Flow volume loops
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough overview of flow volume loops (FVLs), drawn from multiple authoritative pulmonary textbooks.
Flow Volume Loops
What Is a Flow Volume Loop?
A flow volume loop (FVL) is a graphical representation of airflow (y-axis, in L/s) plotted against lung volume (x-axis, in L) during a forced maximal expiration followed by a forced maximal inspiration. The subject exhales fully from total lung capacity (TLC) to residual volume (RV), then inhales back to TLC. The shape of the loop is the most clinically informative feature.
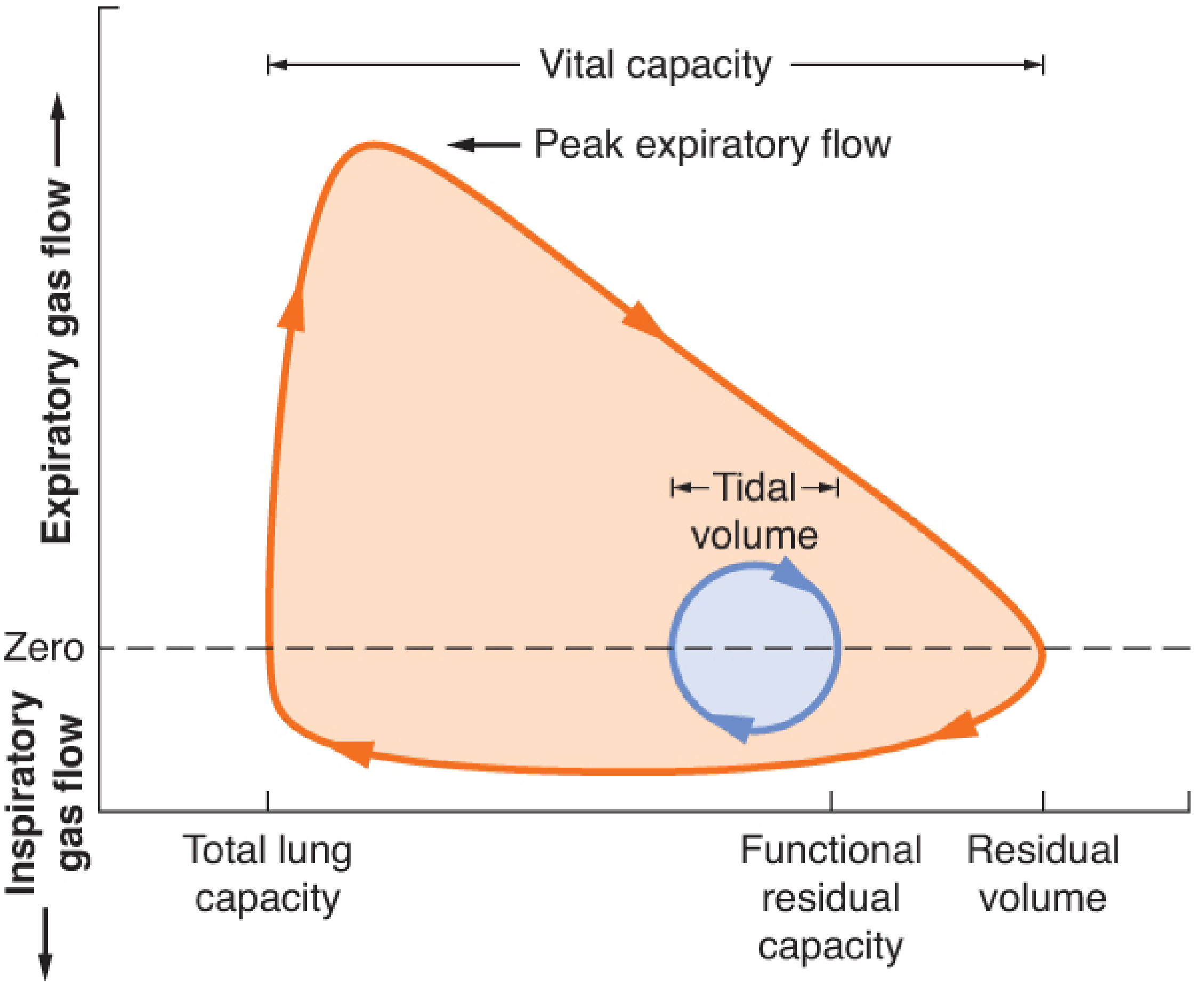
Figure: Normal adult flow-volume loop. Expiratory flow is above the zero line; inspiratory flow is below. Tidal volume is the small circle near functional residual capacity (FRC). - Barash Clinical Anesthesia, p. 1137
Axes and Orientation
| Axis | Represents | Direction |
|---|---|---|
| Y-axis | Airflow (L/s) | Above zero = expiration; below zero = inspiration |
| X-axis | Lung volume (L) | Left = TLC; right = RV |
- The expiratory limb (upper curve): starts at TLC, rises sharply to peak expiratory flow (PEF), then declines linearly toward RV
- The inspiratory limb (lower curve): begins at RV, peak inspiratory flow (PIF) occurs near the midpoint, and returns to TLC
Normal: PEF > PIF, because dynamic compression of intrathoracic airways limits expiratory flow more than inspiratory flow, while the inspiratory portion is entirely effort-dependent.
Effort Dependence
- First 25% of forced expiration (near TLC): effort-dependent - increased effort increases flow
- Remaining 75%: effort-independent - flow is determined by lung elastic recoil and airway mechanics (dynamic compression); more effort does not increase flow
- Entire inspiratory limb: effort-dependent throughout
Normal FVL Characteristics
- Rapid rise to PEF shortly after maximal exhalation begins
- Near-linear decline in expiratory flow from peak to RV
- Smooth, roughly semicircular inspiratory curve
- PIF slightly less than PEF
- FEF50% (mid-expiratory flow) is normally less than FIF50% (mid-inspiratory flow)
Pathological Patterns
1. Obstructive (COPD, Asthma, Emphysema)
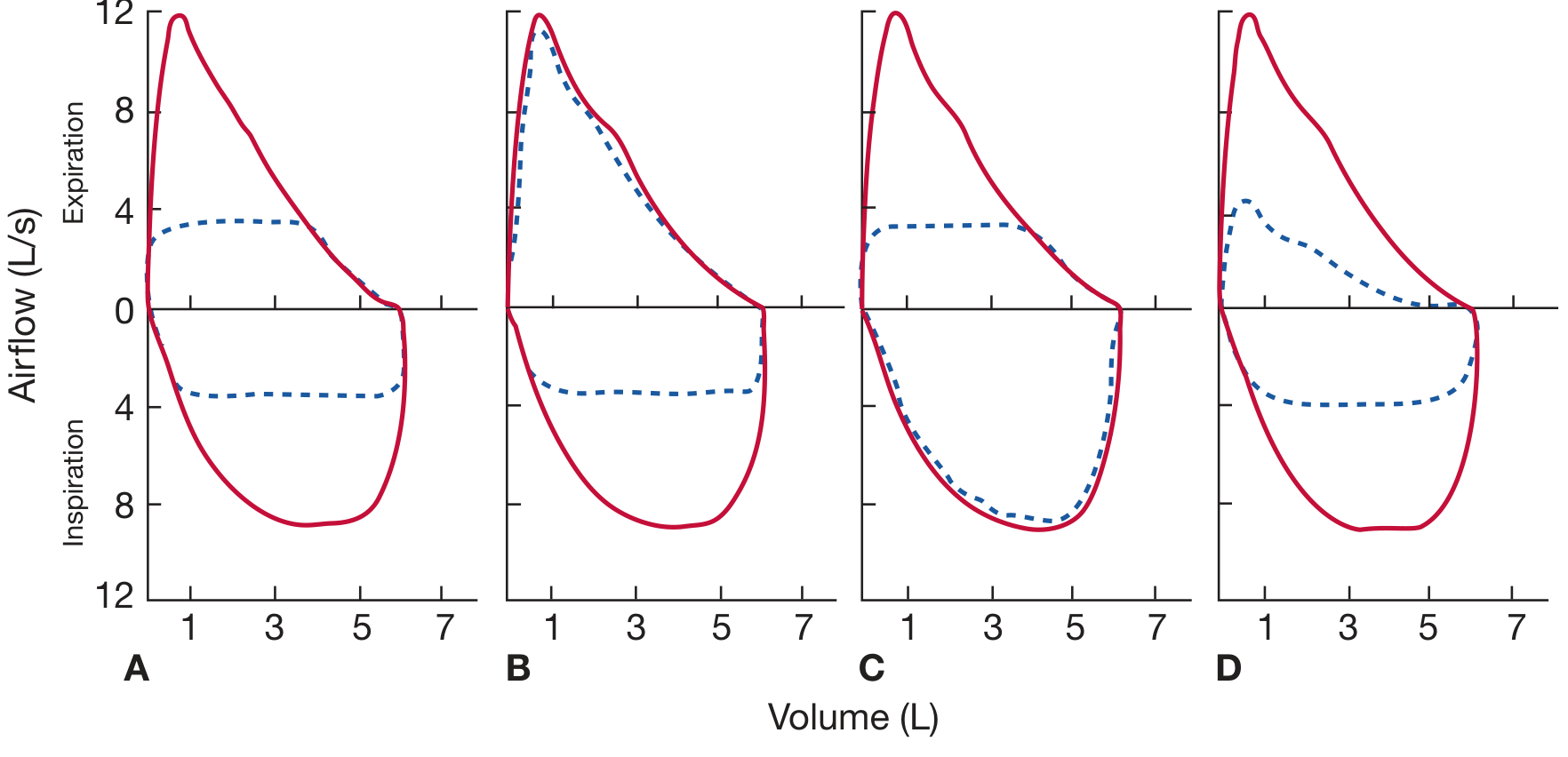
Figure: Schematic flow-volume loops in four pathologic conditions. Red = patient; blue dashed = normal. A: Fixed upper-airway obstruction (both limbs truncated). B: Variable extrathoracic obstruction (inspiratory limb flattened). C: Variable intrathoracic obstruction (expiratory limb flattened). D: COPD - reduced expiratory flow with preserved curve shape/taper. - Fishman's Pulmonary Diseases, p. 605
- Expiratory limb is concave upward (scooped/curvilinear) - this is the hallmark
- Reflects greater flow reduction at low lung volumes vs high lung volumes
- FVC and FEV1 are reduced; FEV1/FVC ratio is decreased
- The loop is shifted to the right (air trapping, increased RV)
- Asthma: loop may normalize post-bronchodilator
- Emphysema: severe scooping, DLCO reduced, TLC increased
2. Restrictive (Interstitial Lung Disease, Chest Wall)
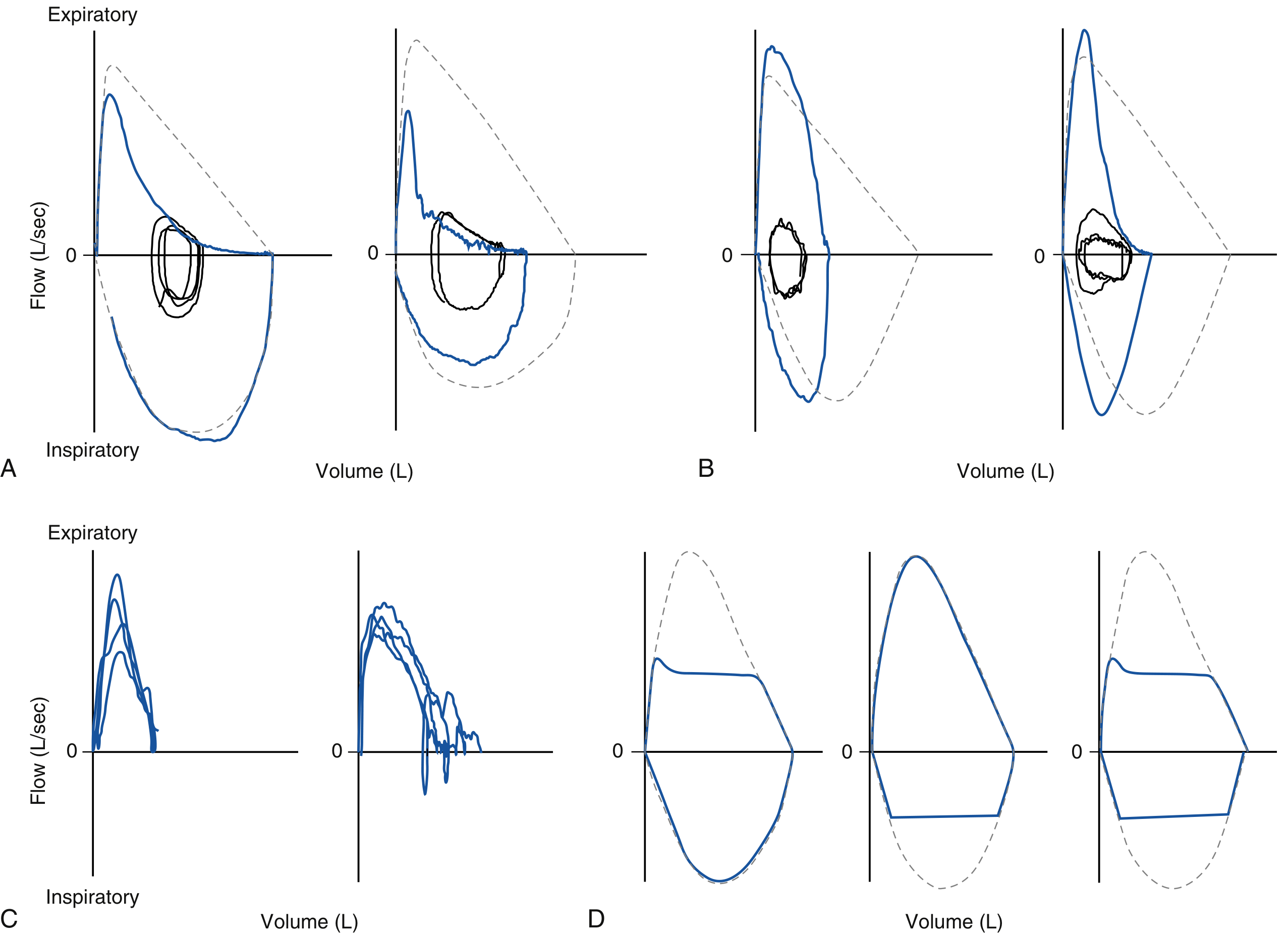
Figure: Real flow-volume curve patterns. A: COPD (concave expiratory limb). B: ILD/restriction (steep, vertically-oriented expiratory limb, reduced VC). C: Poor effort (irregular, non-reproducible). D: Large airway obstruction subtypes. - Murray & Nadel's Respiratory Medicine, p. 763
- Expiratory limb is convex upward (steep, vertically oriented) - increased elastic recoil drives higher peak flows at high volumes
- FVC and FEV1 both reduced proportionally; FEV1/FVC ratio is normal or increased
- Total lung capacity (TLC) is reduced - confirmation requires plethysmography
- Important caveat: spirometry alone identifies restrictive pattern with only ~50% sensitivity; TLC measurement is required for confirmation
3. Upper Airway Obstruction (UAO)
Three subtypes, each with a characteristic loop shape:
| Type | Location | Mechanism | Loop Pattern |
|---|---|---|---|
| Fixed | Either (tracheal scar, stenosis) | Cross-section fixed regardless of breathing phase | Both inspiratory AND expiratory limbs truncated/flattened equally |
| Variable extrathoracic (e.g., vocal cord paralysis, subglottic stenosis) | Above thoracic inlet | Forced inspiration reduces intratracheal pressure below atmospheric → airway collapses | Inspiratory limb flattened; expiratory limb normal |
| Variable intrathoracic (e.g., tracheal tumor, tracheomalacia) | Below thoracic inlet | Forced expiration increases pleural pressure above intratracheal → airway collapses | Expiratory limb flattened; inspiratory limb normal |
Key ratio: FEV1/PEFR > 8 mL/L/min on routine spirometry should prompt careful review of the FVL for UAO.
Distinguishing UAO from COPD: In COPD the expiratory limb is reduced but retains its normal tapering shape (gradual deceleration). In UAO the expiratory limb is flat (uniform flow plateau) throughout expiration - a qualitatively distinct pattern.
FVL in Specific Conditions
| Condition | FEV1 | FVC | FEV1/FVC | DLCO | FVL finding |
|---|---|---|---|---|---|
| Chronic bronchitis | ↓ | ↓ | ↓ | Normal | Abnormal (scooped expiratory) |
| Emphysema | ↓ | ↓ | ↓ | ↓ | Abnormal (scooped, large VC) |
| Asthma | ↓ | ↓ | ↓ | Normal | Abnormal; reverses post-BD |
| ILD (restrictive) | ↓ | ↓ | Normal/↑ | ↓ | Steep/convex expiratory |
| Fixed UAO | ↓ | ↓ | ↓ | Normal | Both limbs truncated |
| Variable extrathoracic | ↓ | ↓ | ↓ | Normal | Inspiratory flattening |
| Variable intrathoracic | ↓ | ↓ | ↓ | Normal | Expiratory flattening |
| Small airway disease | Normal | Normal | Normal | Normal | Normal |
- Fishman's Pulmonary Diseases, Table 31-19
FVL During Exercise
During cardiopulmonary exercise testing (CPET), tidal flow-volume loops (tidal FVLs) are plotted within the maximal flow-volume loop (MFVL) envelope:
- Expiratory flow limitation: tidal loop encroaches on the expiratory limb of the MFVL
- Dynamic hyperinflation: end-expiratory lung volume rises above resting FRC (seen as leftward shift of tidal loop within MFVL)
- Inspiratory muscle limitation: tidal inspiratory flows approach the inspiratory MFVL - indicates near-maximal inspiratory effort
This analysis is particularly useful in COPD, where both flow limitation and dynamic hyperinflation contribute to exertional dyspnea. - Fishman's Pulmonary Diseases, p. 619
Other FVL Findings
- Sawtooth pattern: oscillatory notching on the inspiratory limb (and sometimes expiratory) - associated with obstructive sleep apnea and upper airway instability, or extrapyramidal disease (e.g., Parkinson's)
- Tracheal plateau / vocal cord dysfunction: mid-inspiratory flow plateau suggesting episodic vocal cord adduction
- Suboptimal effort: irregular, slurred curves without repeatability; no consistent peak; diagnose as poor quality
- Negative effort dependence (in severe COPD): tidal expiratory flow at low lung volumes actually exceeds maximal forced flow - the airway collapses more with greater effort, a sign of severe dynamic airway collapse
Clinical Uses
- Diagnosis and classification of obstructive vs. restrictive ventilatory defects
- Detection and characterization of upper airway obstruction (fixed vs. variable, extra vs. intrathoracic)
- Monitoring response to bronchodilators in asthma/COPD
- Preoperative assessment (historically) - though CT/MRI has largely replaced FVL for structural UAO
- Exercise physiology - detection of expiratory flow limitation and dynamic hyperinflation during CPET
- Identifying poor patient effort and technical artifact
Sources: Fishman's Pulmonary Diseases and Disorders (pp. 605, 619) | Murray & Nadel's Textbook of Respiratory Medicine (pp. 707, 761, 763) | Barash Clinical Anesthesia (p. 1137) | Goldman-Cecil Medicine | KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.