Role of Vitamin d in human body
Reading File
Finding Sources
Searching PubMed
"vitamin D"[MeSH Terms] AND "physiology"[MeSH Terms]
Searching the Web
role of vitamin D in human body physiology functions 2025
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have excellent, comprehensive information from multiple authoritative textbooks. Let me compile a thorough answer.
Role of Vitamin D in the Human Body
What Is Vitamin D?
Vitamin D is a fat-soluble secosteroid hormone — unique because it can be entirely synthesized endogenously and acts through a specific nuclear receptor, giving it properties of both a vitamin and a hormone. Two biologically important forms exist:
- Vitamin D₃ (cholecalciferol) — from skin synthesis and animal dietary sources (fatty fish, fish oils, egg yolks)
- Vitamin D₂ (ergocalciferol) — from plant sources (fungi, yeasts)
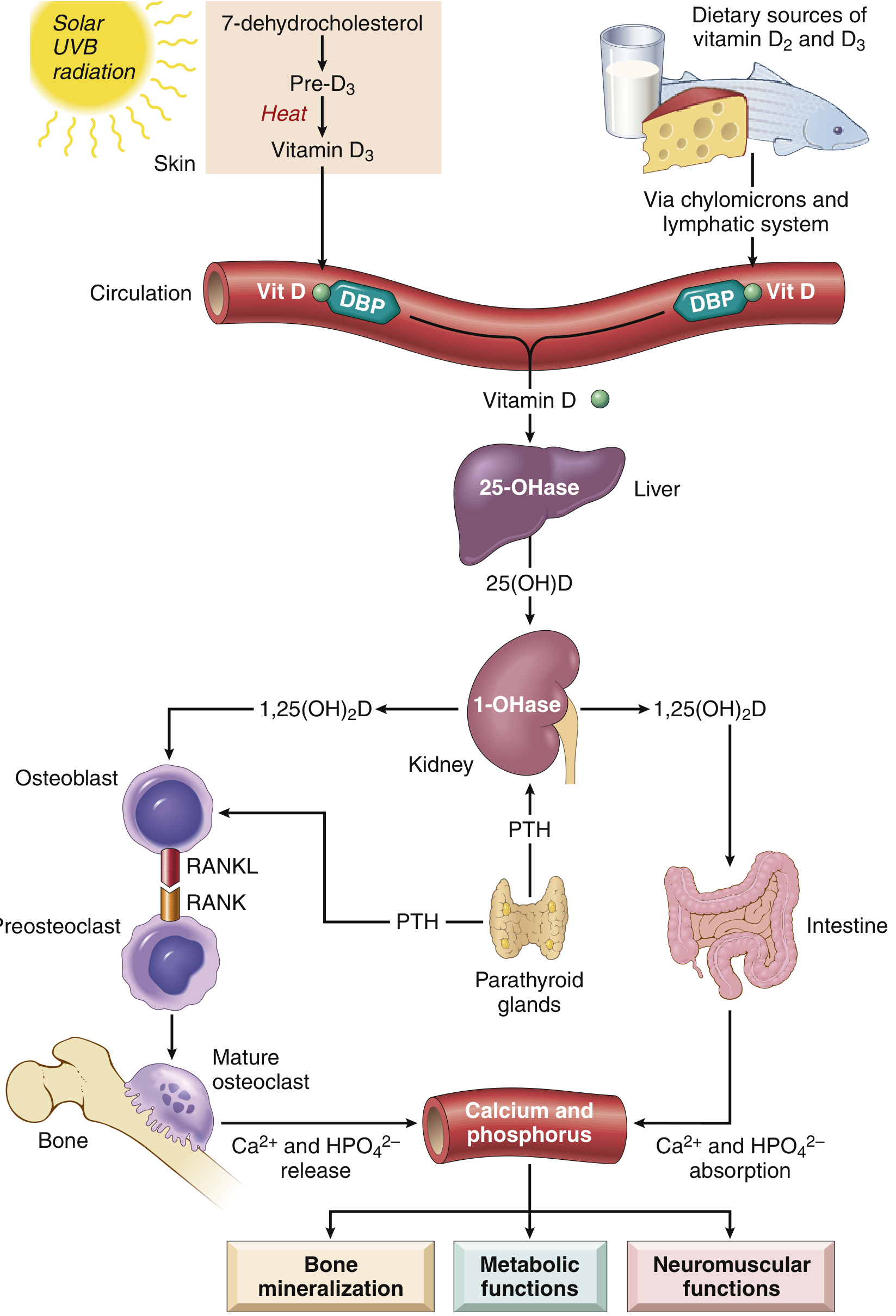
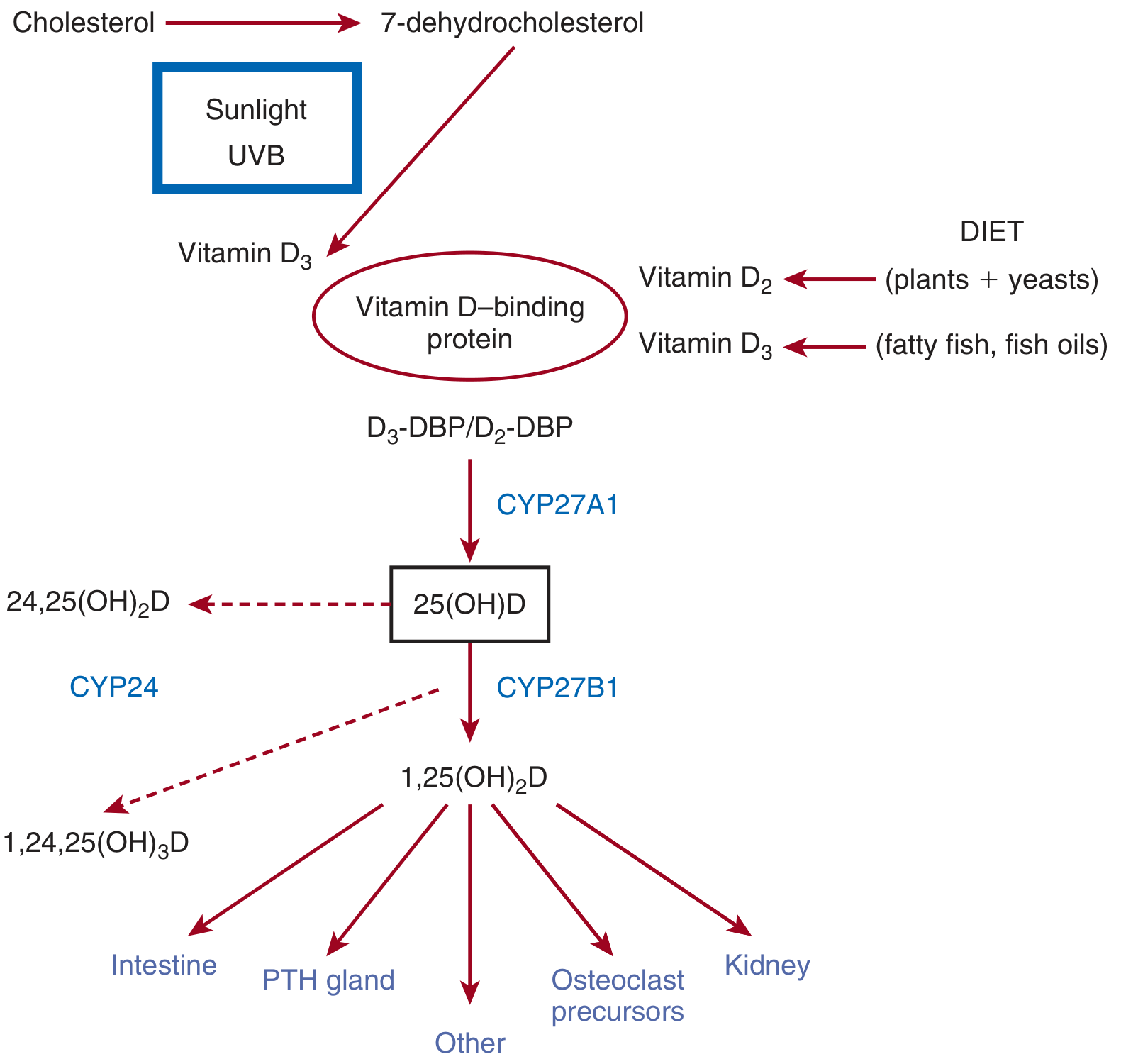
Synthesis & Metabolism
The activation of vitamin D follows a precise two-step hydroxylation pathway:
| Step | Location | Enzyme | Product |
|---|---|---|---|
| UV-B irradiation of 7-dehydrocholesterol | Skin | Photochemical | Vitamin D₃ |
| First hydroxylation | Liver | CYP27A1 (25-hydroxylase) | 25(OH)D (calcidiol — storage form, measured clinically) |
| Second hydroxylation | Kidney | CYP27B1 (1α-hydroxylase) | 1,25(OH)₂D (calcitriol — active form) |
| Inactivation | Kidney/tissues | CYP24A1 (24-hydroxylase) | 24,25(OH)₂D (inactive) |
Key regulation points:
- Under normal sun exposure, ~90% of vitamin D is endogenously derived; melanin in darker skin tones reduces UV-light penetration and lowers cutaneous synthesis
- PTH stimulates 1α-hydroxylase (renal activation) in response to hypocalcemia
- Hypophosphatemia directly activates 1α-hydroxylase
- FGF-23 (produced by osteocytes) inhibits CYP27B1 and activates CYP24A1, creating a feedback loop that limits excess calcitriol
- Calcitriol downregulates its own synthesis via negative feedback on 1α-hydroxylase
- Both 25(OH)D and calcitriol are transported in blood bound to vitamin D-binding protein (DBP), a 58-kDa α₁-globulin synthesized in the liver
Core Functions
1. Calcium & Phosphorus Homeostasis (Primary Role)
The most critical function of vitamin D is maintaining adequate plasma Ca²⁺ and phosphate levels for bone mineralization, metabolic functions, and neuromuscular transmission. Calcitriol [1,25(OH)₂D] acts on three main organs:
Intestine:
- Stimulates intestinal absorption of dietary calcium by upregulating calcium transport proteins in enterocytes
- Increases phosphate absorption
Kidney (Distal Tubules):
- Stimulates calcium reabsorption by upregulating epithelial calcium channels, calbindin (intracellular calcium transporter), and plasma membrane calcium pump
- Reduces urinary calcium losses
Bone:
- Required for mineralization of osteoid matrix and epiphyseal cartilage during formation of flat and long bones
- Upregulates RANKL expression on osteoblasts, activating RANK on osteoclast precursors → osteoclast differentiation and bone resorption to mobilize Ca²⁺ when needed
- Works synergistically with PTH in calcium mobilization
Parathyroid Glands:
- High 1,25(OH)₂D concentrations suppress PTH gene transcription by chief cells — a key negative feedback mechanism
2. Mechanism of Action (Genomic Signaling)
Like steroid hormones, 1,25(OH)₂D binds to the Vitamin D Receptor (VDR) — a high-affinity nuclear receptor present in most nucleated cells of the body. Upon ligand binding:
- VDR translocates to the nucleus
- Heterodimerizes with the Retinoid X Receptor (RXR)
- The complex binds Vitamin D Response Elements (VDREs) in DNA
- Recruits transcription co-activators/co-repressors → modulates gene expression
This genomic pathway explains vitamin D's wide-reaching effects across multiple organ systems.
3. Bone Health
| Condition | Age Group | Mechanism |
|---|---|---|
| Rickets | Children (open epiphyses) | Defective mineralization → unmineralized osteoid → bowing of long bones |
| Osteomalacia | Adults | Same histology; no bowing but decreased bone strength, fracture risk ↑ |
| Osteoporosis | Elderly | Chronic deficiency → secondary hyperparathyroidism → ongoing bone resorption |
4. Immune System Regulation
VDR is expressed on immune cells including T cells, B cells, macrophages, and dendritic cells. Active vitamin D:
- Modulates innate and adaptive immune responses
- Has anti-inflammatory effects
- Plays a role in slowing autoimmunity
- Regulates the renin-angiotensin system, helping prevent hypertension
5. Neuromuscular Function
Adequate vitamin D maintains the correct concentration of ionized calcium in extracellular fluid. Deficiency → drop in Ca²⁺ → continuous excitation of nerves and muscles (tetany):
- Sensory nerves: numbness, tingling, burning
- Motor nerves: spontaneous muscle contractions (carpopedal spasm)
6. Other Emerging Roles
Vitamin D receptors are found in virtually every tissue, and research continues to establish links with:
- Cardiovascular health — regulation of renin-angiotensin system, myocardial function
- Cancer prevention — cell proliferation and differentiation regulation
- Metabolic diseases — insulin secretion and glucose metabolism
- Skin — regulation of keratinocyte differentiation and proliferation
Vitamin D Deficiency
Causes:
- Insufficient sun exposure (elderly, institutionalized, darkly pigmented skin)
- Dietary insufficiency
- Fat malabsorption (Crohn's disease, celiac, cystic fibrosis)
- Chronic kidney disease (impaired 1α-hydroxylase activity)
- Chronic liver disease (impaired 25-hydroxylation)
- Genetic 1α-hydroxylase deficiency (vitamin D-dependent rickets — autosomal recessive)
Clinical features:
- Children: Rickets (bowed legs, frontal bossing, rachitic rosary, delayed dentition)
- Adults: Osteomalacia (bone pain, fragility fractures, proximal myopathy)
- Hypocalcemia → secondary hyperparathyroidism → further bone resorption
- Tetany (in severe hypocalcemia)
Laboratory:
- Serum 25(OH)D is the clinical marker of vitamin D status (not 1,25(OH)₂D, which may be normal or elevated due to secondary hyperparathyroidism)
- Hypocalcemia, hypophosphatemia, elevated ALP and PTH
Dietary Sources
| Source | Form |
|---|---|
| Fatty fish (salmon, tuna, mackerel) | D₃ |
| Fish liver oils | D₃ |
| Egg yolks, beef liver | D₃ |
| Fortified milk, cereals | D₂ or D₃ |
| Mushrooms (UV-exposed) | D₂ |
| Sunlight (UVB, 290–315 nm) | D₃ (skin synthesis) |
Summary
Vitamin D is far more than a bone vitamin. As a pleiotropic hormone, it regulates calcium/phosphorus metabolism, bone integrity, immune function, neuromuscular transmission, and gene expression across virtually every tissue via its nuclear receptor. Its unique two-step activation (liver → kidney) makes it vulnerable to disruption at multiple points, with deficiency producing consequences ranging from rickets in children to osteomalacia, fractures, and immune dysregulation in adults.
Sources:
- Robbins & Kumar Basic Pathology, pp. 293–296
- Medical Physiology (Boron & Boulpaep), p. 1558
- Brenner and Rector's The Kidney, pp. 2393–2396
- Recent systematic review supporting Endocrine Society guidelines: Shah VP et al., J Clin Endocrinol Metab, 2024 (PMID: 38828942)
This is a shared conversation. Sign in to Orris to start your own chat.