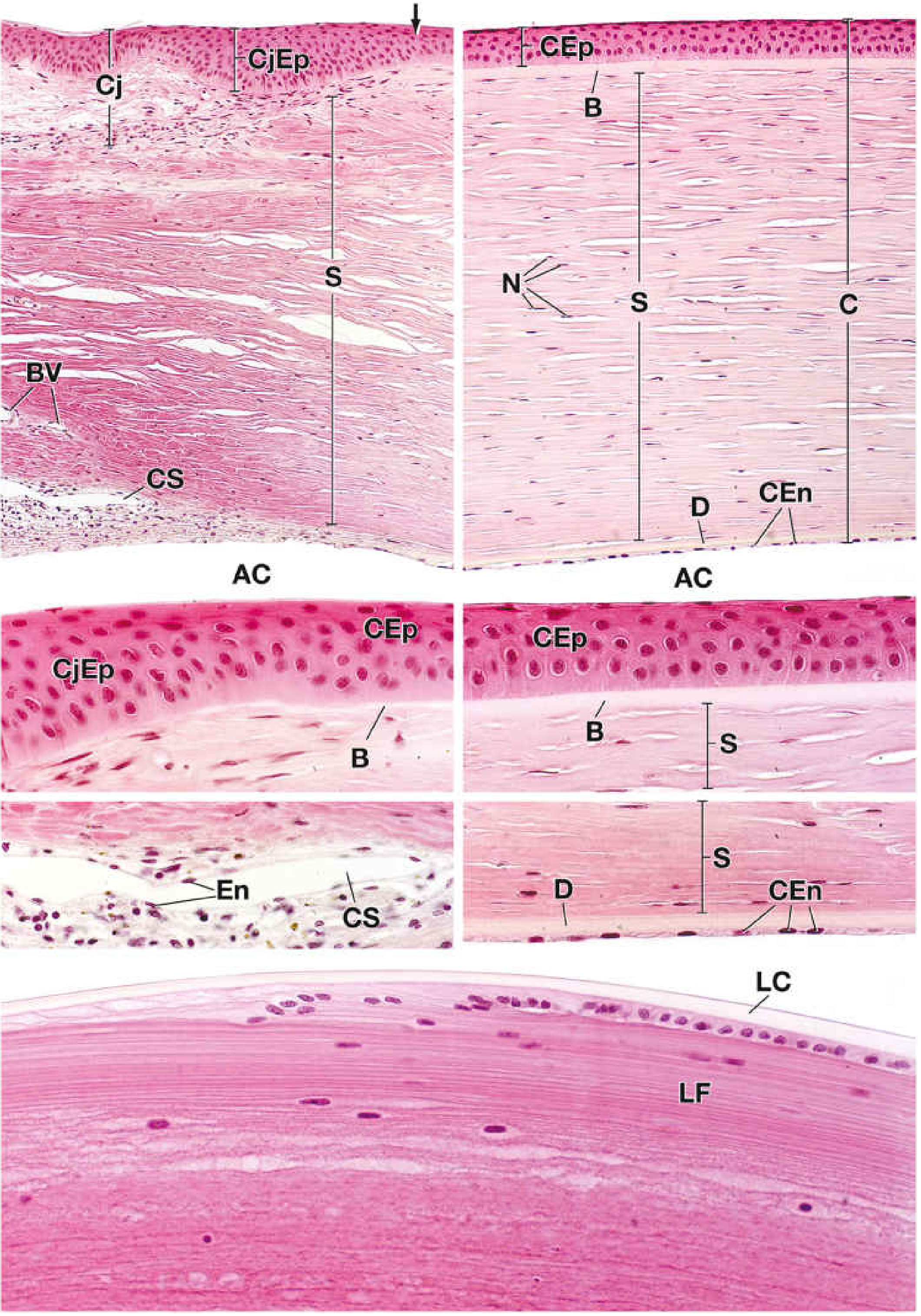
IMAGE 3 — Cornea and Limbus, H&E Multi-Panel Plate
Wheater's Functional Histology / Ross & Pawlina, Plate 24.4
Reading this plate:
- Top right panel (full-thickness cornea, ×175): CEp = corneal epithelium (uniform stratified layer); B = Bowman membrane (just visible below epithelium); S = stroma (homogeneous horizontal bands with N = keratocyte nuclei scattered between lamellae); D = Descemet membrane (thin dark line at posterior surface); CEn = corneal endothelium (flat monolayer); AC = anterior chamber below
- Top left panel (limbus, ×175): CjEp = thicker conjunctival epithelium on the scleral side; CJ = conjunctiva; BV = blood vessels in scleral stroma (cornea is avascular - their presence marks the limbus); CS = canal of Schlemm
- Middle right panel (high power epithelium/Bowman): CEp multilayer visible; B = Bowman membrane (thicker, paler, acellular zone); S = anterior stroma below
- Middle right lower (high power Descemet/endothelium): D = Descemet membrane (thick eosinophilic band); CEn = flat endothelial cells; S = posterior stroma
- Bottom panel (lens): LC = lens capsule; LF = lens fibers (no nuclei in mature lens fibers)
4.1 LAYER 1 — EPITHELIUM
Type: Non-keratinized stratified squamous epithelium
Thickness: 50-60 µm
Cell layers: 5-6
The epithelium is organized into three distinct populations:
A. Basal Cells (Single Layer — Deepest)
- Shape: Tall, columnar; 18-20 µm high, 10 µm wide
- The only mitotically active layer in the corneal epithelium
- Attached to underlying basement membrane by hemidesmosomes
- Hemidesmosome complex: α6β4 integrin → collagen XVII (BP180) → plectin/BP230 → intermediate filaments inside cell; extracellularly → laminin-332 → collagen VII anchoring fibrils → collagen IV in BM
- Loss of any component → Recurrent Corneal Erosion Syndrome (RCES)
- Connected to adjacent basal cells and wing cells above by desmosomes and gap junctions (connexin 43)
- Nuclei: oval, centrally placed, large
- Rich organelles: mitochondria (aerobic metabolism), ribosomes, rough ER, Golgi
- Contain intermediate filaments: keratin 5 (K5) and keratin 14 (K14)
B. Wing Cells (2-3 Layers — Middle)
- Shape: Polygonal with wing-like lateral cytoplasmic processes
- Post-mitotic transitional amplifying cells (TACs) - progressing toward surface
- Connected by desmosomes - primary source of epithelial mechanical cohesion
- Begin synthesizing membrane-associated mucins
- Express K5/K14 transitioning to K3/K12 as they differentiate
C. Superficial Squamous Cells (2 Layers — Surface)
- Shape: Flat, terminally differentiated; very large surface area; low nucleus-to-cytoplasm ratio
- Microplicae (surface folds) + microvilli (finger-like projections) on the apical surface:
- Dramatically increase surface area
- Anchor the tear film glycocalyx
- Bind membrane-associated mucins: MUC1, MUC4, MUC16
- Tight junctions (zonula occludens) between adjacent superficial cells form the outer blood-ocular barrier — prevent paracellular fluid movement and pathogen entry
- Express CK3 and CK12 (markers of terminally differentiated corneal epithelium)
- Lifespan: 7-10 days → programmed desquamation into the tear film
Epithelial Basement Membrane (EBM)
- Secreted by basal epithelial cells
- Composition: collagen IV, laminin-332 and laminin-511, fibronectin, entactin, perlecan
- Thickness: ~40-60 nm
- In ABMD (Map-Dot-Fingerprint Dystrophy): EBM becomes redundant and thickened, extends into the epithelium → impairs hemidesmosome reformation → recurrent erosions
Epithelial Renewal — The XYZ Hypothesis (Thoft & Friend, 1983)
X = Basal cell proliferation (vertical movement ↑)
Y = Centripetal migration from limbal stem cells (horizontal movement →)
Z = Surface cell desquamation (shed into tear film)
Homeostasis: X + Y = Z
- Complete surface cell replacement: every 7-10 days
- Full pool renewal (LSC to surface): approximately 1-2 years
- Centripetal migration rate: ~0.1-0.3 mm/day
Intercellular Junctions
| Junction | Location | Function |
|---|
| Tight junctions (zonula occludens) | Superficial cells | Outer blood-ocular barrier; paracellular resistance |
| Desmosomes | All layers (esp. wing) | Mechanical cell-cell adhesion |
| Gap junctions (connexin 43) | Basal + wing cells | Ionic and molecular communication |
| Hemidesmosomes | Basal cell — basement membrane | Epithelium-stroma adhesion |
Cell Markers Summary
| Cell Population | Key Markers |
|---|
| Limbal stem cells | p63 (high), ABCG2, N-cadherin, K14, K5; NOT K3/K12 |
| Differentiated corneal epithelium | CK3, CK12; MUC1/4/16 on surface |
| Proliferating basal cells | Ki67 positive |
4.2 LAYER 2 — BOWMAN LAYER
- Thickness: 8-14 µm (average ~12 µm)
- Nature: Acellular, condensed zone of anterior stroma — NOT a true membrane; it is the superficial portion of the stromal ECM that has been modified and compacted during development
- Composition: Randomly interwoven thin collagen fibrils — Types I (primary), III, V, VII — smaller diameter (~20-25 nm) and randomly oriented compared to the organized lamellae beneath
- Formed by: Anterior keratocytes during fetal development; secreted before birth
- Contains no cells — no regenerative ability
- Cannot regenerate once destroyed → replaced by fibrous scar tissue (fibroblast-laid irregular collagen)
- Acts as a physical barrier against:
- Epithelial-derived tumors infiltrating into stroma
- Surface microorganism penetration
- Not present in most non-primate mammals (cats, dogs, rabbits lack a true Bowman layer)
Clinical pearl: PTK (phototherapeutic keratectomy) with excimer laser removes Bowman and anterior stroma for superficial scars and dystrophies. Bowman layer does not regenerate — healed surface becomes modified fibrous tissue. However, some regenerative capacity has been reported with LASEK epithelial flaps preserving the plane.
4.3 LAYER 3 — STROMA
The stroma is the bulk of the cornea — 90% of total thickness (~450-500 µm centrally), and the structural/optical backbone.
Overall Composition
| Component | Proportion | Role |
|---|
| Collagen fibrils | ~70% of dry weight | Structural support; transparency (Maurice lattice) |
| Proteoglycans (GAGs) | ~10% of dry weight | Maintain fibril spacing; regulate hydration |
| Keratocytes | ~10% of stromal volume | ECM maintenance; wound healing; scar formation |
| Water | ~78% of wet weight | Maintained in controlled amount by endothelial pump |
Collagen Organization
- 200-300 lamellae total, running full width of the cornea (limbus to limbus)
- Collagen type: Primarily Type I with Types III, V, VI, XII, XIV
- Fibril diameter: Strictly uniform 25-35 nm — this uniformity is fundamental to transparency
- Compare: sclera has variable diameters of 25-250 nm → opaque
- Inter-fibril spacing: ~60-64 nm center-to-center, maintained by proteoglycans
- Within each lamella: fibrils are parallel to each other
- Between lamellae: angle varies (adjacent lamellae are oriented at angles to each other, creating a quasi-orthogonal lattice)
Regional differences:
| Region | Lamellar arrangement | Clinical significance |
|---|
| Anterior 1/3 | More oblique, highly interwoven; lamellar interdigitations | Greater biomechanical strength; CXL effect deepest here; LASIK flap resistant to dislodgement |
| Posterior 2/3 | More orthogonal, well-separated parallel lamellae | Cleaner cleavage planes; basis for DALK Big-Bubble technique |
Maurice's Lattice Theory of Transparency (1957)
This is the molecular basis of corneal transparency:
- Uniform fibril spacing (~60 nm) is much less than the wavelength of visible light (400-700 nm)
- Scattered light waves from adjacent fibrils are exactly out of phase → destructive interference
- Net result: scattered light cancels; transmitted (forward-directed) light passes through unimpeded
Conditions disrupting the lattice → opacity:
- Stromal oedema: increased hydration → fibrils pushed apart → irregular spacing → scattering increases
- Scarring: irregular fibril diameters and random orientation (healing produces Type III collagen, not uniform Type I)
- Infiltrates: cells displace fibrils
- Dystrophies: abnormal deposits in fibril spaces (granular, macular, lattice)
Proteoglycans — The Spacing Molecules
| Proteoglycan | Core protein | GAG side chain | Location | Primary function |
|---|
| Lumican | SLRP (leucine-rich repeat) | Keratan sulfate | Entire stroma | Maintains fibril spacing; most abundant |
| Keratocan | SLRP | Keratan sulfate | Entire stroma | Fibril spacing; unique to cornea |
| Mimecan | SLRP | Keratan sulfate | Anterior stroma | Minor; fibril regulation |
| Decorin | SLRP | Dermatan sulfate | Posterior stroma | Fibril spacing; TGF-β binding |
| Biglycan | SLRP | Dermatan sulfate | Posterior stroma | Minor structural role |
Biochemical uniqueness of the corneal stroma: The cornea is the only tissue in the body where keratan sulfate (not chondroitin sulfate) is the dominant GAG. This highly sulfated molecule with its unique charge and spacing properties is essential for maintaining the precise 60 nm inter-fibril distance.
Macular Corneal Dystrophy (CHST6 mutation): Keratan sulfate synthesis is disrupted. Without proper KS, proteoglycans cannot maintain fibril spacing → diffuse stromal opacification with no clear zones (unlike granular dystrophy which has clear zones).
Keratocytes
- Specialized resident corneal fibroblasts — derived from neural crest
- Morphology: Flat, stellate (star-shaped) cells with long branching cytoplasmic processes that connect to adjacent keratocytes via gap junctions → form a continuous 3D syncytial network throughout the stroma
- Density: ~20,000-25,000 cells/mm² in anterior stroma → decreasing to ~10,000 cells/mm² posteriorly
- In healthy stroma: metabolically quiescent — slow turnover, maintaining ECM
- Refractive index of quiescent keratocyte (~1.359) matched to surrounding ECM → minimizes light scattering from the cells themselves
Wound healing response:
Injury
↓
Epithelium releases IL-1α and TNF-α
↓
Anterior keratocytes undergo APOPTOSIS (hours)
↓ (days 1-4)
Remote keratocytes receive EGF, FGF, PDGF signals
↓
Transform into FIBROBLASTS (proliferate, migrate)
↓
Some further become MYOFIBROBLASTS (α-SMA+)
↓
Myofibroblasts produce irregular Type III collagen
= CORNEAL HAZE / SCAR
- More extensive apoptosis with PRK (surface ablation; direct epithelial destruction) than LASIK (flap creation; less epithelial-stromal interface disruption)
- MMPs (MMP-1, -2, -9) from activated keratocytes → ECM remodeling; excessive activation → ulceration/melting
4.4 LAYER 4 — DUA'S LAYER (Pre-Descemet Layer)
Described by Professor Harminder Dua, University of Nottingham, 2013
- Thickness: 10-15 µm
- Location: Between the posterior stroma and Descemet membrane
- Composition: 5-8 compact lamellae of Type I collagen, more densely packed than the regular stroma
- Acellular: no keratocytes
- Mechanical strength: Surprisingly strong — withstands pressures up to 700-1200 mmHg when isolated; far stronger than the stroma
Clinical significance:
| Scenario | Role of Dua's Layer |
|---|
| DALK — Big Bubble Type 1 | Air injected at stroma-Dua's plane → air dissects cleanly at this interface → ideal surgical result; creates bare Dua's layer on the host bed |
| DALK — Big Bubble Type 2 | Air injected within Dua's layer → slightly larger bubble, less ideal; more fragile |
| Acute corneal hydrops | Descemet membrane ruptures at the Dua's layer-Descemet interface → aqueous rushes into stroma → sudden white cloudy oedema |
| Significance in keratoplasty | Pre-Descemet plane serves as the natural cleavage zone; its strength explains why Big Bubbles can hold pressure without rupturing |
4.5 LAYER 5 — DESCEMET MEMBRANE
- Nature: The basement membrane of the corneal endothelium — secreted by endothelial cells throughout life
- Composition: Collagen IV (primary PNBZ), Collagen VIII (primary ABZ), laminin, fibronectin, perlecan, nidogen/entactin
Thickness Across Life
| Timepoint | Thickness |
|---|
| Birth | ~3-4 µm |
| Adult (central) | 10-12 µm |
| Elderly | 14-20 µm |
| Fuchs dystrophy | 20-30+ µm (with guttata) |
Two Zones — Critical Distinction
| Zone | Abbreviation | Formed | Collagen | EM Appearance |
|---|
| Anterior banded zone | ABZ | In utero (fetal period) | Type VIII collagen (hexagonal lattice) | Banded: regular cross-striations ~100 nm periodicity |
| Posterior non-banded zone | PNBZ | Postnatal — secreted throughout life | Type IV collagen (primary) | Homogeneous; no banding |
Cornea guttata (Fuchs dystrophy) = nodular excrescences on the PNBZ — rounded projections of excess abnormal collagen VIII secreted by dysfunctional endothelial cells. On specular microscopy: dark spots disrupting hexagonal mosaic. In advanced Fuchs: "beaten metal" or "hammered silver" appearance.
Regenerative Capacity
- Unlike Bowman layer, Descemet membrane CAN regenerate
- Endothelial cells continue secreting new PNBZ throughout life
- Basis for: spontaneous partial healing of Haab striae (forceps birth trauma); persistence of DMEK graft viability as a coherent tissue unit
Scrolling Behavior (Important for DMEK Surgery)
When stripped from the stroma (as in DMEK graft preparation), Descemet membrane spontaneously scrolls with the endothelium on the outer/convex surface:
- Because: ABZ (fetal collagen VIII, highly cross-linked, stiffer) is anterior → resists elongation → curls the sheet toward the PNBZ side
- The graft must be gently unscrolled during DMEK insertion
- Tamponaded with an air bubble to adhere to the host posterior stroma
4.6 LAYER 6 — ENDOTHELIUM
The most physiologically critical layer of the cornea.
Structure
- Single monolayer of flattened polygonal cells — predominantly hexagonal (~70-80% hexagonality in healthy adults)
- Cell diameter: ~18-20 µm; cell height (thickness): ~5 µm
- No regenerative capacity in humans (see physiology section)
- Cause: G1 cell cycle arrest maintained by high p27^kip1 expression and TGF-β2 from aqueous humor
- When cells are lost: neighboring cells enlarge (polymegethism) and change shape (pleomorphism) to cover the bare Descemet surface
Cell Density Across Life
| Life Stage | Endothelial Cell Density (ECD) |
|---|
| Newborn | ~3,500-4,000 cells/mm² |
| Young adult (20s) | ~2,500-3,000 cells/mm² |
| Physiological loss | ~0.6% per year |
| Age 80 | ~2,000 cells/mm² |
| Decompensation threshold | ~500 cells/mm² |
| Caution for intraocular surgery | <1,000-1,200 cells/mm² |
Specular Microscopy Parameters (Normal)
| Parameter | Normal Value |
|---|
| ECD (endothelial cell density) | >2,000 cells/mm² |
| Hexagonality (% hexagonal cells) | >60% (ideally >70%) |
| Coefficient of variation (CV) of cell area | <0.30 |
Tight Junction Structure
- Endothelial cells are connected by tight junctions (zonula occludens) and gap junctions
- BUT: these tight junctions are leaky (not truly impermeable like the RPE tight junctions)
- Low transendothelial resistance → fluid continuously leaks inward from aqueous to stroma (passive)
- The active pump must continuously counteract this leak ("leak-pump" model)
SECTION 5: PHYSIOLOGY
5.1 CORNEAL TRANSPARENCY — FOUR MECHANISMS
Mechanism 1: Regular Collagen Lattice (Maurice, 1957)
- Uniform fibril diameter (25-35 nm) + Regular spacing (~60 nm) maintained by proteoglycans
- Spacing < wavelength of visible light (400-700 nm)
- Destructive interference of scattered light → all scattered photons cancel → transmitted light passes unimpeded
If Maurice's two conditions are violated (uniform diameter + regular spacing), the cornea scatters light and becomes opaque. This happens in oedema, scarring, and dystrophies.
Mechanism 2: Relative Dehydration
- Normal water content: 78% (swollen, opaque cornea >84%)
- Stroma is inherently hydrophilic (proteoglycans attract water)
- Active dehydration maintained by:
- Endothelial pump (primary, ~80% of dehydration control)
- Epithelial tight junction barrier (passive; prevents tear film entry)
- Surface evaporation (minor; explains why tight patching of eye can cause mild oedema)
Mechanism 3: Avascularity
- No blood vessels = no haemoglobin, red blood cells, or vessel walls to scatter light
- Maintained by active anti-angiogenic balance:
- sFlt-1 (soluble VEGF receptor-1): acts as a VEGF trap; secreted by corneal keratocytes
- Thrombospondin-1 (TSP-1): anti-angiogenic factor in stroma
- PEDF (pigment epithelium-derived factor), endostatin, angiostatin
- Low baseline VEGF-A in normal stroma
When anti-angiogenic balance tips:
- Chronic hypoxia (contact lens) → VEGF-A upregulation → superficial neovascularization
- Limbal stem cell deficiency → conjunctivalization + vascularization
- Chemical burns → massive VEGF release → aggressive neovascularization
Mechanism 4: Unmyelinated Nerve Fibers
- Myelin is lipid-rich → intensely scatters light
- Corneal nerve fibers lose their myelin sheaths at the limbus as they enter the cornea
- Unmyelinated fibers within stroma are <1-2 µm in diameter → too small to scatter visible light significantly
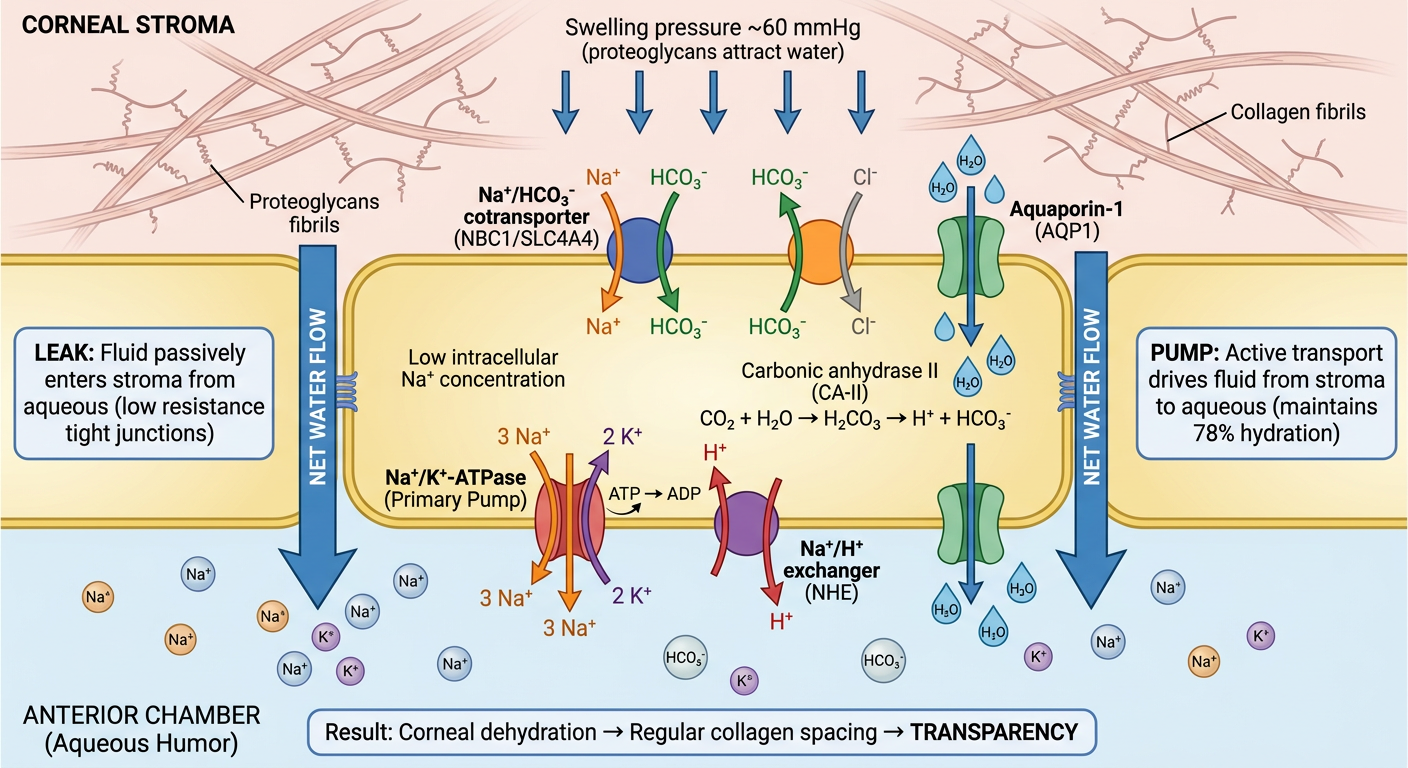
5.2 THE ENDOTHELIAL PUMP — MOLECULAR DETAIL
This is the most important physiological mechanism in the cornea.
The Problem: Swelling Pressure
The stroma exerts an imbibition pressure of ~60 mmHg — its proteoglycans constantly attempt to draw water in and swell. Without the pump, the cornea would swell to 3-4× normal thickness.
Step-by-Step Pump Mechanism
STROMA (high relative water content)
↑ passive leak (aqueous → stroma)
ENDOTHELIAL CELL
│
├── Step 1: Na⁺/K⁺-ATPase (basolateral/lateral membrane)
│ Pumps 3 Na⁺ OUT (→ aqueous)
│ Pumps 2 K⁺ IN
│ Creates low intracellular [Na⁺]
│
├── Step 2: Carbonic Anhydrase (CA-II intracellular, CA-IV membrane)
│ CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻
│
├── Step 3: HCO₃⁻ secretion (apical/posterior membrane)
│ NBC1/SLC4A4: Na⁺ + HCO₃⁻ cotransporter → HCO₃⁻ into aqueous
│ AE2: Cl⁻/HCO₃⁻ exchanger → HCO₃⁻ into aqueous
│ NHE: Na⁺/H⁺ exchanger → H⁺ out
│
├── Step 4: Osmotic gradient established
│ HCO₃⁻ accumulates in aqueous → draws water osmotically
│
└── Step 5: Water transport (apical membrane)
Aquaporin-1 (AQP-1) water channels
Water moves: stroma → through cell → aqueous
AQUEOUS HUMOR (net water flow out of stroma)
"Leak-Pump" Model
Aqueous ──(passive leak, continuous)──→ Stroma
Stroma ──(active pump, continuous)──→ Aqueous
Balance maintained = 78% hydration = transparency
Pump overwhelmed (≤500 cells/mm²) = oedema = opacity
Key Drug Interactions with the Pump
| Drug / Condition | Mechanism | Clinical Effect |
|---|
| CA inhibitors (dorzolamide, acetazolamide) | Inhibit carbonic anhydrase → reduce HCO₃⁻ secretion | Mild corneal thickening; use to temporize bullous keratopathy |
| Elevated IOP (acute angle closure) | Opposes pump-driven fluid movement | Acute stromal oedema ("steamy" cornea on slit lamp) |
| Cold storage (<15°C - MK medium at 4°C) | Reduces Na⁺/K⁺-ATPase activity | Deliberate swelling in eye banking |
| Ouabain | Directly blocks Na⁺/K⁺-ATPase | Immediate pump cessation (experimental only) |
| ROCK inhibitors (Y-27632, ripasudil) | Inhibit Rho kinase → override G1 arrest → promote endothelial proliferation and migration | Enable endothelial cell therapy for FECD; improve graft cell survival post-DMEK |
5.3 CORNEAL METABOLISM
The cornea is metabolically active despite being avascular — energy needs met by three nutrient routes:
Nutrient Sources by Layer
| Layer | Primary Oxygen Source | Primary Glucose Source |
|---|
| Epithelium | Atmospheric O₂ via tear film (most important) | Aqueous humor |
| Stroma | Dissolved O₂ in aqueous (via diffusion) | Aqueous humor; anaerobic glycolysis |
| Endothelium | Dissolved O₂ in aqueous | Aqueous humor; aerobic metabolism |
Metabolic Pathways
Epithelium:
- Normally: aerobic oxidative phosphorylation (from atmospheric O₂) → efficient ATP production
- Under contact lens / hypoxia: forced shift to anaerobic glycolysis → lactate → local acidosis → CO₂ accumulation → epithelial oedema → microcysts
- Chronic hypoxia threshold:
- Dk/t < 24 × 10⁻⁹ for daily wear: risk of limbal hyperaemia, microcysts, superficial neovascularization
- Dk/t < 87 × 10⁻⁹ for extended overnight wear
Stroma:
- Keratocytes: mostly anaerobic glycolysis; low energy demand in quiescent state
- Some O₂ diffusion from aqueous humor
Endothelium:
- Highly metabolically active (must continuously run Na⁺/K⁺-ATPase)
- Aerobic oxidative phosphorylation predominates
- Relies entirely on aqueous humor for glucose and O₂
Growth Factors in the Tear Film (Supporting Epithelium)
| Growth Factor | Source in Tears | Role |
|---|
| EGF (epidermal growth factor) | Lacrimal gland | Epithelial proliferation (primary mitogen) |
| HGF (hepatocyte growth factor) | Lacrimal gland | Migration and proliferation |
| KGF / FGF-7 | Stromal keratocytes | Epithelial proliferation |
| Substance P (SP) | Corneal nerves | Cell adhesion and proliferation |
| IGF-1 | Lacrimal gland | Metabolic support |
| TGF-β | Multiple sources | Wound healing; fibrosis |
| Vitamin A (retinol) | Tear film | Prevents squamous metaplasia |
5.4 CORNEAL INNERVATION
"The cornea is the most densely innervated tissue in the human body" — ~7,000 nerve endings/mm²; 300-400× more dense than skin
Nerve Supply
Sensory (primary):
- Branches of the nasociliary nerve (branch of ophthalmic division V1 of trigeminal nerve, CN V)
- Via 2-3 long ciliary nerve branches running anteriorly in the suprachoroidal space
- Enter the corneal stroma at the peripheral limbus (predominantly at 3 and 9 o'clock meridians)
- As they enter the limbus: myelin sheaths are lost (preserving transparency)
- Within the stroma: exclusively unmyelinated C-fibers and thinly myelinated Aδ-fibers
Autonomic:
- Sparse sympathetic fibers (superior cervical ganglion via long ciliary nerves): role in epithelial metabolic regulation and stem cell support
- No direct parasympathetic innervation of corneal tissue
Two Intracorneal Plexuses
1. Deep Stromal Plexus:
- Main nerve trunks travel radially in the mid-stroma toward the center
- Give off branches upward toward the epithelium
- Not directly involved in surface sensation
2. Sub-Basal Nerve Plexus (SBN Plexus) — The Most Important:
- Fine nerve fibers running immediately beneath the basal epithelial cells (just above Bowman layer)
- Form a dense, whorl-shaped spiral pattern centered slightly inferior to the geometric corneal center
- Visible on in vivo confocal microscopy (IVCM) — best clinical tool to assess corneal nerve health
- These SBN fibers send ascending intraepithelial terminals up through the basal cell layer → between epithelial cells → to the surface
- Primary source of all corneal sensation
- The whorl pattern mirrors the centripetal migration pattern of limbal stem cells (both converge on the center)
Fiber Types and Sensations
| Fiber Type | Diameter | Mediates |
|---|
| Aδ fibers (unmyelinated in cornea) | 2-5 µm → 0 µm in cornea | Rapid, sharp pain; mechanical stimuli (initial stab from foreign body or abrasion) |
| C fibers (unmyelinated) | 0.2-1.5 µm | Slow burning/aching pain; thermal; polymodal responses; reflex lacrimation |
| Mechano-nociceptors | C + Aδ | Touch, pressure |
| Polymodal nociceptors | C (most common) | Chemical (pH change, inflammatory mediators, hypertonic tear film), thermal, mechanical |
| Cold thermoreceptors | C | Tonically active at rest (provide continuous afferent drive for basal lacrimation) |
Reflex Arcs
Corneal Blink Reflex:
Corneal stimulus
↓ (afferent)
Nasociliary nerve → CN V1 → trigeminal main sensory nucleus
↓ (efferent - bilateral)
Both facial nerve nuclei (CN VII) → zygomatic branches
↓
Bilateral orbicularis oculi contraction → blink
- Tests CN V1 (afferent) and CN VII (efferent)
- Absent/diminished in: acoustic neuroma, lateral medullary syndrome (Wallenberg), trigeminal schwannoma, Bell's palsy
Corneal-Lacrimal Reflex:
Corneal stimulus → CN V1 → parasympathetic superior salivatory nucleus
↓
Greater petrosal nerve → pterygopalatine ganglion → lacrimal gland
↓
Reflex lacrimation
Consequences of Denervation — Neurotrophic Keratopathy (NK)
The corneal nerves do more than just sense — they provide trophic support to the epithelium:
- Neuropeptides released: Substance P, neuropeptide Y, calcitonin gene-related peptide (CGRP)
- Nerve growth factor (NGF) produced by corneal epithelial cells in an autocrine/paracrine loop — NGF supports epithelial proliferation, migration, and adhesion
- Loss of innervation → loss of trophic factors → impaired epithelial wound healing → trophic ulcer
Mackie Clinical Staging:
| Stage | Features |
|---|
| I | Superficial punctate keratopathy; epithelial irregularity; reduced tear film stability |
| II | Persistent epithelial defect (PED); no healing |
| III | Stromal ulceration; risk of perforation and endophthalmitis |
Causes of NK:
- HSV/HZO keratitis (most common - viral damage to trigeminal ganglion + corneal nerves)
- CN V surgery (acoustic neuroma resection, skull base surgery, trigeminal rhizotomy)
- Cavernous sinus lesions
- Diabetes mellitus (peripheral neuropathy)
- Topical anaesthetic abuse
- Riley-Day syndrome (familial dysautonomia - congenital absence of sensory neurons)
Corneal Sensitivity Testing:
- Cochet-Bonnet esthesiometer: nylon monofilament 0.12 mm diameter; variable length 5-60 mm
- 60 mm = minimum detectable force = maximum sensitivity
- Normal central: ≥50 mm
- Reduced in: HSV keratitis, post-LASIK (6-24 months recovery), post-CXL (transient), NK, DM
5.5 WOUND HEALING
Epithelial Wound Healing — Three Phases
Phase 1: Cell Migration (0-24 hours)
- Immediately after wounding: cells flatten, extend lamellipodia; no mitosis in this phase
- Actin cytoskeleton reorganization drives cell spreading
- Fibronectin (from aqueous/serum) coats the wound bed = provisional scaffold for cell migration
- Key growth factors: EGF, HGF, KGF (FGF-7), Substance P, neuropeptide Y
- Migration rate: ~1 mm² heals in 24-36 hours under normal conditions
Phase 2: Proliferation (24-72 hours)
- Once the leading edges bridge the defect: EGFR signaling triggers basal cell mitotic division
- Cells divide to restore normal multilayer architecture
- Migration continues (outpaces proliferation initially)
Phase 3: Adhesion Reformation (3 days to several weeks)
- Hemidesmosomes reform: collagen VII anchoring fibrils, BP180, BP230, α6β4 integrin complex
- Full mechanical strength of epithelial adhesion: several weeks
- This explains the window of vulnerability for recurrent erosion after trauma or in ABMD
Smoking retards corneal epithelialization and should be discontinued in any patient with an epithelial problem (Kanski 10th Ed.)
Stromal Wound Healing — Molecular Cascade
Phase 1: Keratocyte Apoptosis (within hours)
- Trigger: IL-1α and TNF-α released from wounded epithelium diffuse into anterior stroma
- Anterior keratocytes undergo rapid apoptosis → "sterile necrotic zone" free of cells
- Depth of apoptosis correlates with depth of epithelial injury
- PRK: extensive anterior keratocyte apoptosis (direct epithelial ablation)
- LASIK: more limited (epithelium only minimally disturbed; flap creation is subsurface)
Phase 2: Keratocyte Activation (days 1-4)
- Remote keratocytes receive: EGF, FGF-2, PDGF, TGF-β from tears and stroma
- Activated into: fibroblasts (proliferate and migrate) → some → myofibroblasts (α-SMA positive)
Phase 3: Matrix Remodeling (weeks to years)
- Myofibroblasts produce Type III collagen (irregular diameter, random orientation) → haze
- MMPs (MMP-1 collagenase, MMP-2 gelatinase, MMP-9) remodel ECM
- Ideal outcome: myofibroblasts undergo apoptosis; fibroblasts revert to keratocytes; Type III collagen gradually replaced → haze fades (6-18 months post-PRK)
- Poor outcome: persistent TGF-β1 stimulation (from defective EBM) → sustained myofibroblast activity → dense permanent scar
Key: Why LASIK causes less haze than PRK:
- LASIK: epithelial basement membrane intact → TGF-β1 cannot diffuse from tears into stroma → keratocytes not activated to myofibroblasts → minimal haze
- PRK: EBM completely removed by ablation → TGF-β1 floods stroma until EBM regenerates → haze risk
Mitomycin C (MMC 0.02%, applied for 20-40 seconds post-PRK ablation): alkylating agent → DNA cross-linking → inhibits fibroblast and myofibroblast proliferation → dramatically reduces post-PRK haze. Standard of care for PRK ablations >50-60 µm depth.
Endothelial Wound Response
- Endothelial cells cannot proliferate in humans (G1 cell cycle arrest - high p27^kip1; TGF-β2 from aqueous humor maintains this block)
- Response to cell loss: neighboring cells enlarge (polymegethism) and migrate (pleomorphism) to cover exposed Descemet
- ROCK inhibitors (Y-27632, ripasudil) override this G1 arrest → limited endothelial cell proliferation possible → therapeutic platform for:
- Fuchs endothelial corneal dystrophy (FECD)
- Post-DMEK endothelial cell density recovery
- Cultivated endothelial cell injection therapy (Japan - one donor → 50-100+ recipients)
5.6 TEAR FILM ANATOMY AND PHYSIOLOGY
The tear film is the true optical anterior surface of the eye — its quality determines the smoothness of the refracting surface.
Three-Layer Model
(Note: The modern model describes a continuous mucin-aqueous gradient, but the three-layer model remains clinically standard)
| Layer | Position | Thickness | Source | Key Components | Primary Function |
|---|
| Lipid | Outermost | 0.1-0.2 µm | Meibomian glands (modified sebaceous); accessory Zeis and Moll glands | Phospholipids, wax esters, sterol esters, polar lipids (inner spreading layer) | Retards evaporation by 90-95%; prevents aqueous spillover over lid margin |
| Aqueous | Middle | ~7-8 µm (~90% of tear volume) | Main lacrimal gland (reflex secretion); accessory glands of Krause and Wolfring (basal/tonic secretion) | Water, electrolytes (Na⁺, K⁺, Cl⁻, HCO₃⁻), proteins (lysozyme, lactoferrin, secretory IgA, albumin), EGF, retinol | Oxygen + nutrient delivery; antimicrobial; mechanical debris clearance |
| Mucin | Innermost (glycocalyx) | ~0.02-0.05 µm | Goblet cells (conjunctiva - MUC5AC); corneal/conjunctival epithelial cells (membrane-bound mucins) | MUC5AC (secreted, gel-forming); MUC1, MUC4, MUC16 (membrane-associated, on epithelial surface) | Converts hydrophobic epithelial surface to hydrophilic; anchors aqueous layer; fills microplicae |
Tear Film Functions
- Optical: Provides the smooth, regular anterior refracting surface — tear film irregularity = higher-order aberrations = blur
- Oxygen delivery: Primary O₂ source for epithelium (pO₂ ~155 mmHg in open eye)
- Nutrition: Glucose, amino acids
- Antimicrobial:
- Lysozyme (~25% of total protein): hydrolyzes Gram-positive bacterial cell walls (cleaves β-1,4 glycosidic bonds in peptidoglycan)
- Lactoferrin: chelates iron → bacteriostatic
- Secretory IgA (sIgA): predominant tear immunoglobulin; neutralizes pathogens, prevents adhesion
- β-defensins 1, 2, 3: antimicrobial peptides; upregulated in infection
- Wound healing: EGF, HGF, fibronectin, TGF-β, retinol accelerate epithelial repair
- Mechanical lubrication: Reduces friction between corneal surface and palpebral conjunctiva with each blink (blinking 15-20 times/min)
Tear Film Break-Up Time (TBUT)
- The interval between a complete blink and the appearance of the first dry spot on the corneal surface
- Normal: >10 seconds (non-invasive TBUT)
- Abnormal: <5 seconds = tear film instability → evaporative dry eye
- Mechanism of break-up: Meibomian gland dysfunction → inadequate lipid layer → accelerated aqueous evaporation → mucin layer becomes exposed → air/hydrophobic surface contact → break-up
5.7 ANTI-ANGIOGENIC MECHANISMS AND VASCULARIZATION
Normal Avascularity — Molecular Balance
| Anti-angiogenic factors (normal cornea) | Pro-angiogenic factors (suppressed) |
|---|
| sFlt-1 (soluble VEGF receptor-1) | VEGF-A |
| Thrombospondin-1 (TSP-1) | VEGF-C (lymphangiogenesis) |
| PEDF (pigment epithelium-derived factor) | bFGF / FGF-2 |
| Endostatin | IL-8 / CXCL8 |
| Angiostatin | MMP-2, MMP-9 |
| Decorin (sequesters growth factors) | PDGF |
When this balance is disrupted (inflammation, injury, LSCD, hypoxia) → neovascularization:
Types of corneal neovascularization:
- Superficial (pannus): above or in Bowman layer; from chronic surface irritation, trachoma, CL
- Deep stromal: from limbal vessels invading full stroma; interstitial keratitis (syphilis, TB, HSV)
- Ghost vessels: regressed vessels (no flowing blood); appear as faint tubular shadows; classic in old syphilitic interstitial keratitis
5.8 LIMBAL STEM CELL BIOLOGY
Limbal Architecture
- Limbus = ~1.5-2 mm annular transition zone
- Palisades of Vogt: radial fibrovascular ridges at superior and inferior limbus (best seen on slit-lamp with diffuse illumination)
- Limbal crypts: deep furrows beneath the palisades; structural niche for LSCs
- Rich capillary network from anterior ciliary arteries — the only blood supply in proximity to the cornea
LSC Hierarchy (Four Populations)
True Limbal Stem Cells (LSCs)
↓ asymmetric division
Transient Amplifying Cells (TACs) — rapidly dividing
↓ commitment to differentiation
Post-mitotic Wing Cells
↓ terminal differentiation
Terminally Differentiated Surface Squamous Cells
↓ desquamation (7-10 days)
Shed into tear film
LSC Characteristics
| Feature | LSC | Differentiated Corneal Epithelium |
|---|
| Proliferative state | Slow cycling (label-retaining) | Mitotically active (basal) or post-mitotic |
| Nucleus:cytoplasm ratio | High | Low |
| Key markers | p63 (high), ABCG2, N-cadherin, K5, K14 | CK3, CK12, MUC1/4/16 |
| Ki67 | Negative (quiescent) | Positive in basal layer |
| MHC class II | Negative (immune privilege) | Negative |
Niche Factors Maintaining LSC Quiescence
- Physical: Fibrovascular stroma of palisades provides structural support
- Soluble signals: Wnt signaling, Notch signaling, BMP pathway
- ECM: Tenascin-C, fibronectin, laminin-511 in limbal basement membrane
- Paracrine: Limbal fibroblasts secrete keratocan and hepatocyte growth factor (HGF); limbal melanocytes provide UV protection to LSC DNA
- Autocrine: LSCs produce their own niche signals
Centripetal Migration — The Y Component
Evidence:
- Lineage tracing in mouse corneas: clonal strips of labeled epithelium extend from limbus to center
- Human evidence: IVCM shows the sub-basal nerve whorl pattern mirrors the centripetal epithelial migration
- Whorl-like epithelial patterns after LSCD recovery correspond to sectors of residual stem cell activity
Clinical consequences of LSCD:
- Loss of Y component → X cannot compensate alone → Z exceeds supply
- Conjunctival epithelium grows over corneal surface (conjunctivalization)
- Signs: irregular epithelium, goblet cells on corneal surface (CK7-positive), superficial vascularization, persistent epithelial defects, photophobia, blurred vision
SECTION 6: CORNEAL OPTICS
6.1 Refractive Power
The cornea refracts light at two surfaces:
| Surface | Interface | Power |
|---|
| Anterior | Air (n=1.000) / tear film (n=1.336) / corneal stroma (n=1.376) | ~+48.8 D |
| Posterior | Corneal stroma (n=1.376) / aqueous humor (n=1.336) | ~-5.8 D |
| Net corneal power | | ~+43 D |
- Keratometric index (n=1.3375): simplified index used by all keratometers that combines both surfaces into one calculation from the anterior curvature alone
- Post-refractive surgery problem: keratometers still use n=1.3375 but the anterior surface is now flatter (ablated) while the posterior surface is unchanged → IOL calculation formulae underestimate corneal power → hyperopic surprise after cataract surgery → must use Holladay/Barrett/Shammas post-LASIK formulae
6.2 Asphericity (Q value)
- Q = 0: perfect sphere
- Q < 0 (prolate - NORMAL cornea): flatter periphery than center; Q ≈ -0.26 normally
- Prolate shape: peripheral light rays are refracted less strongly than paraxial rays → both converge near the same focal point → minimizes spherical aberration
- Q > 0 (oblate): steeper periphery; occurs after standard myopic LASIK
- Oblate shape: peripheral rays refracted more strongly → focus anterior to paraxial → increased positive spherical aberration → night halos, glare, reduced contrast sensitivity
6.3 Higher-Order Aberrations
| Aberration | Description | Clinical Causes |
|---|
| Spherical aberration (Z₄⁰) | Peripheral vs paraxial focus difference | Standard myopic LASIK → positive SA increase; night halos |
| Coma (Z₃±¹) | Asymmetric; comet-shaped blur | Decentered ablation; keratoconus |
| Trefoil (Z₃±³) | Three-fold symmetric | Keratoconus; post-DALK interface |
| Normal total RMS HOAs | ~0.3-0.5 µm (measured by Hartmann-Shack wavefront sensor) | |
SECTION 7: ANATOMICAL RELATIONS
Cornea and Anterior Chamber Angle
- Anterior chamber depth: 2.5-3.5 mm (endothelium to anterior lens capsule)
- Aqueous humor directly bathes the endothelium → primary metabolic source
- Gonioscopic landmarks (anterior to posterior):
- Schwalbe's line (peripheral terminal of Descemet membrane)
- Trabecular meshwork
- Scleral spur
- Ciliary body face + iris root
Cornea and Cataract Surgery
- During phacoemulsification: every instrument entering through the corneal wound passes within millimetres of the endothelium
- OVD (ophthalmic viscosurgical device = viscoelastic) is applied to coat and protect endothelium from: direct trauma, irrigation turbulence, ultrasound energy
- In Fuchs dystrophy: torsional phacoemulsification (reduced ultrasound time) preferred; CCT monitoring perioperatively; consider triple procedure (phaco + DMEK combined)
IMAGE 4 — Keratoconus: Oil-Droplet Red Reflex
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.39A
What this shows: The "oil droplet" red reflex viewed at 0.5 m with direct ophthalmoscope. The conical corneal distortion refracts the red reflex unevenly — producing a well-demarcated darker central zone (the cone) surrounded by a brighter annular ring. One of the earliest clinically detectable signs of keratoconus. The darker center represents the cone apex where light is refracted away from the observer.
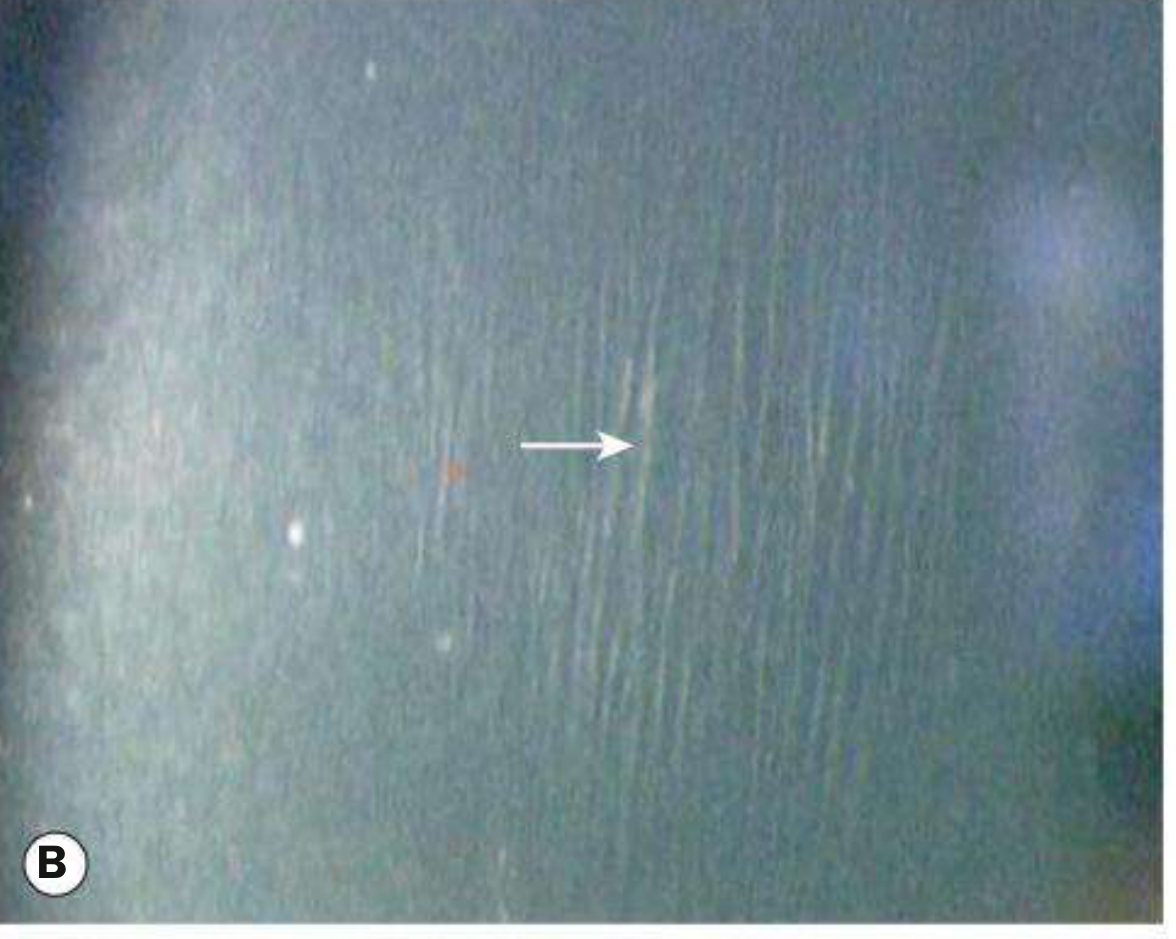
IMAGE 5 — Keratoconus: Vogt Striae
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.39B
What this shows: Fine, vertical stress lines in the deep posterior stroma (white arrow). These are Vogt striae — caused by mechanical compression/tensile stress on the posterior stroma as the conical protrusion deforms the lamellar architecture. Pathognomonic feature: they disappear transiently with gentle digital pressure on the globe (pressure relieves the stress). Best seen on slit-lamp with narrow beam in direct or retro-illumination.
IMAGE 6 — Keratoconus: Conical Protrusion
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.39D
What this shows: Slit-lamp view of a typical keratoconus cone. The narrow slit beam profile reveals the characteristic conical protrusion of the central/paracentral cornea anteriorly. Thinning is maximal at the apex. The beam shows the uneven, pointed anterior contour against the relatively normal peripheral cornea. The clear nature of the cone (visible iris through it) indicates the stroma has not yet undergone significant scarring.
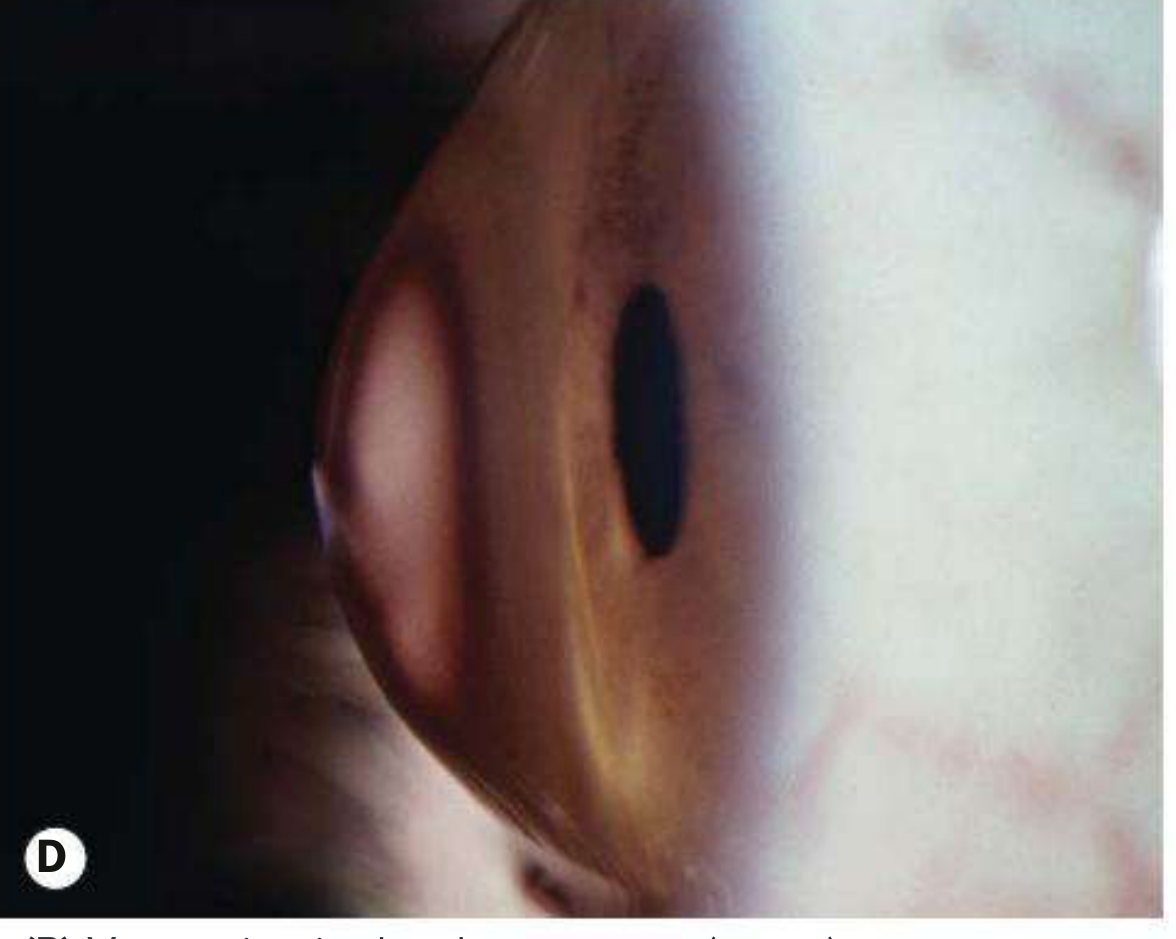
IMAGE 7 — Keratoconus: Munson Sign
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.40A
What this shows: Munson sign — the advanced keratoconus cone physically contacts and deforms the lower eyelid in downgaze, producing a characteristic V-shaped or tent-shaped indentation of the lower lid margin. This sign is visible to the naked eye without instrumentation. It indicates moderate-to-advanced keratoconus. The mechanism: the cone has protruded so far anteriorly that in downgaze it pushes against the lower lid.
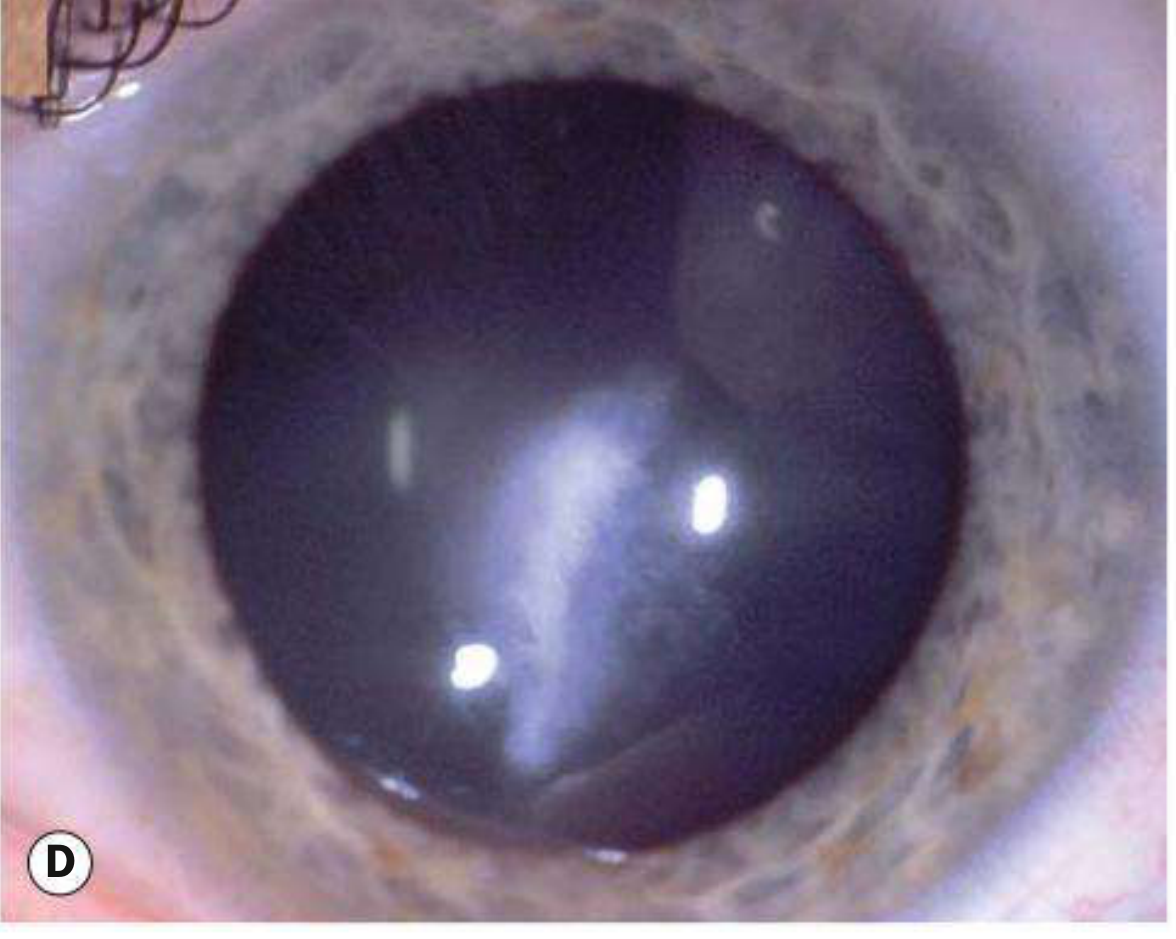
IMAGE 8 — Acute Corneal Hydrops: Late Scarring
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.40D
What this shows: Dense grey-white central corneal scarring following acute hydrops in keratoconus. Acute hydrops occurs when Descemet membrane ruptures at the cone apex → aqueous rushes into stroma → sudden severe pain + white corneal swelling. After resolution (6-10 weeks), fibrous scar tissue replaces the previously oedematous stroma. Note: paradoxically, scar formation may flatten the cone and occasionally improve BCVA temporarily. Tectonic keratoplasty may be required if scar is visually significant and dense.
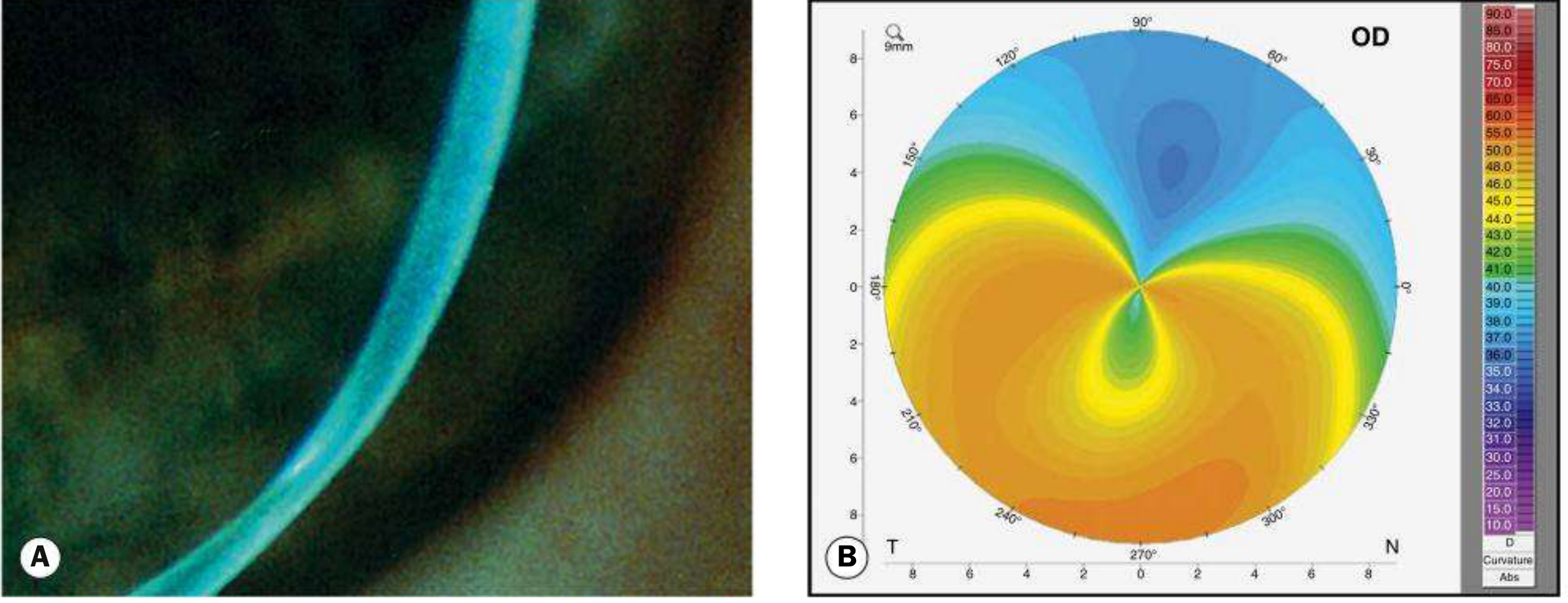
IMAGE 9 — PMD Topography: Butterfly Pattern
Kanski's Clinical Ophthalmology 10th Ed., Fig. 7.43 (A, B)
What this shows: (A) Slit-lamp photo: Pellucid marginal degeneration — the inferior peripheral crescent-shaped thinning zone, ~1 mm from the limbus, 4-8 o'clock. The overlying epithelium is intact (unlike ulcers). (B) Corneal topography: The characteristic "butterfly" or "lobster-claw" pattern — orange/yellow-red = steep zones at the inferior periphery (where ectasia secondary to thinning is maximal); blue = flat superior cornea. This pattern distinguishes PMD from keratoconus: KC has inferiorly displaced cone with conical topography; PMD has crescent inferior thinning with secondary ectasia above and extreme against-the-rule astigmatism.
SECTION 8: MASTER SUMMARY TABLE
The Six Layers at a Glance
| Layer | Thickness | Cell Types / Structure | Key Molecules | Regenerates? | Key Clinical Facts |
|---|
| Epithelium | 50-60 µm | Basal (columnar, mitotic) + Wing (polygonal) + Surface squamous | CK3/K12 (differentiated), MUC1/4/16 (surface), hemidesmosomes (adhesion) | YES — from limbal stem cells | Renews 7-10 days; LSCD → pannus; ABMD → recurrent erosions; stem cells at limbus (p63, ABCG2) |
| Bowman | 8-12 µm | Acellular; randomly arranged thin collagen fibrils | Type I, III, V, VII collagen (smaller diameter, randomly oriented) | NO — replaced by scar | Scars are permanent; target for PTK; absent in most animals |
| Stroma | 450-500 µm | 200-300 collagen lamellae; keratocytes (fibroblasts, neural crest) | Type I collagen (regular lamellae), keratan sulfate (lumican/keratocan), dermatan sulfate (decorin) | Partially (irregular scar — Type III collagen) | 90% of thickness; Maurice lattice theory; wound healing → haze; CXL target; ectasia in KC |
| Dua's layer | 10-15 µm | Acellular; compact Type I collagen lamellae (5-8 layers) | Type I collagen (dense) | Unknown | DALK Big-Bubble planes (Type 1 = ideal; Type 2 = within); natural cleavage zone |
| Descemet | 10-12 µm | Acellular BM; ABZ (in utero, Col VIII, banded) + PNBZ (postnatal, Col IV, non-banded) | Col IV (PNBZ), Col VIII (ABZ), laminin, fibronectin | YES — endothelial cells secrete new PNBZ | Guttata in Fuchs (PNBZ); DMEK graft unit; scrolls endothelium-out; Haab striae |
| Endothelium | ~5 µm (single layer) | ~2,500-3,000 cells/mm²; hexagonal mosaic; metabolically highly active | Na⁺/K⁺-ATPase, AQP-1, CA-II/IV, NBC1/SLC4A4 (HCO₃⁻ pump) | NO (G1 arrest - p27, TGF-β2) | Decompensation <500 cells/mm²; FECD (TCF4/COL8A2); DMEK; ROCK inhibitors enable therapy |
SECTION 9: HIGH-YIELD CLINICAL CORRELATIONS
| Anatomical / Physiological Principle | Clinical Correlate |
|---|
| Epithelium renews from limbal stem cells (centripetal migration) | LSCD → conjunctivalization, pannus, PED; treated with CLET/CLAL |
| Bowman layer does NOT regenerate | Anterior stromal scars are permanent; PTK removes but cannot restore Bowman |
| Stroma = 90%; transparency = uniform collagen + proteoglycans | Any disruption (oedema, scar, dystrophy) → opacity |
| Stroma cannot regenerate — forms scar (Type III collagen) | Post-PRK haze; PTK leaves modified fibrous plane |
| Dua's layer is the natural posterior cleavage plane | DALK Big-Bubble Type 1 = optimal surgical result |
| Descemet membrane regenerates (PNBZ grows throughout life) | DMEK graft viability; spontaneous partial healing of Haab striae |
| Endothelium cannot regenerate (G1 arrest) | Must monitor ECC before all intraocular surgery |
| Endothelial pump requires Na⁺/K⁺-ATPase + carbonic anhydrase | CA inhibitors (dorzolamide/acetazolamide) can worsen marginal endothelium |
| Critical ECC ~500 cells/mm² | Below this = bullous keratopathy; DMEK/DSAEK indicated |
| Cornea is most densely innervated tissue in body | Even small abrasion = intense pain, photophobia, blepharospasm |
| Sub-basal nerve plexus provides trophic support + sensation | Loss (HSV, DM, surgery, CN V damage) → neurotrophic keratopathy (NK) |
| Post-LASIK: SBN plexus severed by flap | Reduced sensation for 6-24 months; dry eye; check IVCM at follow-up |
| Cenegermin (rh-NGF) replaces the trophic factor | FDA/EMA approved treatment for NK Stage II-III |
| Prolate corneal shape (Q ≈ -0.26) minimizes SA | Standard LASIK → oblate → increased SA → halos; asphericity-optimized LASIK compensates |
| Keratometric index (n=1.3375) assumes normal post:ant radius relationship | Post-LASIK: ratio changed → all standard keratometry/IOL formulae underestimate corneal power → use Barrett True-K/Holladay 2/Shammas |
| Maurice lattice depends on regular fibril spacing by KS proteoglycans | Macular CD (CHST6 mutation, no KS) → disrupted spacing → diffuse opacity, no clear zones |
| TCF4 CTG repeat expansion → defective endothelium → excess Col VIII | Fuchs FECD (most common form); cornea guttata on specular microscopy |
Compiled June 2026 | Sources: Kanski's Clinical Ophthalmology 10th Ed. (p. 219-225); Robbins, Cotran & Kumar Pathologic Basis of Disease (Ch. 29); Wheater's Functional Histology (Plates 24.3-24.4); Gray's Anatomy for Students; Krachmer/Mannis/Holland Cornea 3rd Ed. (conceptual framework)