Amitriptyline drug detail and tapering
Reading File
Finding Sources
Searching the Web
amitriptyline drug details pharmacology indications tapering protocol 2024
Searching PubMed
amitriptyline tapering discontinuation withdrawal
Reading File
Reading File
Searching PubMed
amitriptyline antidepressant discontinuation withdrawal syndrome
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information from the Maudsley Deprescribing Guidelines and other textbooks. Let me compile a thorough answer.
Amitriptyline - Drug Profile & Tapering Guide
Drug Overview
Class: Tricyclic antidepressant (TCA)
Trade Names: Elavil, Endep
Available Formulations: Tablets (10, 25, 50, 75, 100, 150 mg), sustained-release capsules, oral liquid solution (2 mg/mL)
Mechanism of Action
Amitriptyline inhibits the membrane pump (reuptake transporter) responsible for re-uptake of both serotonin (SERT) and norepinephrine (NET) in adrenergic and serotonergic neurons, thereby potentiating and prolonging neuronal activity. Beyond reuptake inhibition, it has strong binding affinities at:
- Alpha-adrenergic receptors - causes orthostatic hypotension, dizziness
- Histamine H1 receptors - causes sedation, weight gain
- Muscarinic M1 receptors - causes anticholinergic effects
- Sodium channels - membrane-stabilizing/cardiac effects (relevant in toxicity)
Its active metabolite nortriptyline (formed via CYP2C19) also contributes significantly to clinical effect. CYP3A4 and CYP2D6 are also involved in metabolism.
Pharmacokinetics
| Parameter | Value |
|---|---|
| Peak plasma | 1-12 hours |
| Half-life | ~25 hours (range 18-28 h) |
| Volume of distribution | 17.1 ± 2.4 L/kg (high) |
| Metabolism | Hepatic (CYP2C19, CYP3A4, CYP2D6) to nortriptyline + hydroxynortriptyline |
| Excretion | Primarily renal |
| Protein binding | ~95% |
Women tend to have higher plasma levels and lower clearance rates than men. The drug crosses the placental barrier.
FDA-Approved Indication
- Major Depressive Disorder (MDD) in adults - endogenous depression is more likely to be alleviated than other depressive states
Off-Label Uses
- Chronic pain (fibromyalgia, diabetic neuropathy, postherpetic neuralgia)
- Migraine prophylaxis
- Insomnia
- Anxiety / PTSD
- Irritable bowel syndrome (IBS)
- Interstitial cystitis / bladder pain syndrome
- Post-COVID headache
- Sialorrhea (drooling)
In rheumatology, amitriptyline is a first-line pharmacologic treatment for fibromyalgia per AWMF guidelines.
Dosing
| Indication | Starting Dose | Maintenance Dose |
|---|---|---|
| Depression | 25-75 mg/day | 75-150 mg/day (up to 300 mg in inpatients) |
| Chronic pain/neuropathy | 10-25 mg/night | 25-75 mg/night |
| Migraine prophylaxis | 10 mg at bedtime | 10-75 mg |
| Insomnia | 10-25 mg at bedtime | 10-50 mg |
Dosing is typically once at night due to sedative effects (manufacturer recommends twice daily with the larger dose at bedtime).
Adverse Effects
Anticholinergic (most common):
- Dry mouth, constipation, urinary retention, blurred vision
- Confusion, delirium (especially in elderly)
CNS/Histaminergic:
- Sedation, cognitive slowing, weight gain
Cardiovascular:
- Orthostatic hypotension (alpha-1 blockade)
- QTc prolongation, sinus tachycardia
- Can cause fatal arrhythmias in overdose (sodium channel blockade)
Other:
- Sexual dysfunction
- Lowered seizure threshold
- Hyponatraemia (rare, reported in acute withdrawal too)
Contraindications
- Recent (within 14 days) or concurrent MAO inhibitor use - risk of hyperthermic crisis, severe convulsions, death
- Acute myocardial infarction recovery phase
- Prior hypersensitivity to the drug
- Caution in: angle-closure glaucoma, BPH, cardiac arrhythmias, epilepsy, bipolar disorder (may precipitate mania/hypomania), hepatic impairment, elderly patients
Drug Interactions
| Interactant | Effect |
|---|---|
| MAOIs | Potentially fatal - hyperpyrexia, convulsions |
| CYP2D6 inhibitors (fluoxetine, paroxetine) | Increased amitriptyline levels / toxicity |
| CYP3A4 inducers (St. John's Wort) | Decreased amitriptyline levels |
| CNS depressants, alcohol | Additive sedation |
| Anticholinergic drugs, diphenhydramine | Additive anticholinergic effects |
| Cimetidine | Increased TCA levels |
Tapering Protocol (Maudsley Deprescribing Guidelines)
Why Tapering Matters
Amitriptyline is classified as high risk for withdrawal effects. One placebo-controlled study showed that when tapered over 6 months, 80% of patients experienced withdrawal symptoms. The relationship between dose and receptor occupancy is hyperbolic - equal linear dose cuts do NOT produce equal reductions in pharmacological effect. As doses get lower, smaller absolute reductions cause proportionally larger receptor occupancy changes, triggering more severe withdrawal.
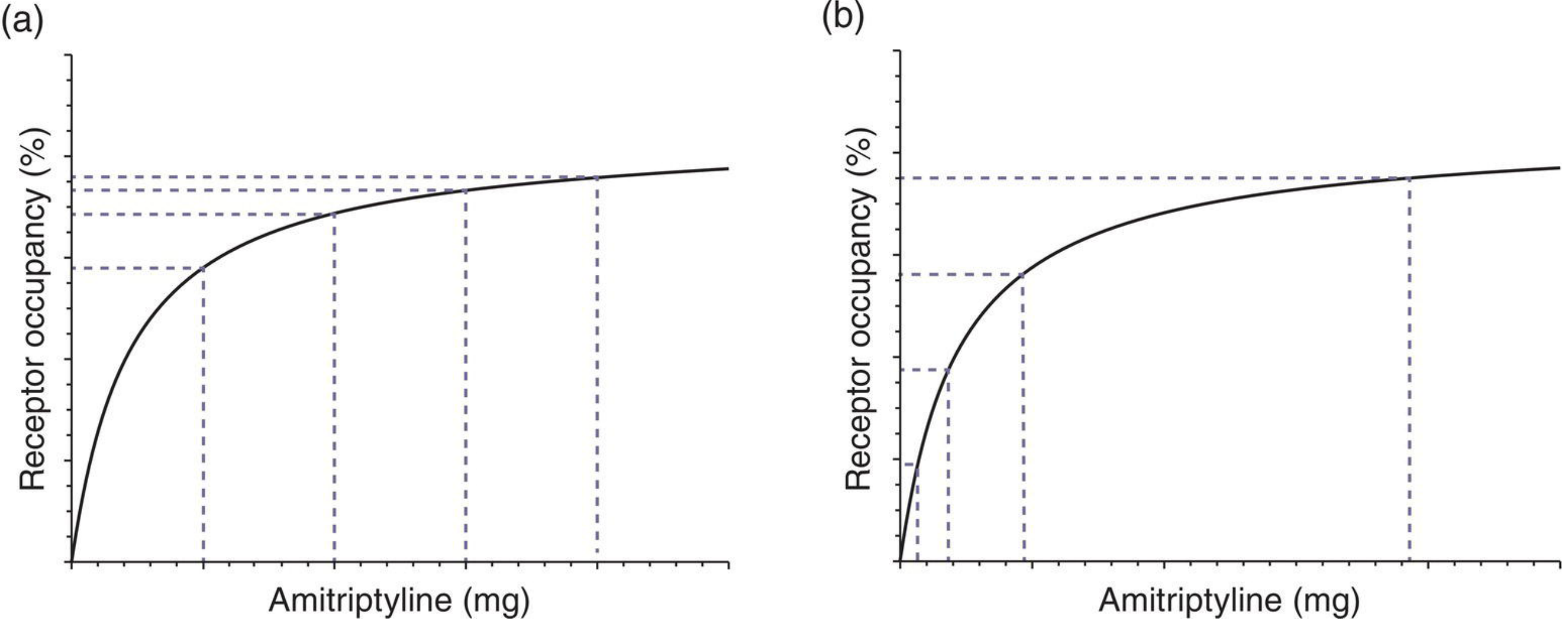
(a) Equal linear dose cuts cause increasingly large drops in receptor occupancy at lower doses.
(b) To produce equal reductions in receptor effect, dose cuts must become smaller and smaller (hyperbolic schedule).
Key principle: every-other-day dosing is NOT recommended for tapering because the 25-hour half-life means significant plasma concentration fluctuations that can provoke withdrawal.
Taper Schedules (from Maudsley Deprescribing Guidelines, starting from 100 mg)
Option A - Faster taper (~20 steps, reductions every 2-4 weeks)
| Step | Dose | Formulation |
|---|---|---|
| 1 | 100 mg | Tablets |
| 2 | 70 mg | Tablets |
| 3 | 50 mg | Tablets |
| 4 | 35 mg | Tablets |
| 5 | 25 mg | Tablets |
| 6 | 17.5 mg | ¾ tablet |
| 7 | 12.5 mg | ½ tablet |
| 8 | 10 mg | Tablet |
| 9 | 7.5 mg | ¾ tablet |
| -- | Switch to 2 mg/mL liquid | -- |
| 10 | 6 mg | 3 mL |
| 11 | 5 mg | 2.5 mL |
| 12 | 4 mg | 2 mL |
| 13 | 3 mg | 1.5 mL |
| 14 | 2.5 mg | 1.25 mL |
| 15 | 2 mg | 1 mL |
| 16 | 1.5 mg | 0.75 mL |
| 17 | 1 mg | 0.5 mL |
| 18 | 0.6 mg | 0.3 mL |
| 19 | 0.3 mg | 0.15 mL |
| 20 | Stop | -- |
Option B - Slower taper (~39 steps, reductions every 2-4 weeks)
This extends the schedule with smaller intermediate steps between each tablet dose, then micro-tapers using the liquid formulation all the way from ~12.5 mg down through 0.25 mg before stopping. This is recommended for patients who:
- Have had previous difficult withdrawal attempts
- Have been on the drug for many years
- Experienced significant symptoms on the faster schedule
Practical Tapering Principles
- Reduce by no more than 10% of the current dose at each step as a general rule (hyperbolic model)
- Allow 2-4 weeks at each dose level before reducing further - symptoms may be delayed
- Switch to liquid formulation once below 10 mg to allow precise micro-dosing
- Slow down or hold the dose if withdrawal symptoms emerge; resume tapering only when stable
- Do not abruptly stop - risk of rebound symptoms, cholinergic rebound (nausea, vomiting, sweating, diarrhea, insomnia), anxiety, and agitation
- The total taper duration for long-term users may span months to over a year
Withdrawal Symptoms to Monitor
- Flu-like symptoms: nausea, vomiting, diarrhea, sweating, myalgia
- Sleep disturbance, vivid dreams
- Anxiety, agitation, irritability
- Headache
- "Electric shock" sensations (less common with TCAs than SSRIs)
- Relapse of original condition (must be distinguished from withdrawal)
- Rare: hyponatraemia, delirium (more common with abrupt stopping in elderly)
Sources:
- The Maudsley Deprescribing Guidelines - Amitriptyline section (pp. 323-328)
- Bradley and Daroff's Neurology in Clinical Practice - Antidepressants for pain management
- Harrison's Principles of Internal Medicine, 22E
- StatPearls (NIH/NCBI) - Amitriptyline
- FDA prescribing information (2025)
This is a shared conversation. Sign in to Orris to start your own chat.