Speed test shoulder explain everything in detail with appropriate illustrative images and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
Speed's test shoulder bicipital tendinitis examination
Searching Images
shoulder anatomy bicipital groove long head biceps tendon
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive textbook content, clinical photos, anatomy diagrams, and MRI images. Let me compile the full detailed answer.
Speed's Test of the Shoulder — Complete Guide
1. What Is Speed's Test?
Speed's test (also called the biceps resistance test or forearm supination test) is a clinical provocative examination maneuver used to detect pathology of the long head of the biceps tendon (LHBT) — specifically bicipital tendinitis/tendinopathy and superior labral (SLAP) tears. It was originally described to reproduce pain localized to the anterior shoulder at the bicipital groove.
2. Relevant Anatomy
To understand why the test works, you need to understand the anatomy of the long head of the biceps.
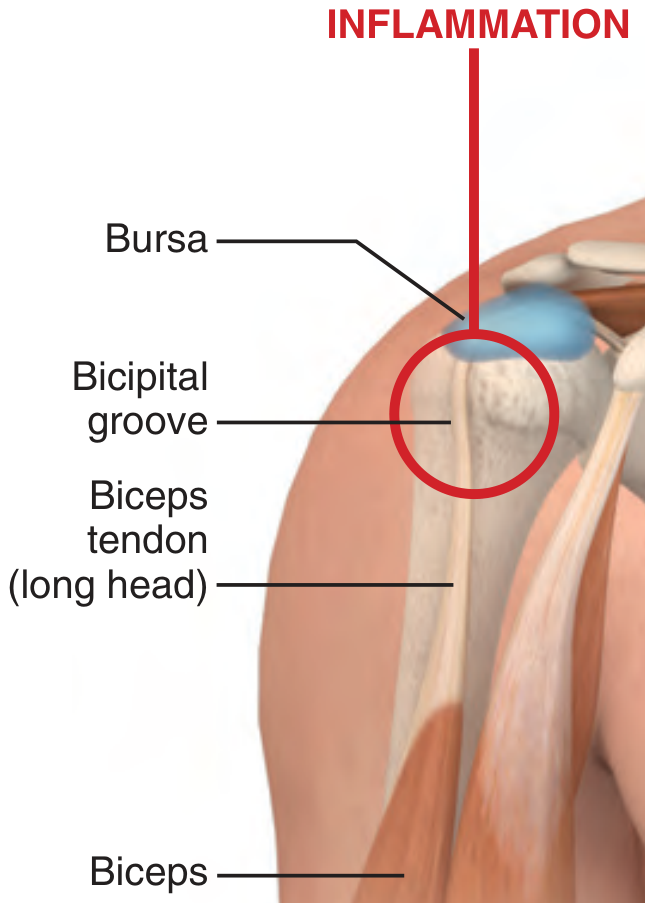
Anatomy of the anterior shoulder: the long head of the biceps tendon runs through the bicipital (intertubercular) groove, covered by a synovial sheath and held in place by the transverse humeral and coracohumeral ligaments. The subacromial bursa lies just above.
Key anatomical facts:
- The long head of biceps originates from the supraglenoid tubercle and glenoid labrum, passing over the humeral head as an intra-articular but extrasynovial structure
- It then descends through the bicipital groove (intertubercular sulcus) between the greater and lesser tuberosities
- It is stabilized in the groove by the coracohumeral ligament and transverse humeral ligament
- The LHBT is a shoulder stabilizer and serves as the primary supinator of the forearm and a flexor of the elbow
- The tendon travels within a synovial sheath that communicates with the glenohumeral joint — making it susceptible to both local and intra-articular inflammation
The bicipital groove can be palpated with the elbow at 90° flexion and the arm internally/externally rotated.
3. How to Perform Speed's Test
Patient Position
- Patient is standing or seated
- The involved arm is at the side
Step-by-Step Technique
| Step | Action |
|---|---|
| 1 | Extend the patient's elbow fully |
| 2 | Supinate the forearm (palm facing upward) |
| 3 | Flex the shoulder to 60–90° of forward flexion |
| 4 | Ask the patient to resist downward force applied by the examiner at the wrist/distal forearm |
| 5 | Observe for pain at the bicipital groove (anterior shoulder) |
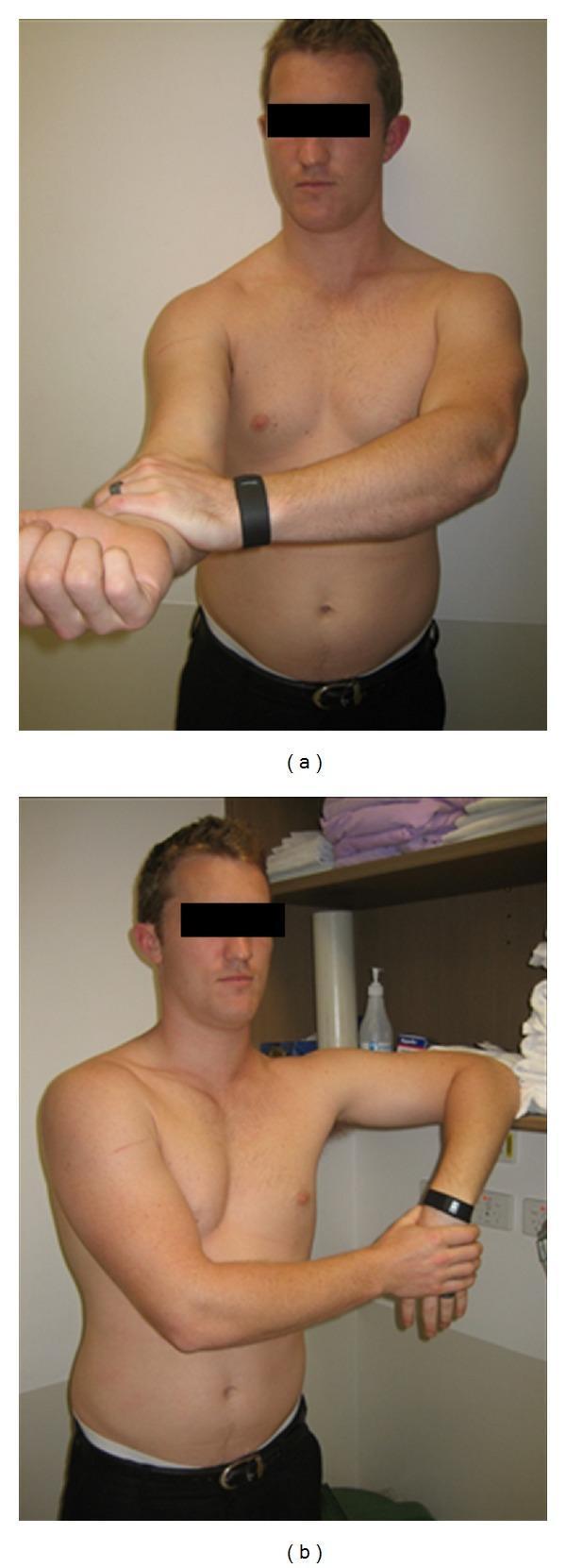
Clinical photograph: (a) Speed's test — the arm is forward-flexed to ~90° with elbow fully extended and forearm supinated (palm up). The examiner applies downward resistance at the wrist. A positive test reproduces pain at the anterior shoulder/bicipital groove.
Positive Test
Pain localized to the bicipital groove = positive Speed's test → suggests bicipital tendinopathy or SLAP lesion.
⚠️ Pain over the superior shoulder or AC joint instead of the bicipital groove suggests a different diagnosis (e.g., AC joint pathology).
4. Mechanism — Why the Test Stresses the LHBT
The combination of:
- Full elbow extension — maximally lengthens and tensions the biceps muscle-tendon unit
- Forearm supination — supination is the primary action of the long head of biceps; supinating while loaded engages the LHBT maximally
- Shoulder forward flexion against resistance — creates an anterior shear force at the glenohumeral joint, directly stressing the LHBT origin at the supraglenoid tubercle and the tendon traversing the bicipital groove
This combination places maximum tensile load on the LHBT and reproduces pain when the tendon is inflamed, torn, or pathologically loaded.
5. Diagnostic Accuracy
| Parameter | Value |
|---|---|
| Sensitivity | 60–87% |
| Specificity | 33–80% |
| Positive Likelihood Ratio | ~2.77 |
From Tintinalli's Emergency Medicine: "The Speed's test appears to have a sensitivity of 60% to 87% and a specificity of 80% for tear of the long head of the biceps, with a positive likelihood ratio of 2.77."
From Rosen's Emergency Medicine: Meta-analyses suggest Speed's test is more sensitive (61–83%) for bicipital tendinopathy, with specificity of 33–71%.
Important caveat: The specificity of Speed's test is limited in the presence of concomitant impingement syndrome and rotator cuff disease — which is common in clinical practice. The test is best interpreted alongside other clinical findings. — Rosen's Emergency Medicine
6. What Speed's Test Diagnoses
Primary diagnosis: Bicipital Tendinopathy
This includes:
- Bicipital tendinitis — inflammation of the LHBT and/or its synovial sheath (tenosynovitis), more common in younger patients with repetitive overhead activities
- Bicipital tendinosis — collagen degenerative changes, more common in older patients
- LHBT partial or complete tear — usually proximal; preceded by age-related microtrauma
Classic clinical picture of bicipital tendinopathy:
- Middle-aged patient with repetitive overhead occupation/sport
- Anterior shoulder pain along the bicipital groove
- Pain worse at night, with external rotation, overhead activities
- Tenderness on palpation of the bicipital groove at 10° internal rotation
Secondary: SLAP Tear (Superior Labral Tear Anterior to Posterior)
Speed's test may also be positive in SLAP lesions because the LHBT originates at the superior labrum — labral tears stress the tendon anchor. However, for suspected SLAP tears, the O'Brien (active compression) test has higher specificity (85–98%).
7. Imaging Correlation
MRI findings in LHBT pathology
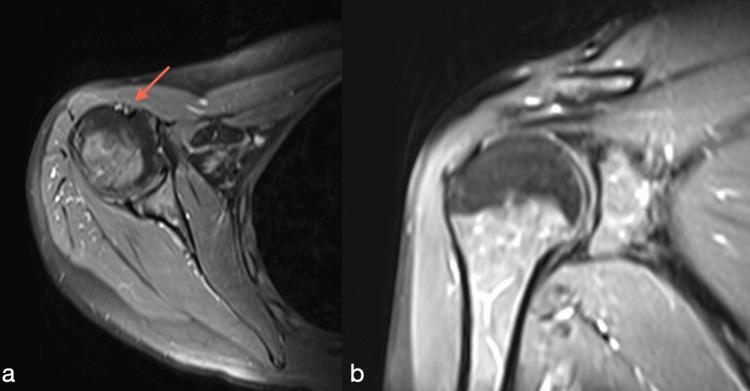
MRI shoulder: (a) Axial view — red arrow points to the LHBT in the bicipital groove showing increased signal intensity and thickening, consistent with proximal biceps tendinopathy. (b) Coronal view — normal-appearing rotator cuff, illustrating isolated biceps pathology.
Preferred imaging:
- Ultrasound — excellent for complete rupture, subluxation, dislocation; less sensitive for partial tears; also guides injection
- MRI — preferred for labral (SLAP) evaluation and full characterization of tendon pathology
8. Companion Tests — The Full Bicipital/Shoulder Examination
Speed's test is not used in isolation. The complete shoulder physical exam for bicipital/labral pathology includes:
Yergason's Test
- Technique: Elbow flexed at 90°, arm adducted against body, patient supinates the forearm against the examiner's resistance
- Positive: Pain or painful pop at the bicipital groove
- Sensitivity: ~50% / Specificity: 83% / PLR: 2.20
- Target: Bicipital tendinopathy, biceps tendon stability in the groove
O'Brien (Active Compression) Test
- Technique: Shoulder flexed 90°, adducted 10–15°, internally rotated (thumb down) → examiner applies downward force; repeated with full supination
- Positive: Pain on first maneuver relieved by second → SLAP lesion
- Sensitivity: 60–100% / Specificity: 85–98%
- Target: SLAP lesions, AC joint pathology
Uppercut Test
- Technique: Shoulder neutral, elbow at 90°, forearm supinated (fist formed) — patient performs a resisted "uppercut" punch against examiner's hand
- Positive: Pain or painful pop at anterior shoulder
- PLR: 3.38 (most favorable for biceps tendinopathy diagnosis)
- When combined with ultrasound: 97% sensitivity, up to 100% specificity
Neer Impingement Sign
- Passive forward flexion >90° → pain = subacromial impingement
Hawkins-Kennedy Test
- Shoulder at 90° flexion + internal rotation → pain = impingement
Drop-Arm Test
- Inability to maintain arm in forward flexion after release = supraspinatus tear
The full table of shoulder examination tests from Miller's Review of Orthopaedics is organized as follows:
| Category | Test | Technique | Significance |
|---|---|---|---|
| Impingement/Rotator Cuff | Hawkins test | Passive FF 90° + IR | Impingement syndrome |
| Impingement/Rotator Cuff | Jobe (empty can) test | Resisted pronation/FF 90° | Supraspinatus lesion |
| Impingement/Rotator Cuff | Drop-arm test | Release from FF | Supraspinatus lesion |
| Instability | Apprehension test | Supine abduction 90° + ER | Anterior instability |
| Instability | Relocation test | Apprehension + posterior force | Anterior instability |
| Instability | Sulcus sign | Inferior force, arm at side | Inferior instability/laxity |
| Labrum/Biceps | O'Brien test | 90° FF, 10° adduct, pronation | SLAP / AC joint |
| Labrum/Biceps | Speed's test | Resisted FF, elbow extended, supinated | Biceps tendon tear/tendinitis |
| Subscapularis | Lift-off test | Arm in IR behind back | Subscapularis tear |
| Subscapularis | Bear-hug test | Hand on opposite shoulder, examiner lifts | Subscapularis tear |
9. Clinical Conditions Diagnosed by Speed's Test
Bicipital Tendinitis
- Mechanism: Repetitive overhead use → microtrauma → synovial sheath inflammation
- Risk factors: Swimmers, weightlifters, overhead laborers; age >40 for tendinosis
- Associated with: Subacromial impingement, rotator cuff disease (rarely isolated)
- Management: Rest, NSAIDS, ice; ultrasound-guided corticosteroid injection (caution — direct tendon injection risks rupture); surgery for refractory cases
Biceps Tendon Rupture
- Proximal rupture (at bicipital groove/supraglenoid tubercle): most common; often spontaneous in older patients
- Classic sign: "Popeye deformity" — distal muscle belly bunches due to proximal tendon release
- Speed's test may be negative after complete rupture (nothing to stress)
- Supination is weakened; elbow flexion is relatively preserved (short head and brachialis intact)
SLAP Lesion
- Superior labral tear from anterior to posterior
- Associated with repetitive overhead (throwing athletes, swimmers)
- Speed's test sensitivity for SLAP: moderate; O'Brien test preferred
10. Differential Diagnosis of Anterior Shoulder Pain
When Speed's test is positive, consider:
| Diagnosis | Key Distinguishing Feature |
|---|---|
| Bicipital tendinopathy | Groove tenderness, positive Yergason's |
| Proximal biceps tear | Popeye deformity, weak supination |
| Rotator cuff tear | Drop-arm test, weakness in abduction |
| SLAP lesion | O'Brien test positive, overhead athletes |
| Subluxing biceps tendon | Painful pop with rotation, medial displacement |
| Subacromial bursitis | Diffuse subacromial tenderness, impingement tests |
| GH/AC osteoarthritis | Joint-line tenderness, radiograph changes |
| Adhesive capsulitis | Global restriction of ROM (all planes) |
11. Summary
| Feature | Detail |
|---|---|
| Full name | Speed's test / Biceps resistance test |
| Target structure | Long head of biceps tendon, superior labrum |
| Patient position | Shoulder flexed 60–90°, elbow extended, forearm supinated |
| Examiner action | Resists shoulder forward flexion (downward force at wrist) |
| Positive finding | Pain at bicipital groove |
| Sensitivity | 60–87% |
| Specificity | 33–80% |
| PLR | ~2.77 |
| Primary diagnosis | Bicipital tendinopathy (tendinitis/tendinosis/tear) |
| Secondary diagnosis | SLAP tear |
| Best companion test | Uppercut test (PLR 3.38) + US for biceps; O'Brien test for SLAP |
| Best imaging | Ultrasound (tendon); MRI (labrum + tendon) |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter on Shoulder
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapters 52 & 103
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 52
- Miller's Review of Orthopaedics, 9th Edition, Table 4.7
Cubitus varus deformity causes etiology pathology biomechanics signs and symptoms classification and investigations and evaluation treatment explain in detail with appropriate images and illustration
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
cubitus varus deformity gunstock elbow child supracondylar fracture
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Cubitus Varus Deformity — Comprehensive Guide
1. Definition & Overview
Cubitus varus (also called the "gunstock deformity") is an angular deformity of the elbow in which the carrying angle is reduced below normal, reversed, or negative — meaning the forearm deviates medially (inward/varus) relative to the long axis of the arm when the elbow is in full extension and the forearm is supinated.
Normal carrying angle:
- Males: 5–10°
- Females: 10–15°
- The angle normally allows the forearm to clear the hip when carrying objects — hence the name
In cubitus varus, this physiological valgus angulation is abolished or replaced by a varus (inward) tilt. The deformity is most commonly seen in children as a complication of malunited supracondylar fractures of the humerus.
2. Normal Elbow Anatomy & Carrying Angle
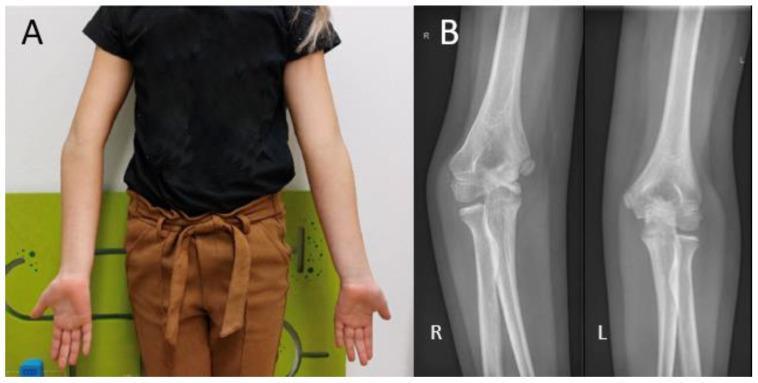
Panel A: Clinical photo — asymmetric carrying angles. Right arm shows cubitus varus (forearm deviated medially). Left arm shows normal valgus alignment. Panel B: AP radiographs — the right elbow (R) shows distal humeral malalignment with decreased Baumann's angle; the left (L) is normal.
The carrying angle is measured with the patient in the anatomical position — elbow fully extended, forearm supinated. The angle is formed between the long axis of the humerus and the long axis of the forearm. This angle:
- Disappears on full pronation
- Disappears on full flexion of the elbow
- Must be compared bilaterally
3. Etiology & Causes
Primary (Most Common) Cause
Malunited Supracondylar Fracture of the Humerus
- Overwhelmingly the most common cause in children (peak age 5–8 years)
- Accounts for >95% of all cases of cubitus varus
- Results from malunion (not growth arrest — this is a critical distinction)
- Posteromedial angulation of the distal fragment leads to varus malalignment on healing
- The Gartland Type III fracture (completely displaced, posteromedial rotation of distal fragment) carries the highest malunion risk
From Miller's Review of Orthopaedics: "Cubitus varus is typically the result of malunion, not growth arrest. It results in a gunstock deformity associated with poor cosmesis but does not generally affect function."
Other Causes (Less Common)
| Cause | Mechanism |
|---|---|
| Lateral condyle fracture malunion | Disrupts lateral physis → varus growth |
| Medial epicondyle fracture | Disrupts medial growth → lateral growth dominant → varus |
| Distal humeral physeal separation | Especially in children <6 years; frequently mistaken for dislocation |
| Growth plate injury (physeal arrest) | Asymmetric growth; lateral physeal damage → relative varus |
| Congenital causes | Rare — bony dysplasias |
| Rickets / metabolic bone disease | Varus bowing at multiple sites |
| Osteomyelitis of distal humerus | Septic destruction of lateral physis |
4. Pathology & Pathoanatomy
The deformity arises primarily at the distal humerus. In malunited supracondylar fractures:
- The distal fragment undergoes posteromedial rotation during displacement
- If inadequately reduced or re-displaced in a cast, the fragment heals in this malrotated position
- The result is medial tilting of the articular surface → varus carrying angle
- Internal rotation component is frequently present but often underappreciated clinically
- The distal humerus shows a "tilted" articular surface — the medial column is relatively lower than the lateral column
Key pathological components of cubitus varus:
- Varus angulation (primary) — decreased carrying angle
- Internal rotation (secondary, often overlooked)
- Hyperextension deformity (may coexist)
- Lateral condyle prominence — the lateral epicondyle becomes more prominent due to the angulation, creating the characteristic "gunstock" silhouette
The term "gunstock deformity" comes from the visual resemblance of the arm to an old musket gunstock — the upper arm and forearm form a shape similar to the stock and barrel of a rifle.
5. Biomechanics
Altered Biomechanics in Cubitus Varus
| Parameter | Normal | Cubitus Varus |
|---|---|---|
| Carrying angle | +10–15° (valgus) | Neutral, 0°, or negative (varus) |
| Valgus stress at medial elbow | Normal | Reduced / reversed |
| Lateral compartment loading | Normal | Increased |
| Medial ulnar collateral ligament | Normal tension | Reduced tension (relative laxity) |
| Posterolateral rotatory stress | Normal | Increased — predisposes to PLRI |
Important Biomechanical Consequences:
-
Lateral compartment overloading — the medially angulated forearm transmits greater compressive force to the radiocapitellar (lateral) compartment during axial loading
-
Posterolateral rotatory instability (PLRI) — the malaligned distal humerus alters the course of the lateral collateral ligament complex. Over time, the LUCL (lateral ulnar collateral ligament) is stretched. This is the mechanism for late-onset elbow instability — a recognized late complication of untreated cubitus varus in adults
-
Valgus laxity of the medial side — the medial ulnar collateral ligament operates at a lower tension than normal, but the medial side is paradoxically less symptomatic than the lateral overloaded side
-
Snapping/subluxation of the triceps — the medial head of triceps may sublux over the medial epicondyle due to altered joint alignment, causing pain and a snapping sensation (another late complication)
-
Tardy ulnar nerve palsy (less common than in cubitus valgus) — but documented in cases where the deformity alters the cubital tunnel geometry
6. Signs & Symptoms
Clinical Presentation
In Children (Shortly After Fracture Healing)
- Cosmetic complaint is the dominant issue
- Medial deviation of the forearm when the arm is extended
- The deformity is often not noticed initially because the elbow is swollen; becomes apparent after swelling subsides
- No pain — the deformity in children is typically painless
- Full range of motion usually preserved (elbow flexion-extension and forearm rotation intact)
- Deformity is progressive in appearance during growth (though not from growth arrest)
Clinical Signs
| Sign | Description |
|---|---|
| Gunstock deformity | The pathognomonic appearance — medial angulation of the forearm |
| Reduced carrying angle | Angle <5° or negative (varus) compared to contralateral side |
| Lateral epicondyle prominence | Becomes more visible/palpable due to the varus angulation |
| "Reversed" carrying angle | Forearm deviates medially rather than laterally on extension |
From S. Das Manual of Clinical Surgery: "When the carrying angle is abnormally decreased the condition is called cubitus varus." From Bailey & Love's: "cubitus varus (gun-stock deformity): the carrying angle is reversed, secondary to a malunited supracondylar fracture."

The normal carrying angle is present on the right side; cubitus varus deformity is obvious on the left side. (S. Das Manual on Clinical Surgery, Fig 13.12)
Late Complications (Adults with Untreated Cubitus Varus)
- Lateral elbow pain — from overloaded radiocapitellar compartment
- Posterolateral rotatory instability (PLRI) — episodic elbow instability, usually with the arm outstretched
- Snapping triceps syndrome — medial triceps subluxation causing painful snapping
- Tardy ulnar nerve palsy — late-onset ulnar neuropathy (rare, less common than in cubitus valgus)
- Osteochondral lesions of the radiocapitellar joint from chronic overloading
7. Radiological Assessment
Standard Radiographs
AP and lateral views of both elbows in full extension are mandatory for comparison.
The Baumann Angle (Humeral–Capitellar Angle)
This is the critical radiographic measurement for detecting and quantifying cubitus varus.
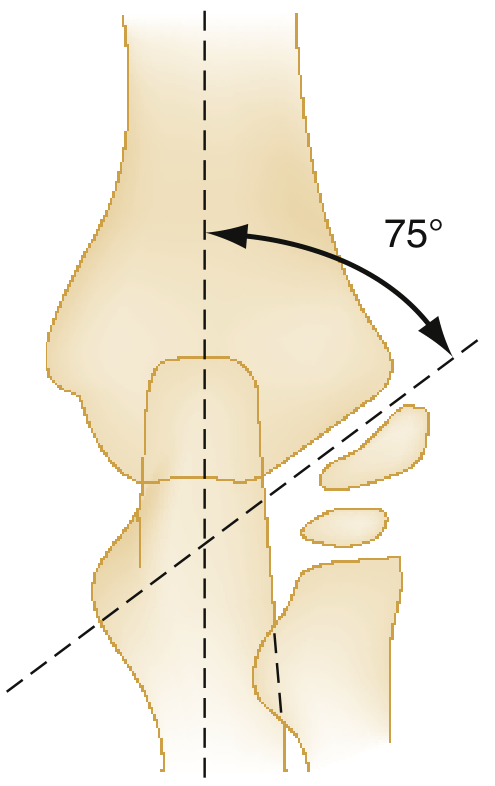
The Baumann angle: measured on AP radiograph as the angle between the longitudinal axis of the humerus and the physeal line of the capitellum. Normal value: 70–75° (equivalent to ~9–26° of humeral–capitellar valgus). A reduced Baumann angle indicates varus malunion.
From Rosen's Emergency Medicine: "The Baumann angle, normally 70 to 75 degrees, can be helpful in detecting subtle fractures and is formed by a line drawn to follow the growth plate of the capitellum and a line perpendicular to the long axis of the humerus."
From Miller's Review of Orthopaedics: "Humeral-capitellar (Baumann) angle should be in valgus and fall between 9 and 26 degrees."
AP Radiograph Findings in Cubitus Varus:

AP elbow X-ray: significant cubitus varus deformity. The forearm (radius and ulna) is angulated medially relative to the humerus. Altered distal humeral morphology indicates a sequela of malunited supracondylar fracture.
Key radiographic findings:
- Decreased or negative carrying angle on AP view
- Reduced Baumann angle (below normal 70–75°)
- Asymmetric metaphyseal height (medial column lower than lateral)
- Altered distal humeral shape
- Compare with contralateral normal elbow always
Additional Radiographic Lines (Lateral View):
- Anterior humeral line should bisect the middle third of the capitellum — displaced in type II/III fractures
- Fat pad signs — posterior fat pad displacement = pathologic (indicates joint effusion/fracture)
CT Scan
Useful preoperatively to:
- Quantify degree of varus, internal rotation, and hyperextension
- Plan corrective osteotomy geometry
- Assess for associated intra-articular changes (lateral compartment OA, loose bodies)
8. Classification
Classification of Cubitus Varus Deformity
There is no widely adopted single classification specifically for cubitus varus itself. It is classified based on:
A. Degree of Angular Deformity
| Grade | Carrying Angle |
|---|---|
| Mild | 0–5° (neutral, loss of normal valgus) |
| Moderate | Negative angle 5–15° (definite varus) |
| Severe | >15° varus |
B. Components of Deformity (Multiplanar Classification)
Complex cubitus varus has three components that must be assessed:
- Varus angulation (coronal plane) — primary deformity
- Internal rotation (axial plane) — often coexists, worsens cosmesis
- Hyperextension (sagittal plane) — may coexist, impacts function
C. Gartland Classification (of the Causative Supracondylar Fracture)
| Type | Description | Treatment |
|---|---|---|
| I | Nondisplaced | Long-arm cast 2–3 weeks |
| II | Displaced, posterior cortex intact | Cast vs. CRPP |
| IIIA | Completely displaced, posteromedial rotation | CRPP |
| IIIB | Completely displaced, posterolateral rotation | CRPP |
Type IIIA (posteromedial rotation of the distal fragment) carries the highest risk of cubitus varus malunion if inadequately reduced, as the medial rotation directly creates the varus tilt.
9. Investigations & Evaluation
Clinical Evaluation
History:
- Prior elbow fracture in childhood (supracondylar fracture)?
- Age at injury, treatment received
- Duration and progression of deformity
- Functional complaints? (most children are asymptomatic; adults may have pain, instability)
- Dominant limb affected?
Physical Examination:
- Inspect in anatomical position — compare carrying angles bilaterally
- Quantify the varus angle (or loss of valgus)
- Assess ROM — flexion-extension, pronation-supination (usually full)
- Assess for lateral condyle prominence
- Palpate medial epicondyle and assess ulnar nerve (Tinel's sign at cubital tunnel)
- Lateral pivot-shift test — for PLRI (if suspected late complication)
- Snapping triceps — check for medial triceps subluxation with flexion-extension
Imaging
| Investigation | Purpose |
|---|---|
| AP + lateral X-ray (bilateral) | Quantify deformity, compare Baumann angles |
| CT scan (3D reconstruction) | Pre-op planning, quantify rotation component |
| MRI | Assess for lateral compartment OA, LUCL integrity, osteochondral lesions |
| Ultrasound | Snapping triceps evaluation |
| Nerve conduction studies | If tardy ulnar nerve palsy suspected |
10. Treatment
Conservative (Non-surgical)
- Observation only for mild, asymptomatic deformities in children with good function
- No splinting or physiotherapy corrects an established bony deformity
- Appropriate when the deformity is cosmetically acceptable and there are no functional deficits
Surgical Treatment — Corrective Osteotomy
Surgery is indicated for:
- Moderate-to-severe deformity with cosmetic concern
- Functional impairment
- Pain (lateral compartment overloading)
- Posterolateral rotatory instability
- Snapping triceps syndrome
- Tardy nerve palsy
The timing of surgery: generally when the child is old enough to tolerate surgery safely (usually >6 years) and preferably before skeletal maturity. Earlier correction prevents late complications.
Types of Corrective Osteotomy
1. Lateral Closing-Wedge Osteotomy (Most Common)
- A wedge of bone is removed from the lateral side of the distal humerus (supracondylar region)
- The wedge is sized to correct the varus angle
- Medial cortex remains as a hinge
- Fixation: K-wires (crossed pins), plate and screws
- Advantages: Simple, reproducible, widely used
- Disadvantages: Increases lateral condyle prominence; does not correct rotational component
2. Dome (Curved) Osteotomy
- Curved cut allows correction in multiple planes simultaneously
- Addresses varus AND rotation in one procedure
- Technically more demanding
3. Step-Cut Osteotomy
- Step-shaped cut provides inherent stability
- Good rotational control
4. Medial Opening-Wedge Osteotomy
- A wedge is opened on the medial side
- Less popular; requires bone graft
5. French Osteotomy
- Modified lateral closing wedge with internal rotation correction
- Specifically designed to address the rotational component
Fixation Methods:
- Crossed K-wires — most commonly used in children; removed at 4–6 weeks
- Plate and screws — preferred in adolescents and adults for stability
- External fixator — for complex or revision cases
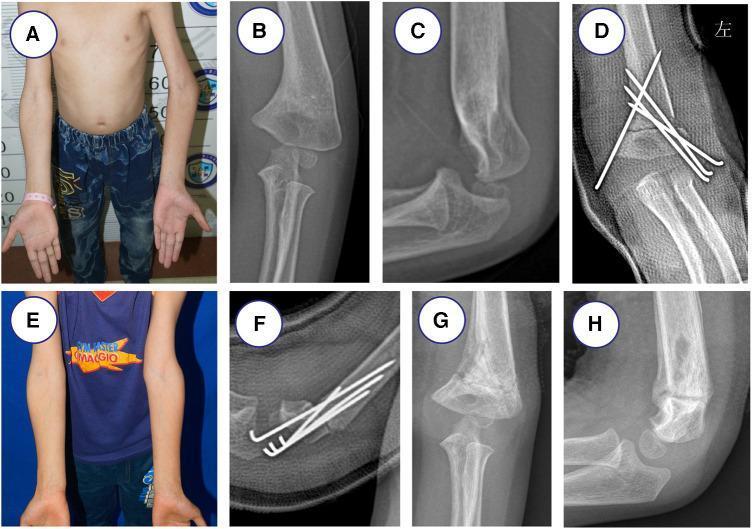
Surgical correction of cubitus varus: (A) preoperative gunstock deformity; (B, C) AP and lateral radiographs showing bony malalignment; (D) post-osteotomy K-wire fixation; (E) clinical correction achieved; (F-H) progressive healing on follow-up radiographs.

Clinical photographs: (a) preoperative — clear varus angulation with 20° of malalignment; (b) postoperative — carrying angle restored to near-normal after corrective osteotomy.
Postoperative Management
- Long-arm cast/splint at 90° elbow flexion for 4–6 weeks
- K-wires removed at 4–6 weeks under sedation
- Physiotherapy for ROM recovery (though ROM usually returns spontaneously in children)
- Expected correction to normal or slight overcorrection to valgus (5–10°)
11. Complications of Cubitus Varus (Untreated) & Post-Surgical
Untreated Complications
| Complication | Mechanism | Notes |
|---|---|---|
| Posterolateral rotatory instability (PLRI) | Chronic LUCL stretch from malalignment | Most serious late complication |
| Lateral compartment OA | Chronic overloading | Radiocapitellar arthritis |
| Snapping triceps syndrome | Medial triceps subluxation | Pain and snapping with elbow motion |
| Tardy ulnar nerve palsy | Altered cubital tunnel geometry | Less common than in cubitus valgus |
| Osteochondral lesions | Radiocapitellar impaction | Capitellar OCD |
Post-Surgical Complications
| Complication | Notes |
|---|---|
| Recurrence | Inadequate correction or growth-related |
| Overcorrection → cubitus valgus | Risks tardy ulnar nerve palsy |
| Iatrogenic ulnar nerve injury | From medial pin placement (3–8%) |
| Lateral condyle prominence | Increased with closing-wedge technique |
| Delayed union / non-union | Rare |
| Pin-site infection | More common in younger patients |
| Compartment syndrome | Rare |
12. Cubitus Varus vs Cubitus Valgus — Comparison
| Feature | Cubitus Varus | Cubitus Valgus |
|---|---|---|
| Carrying angle | Decreased / reversed | Increased |
| Forearm deviation | Medial (inward) | Lateral (outward) |
| Common cause | Malunited supracondylar fracture | Malunited lateral condyle fracture |
| Cosmesis | Gunstock deformity | Less obvious |
| Function | Usually preserved | Usually preserved |
| Nerve risk | PLRI, rarely ulnar nerve | Tardy ulnar nerve palsy (classic) |
| Mechanism | Malunion | Malunion / growth arrest |
13. Summary
| Key Feature | Detail |
|---|---|
| Definition | Decreased/reversed carrying angle; medial forearm deviation |
| Synonym | Gunstock deformity |
| Most common cause | Malunited supracondylar humerus fracture (type III, posteromedial) |
| Mechanism | Malunion (not growth arrest) |
| Key sign | Reversed carrying angle + lateral condyle prominence |
| Key investigation | AP X-ray both elbows; Baumann angle (normal 70–75°) |
| Functional impairment | Usually minimal in children; late PLRI in adults |
| Treatment of choice | Lateral closing-wedge osteotomy + K-wire fixation |
| Most feared late complication | Posterolateral rotatory instability |
Sources:
- S. Das: A Manual on Clinical Surgery, 13th Edition, Chapter 13
- Miller's Review of Orthopaedics, 9th Edition, Chapters 4 & 11
- Rosen's Emergency Medicine, 8th Edition, Chapter 170
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 35
This is a shared conversation. Sign in to Orris to start your own chat.