Pulse oximetry - principles, and applications, functioning complications and limitation
Reading File
Finding Sources
Finding Sources
Searching the Web
pulse oximetry principles applications complications limitations 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Pulse Oximetry: Principles, Applications, Functioning, Complications, and Limitations
1. Introduction
Pulse oximetry is a noninvasive, continuous method to assess the percentage of hemoglobin saturated with oxygen (SpO2) in arterial blood. It has become the standard of care across virtually all clinical settings since its adoption as a minimum anesthesia monitoring standard by the ASA in 1986, and it is now part of the WHO Safe Surgery Checklist.
"Pulse oximetry has become the standard of care in a wide variety of clinical settings."
- Roberts and Hedges' Clinical Procedures in Emergency
2. Physiologic Fundamentals
Hemoglobin Species and Oxygen Saturation
Five hemoglobin (Hb) species exist in adult blood:
- O2Hb - oxygenated hemoglobin
- deO2Hb - deoxygenated hemoglobin
- COHb - carboxyhemoglobin (normally 1-3%)
- MetHb - methemoglobin (normally <1%)
- SHb - sulfhemoglobin (normally <1%)
Two key saturation values are used:
- Functional SaO2 = O2Hb / (O2Hb + deO2Hb) x 100
- Fractional SaO2 = O2Hb / (O2Hb + deO2Hb + COHb + MetHb + SHb) x 100
Standard pulse oximeters measure functional saturation only, using just two wavelengths of light. They cannot distinguish additional hemoglobin species such as COHb or MetHb. CO-oximeters use 4+ wavelengths to measure fractional saturation.
The oxyhemoglobin dissociation curve means that SaO2 is not linearly related to PaO2 - a patient can have a "normal-appearing" SpO2 while PaO2 has already dropped substantially (the flat upper portion of the curve).
(Miller's Anesthesia, 10e)
3. Physical Principle: Beer-Lambert Law
Pulse oximetry is based on two combined principles:
- Beer-Lambert Law: The concentration of an unknown solute (here, hemoglobin species) can be determined by measuring light absorption - each substance absorbs light at a characteristic wavelength.
- Optical plethysmography: The pulsatile nature of arterial blood is used to isolate the arterial component from background tissue and venous blood.
(Roberts and Hedges' Clinical Procedures in Emergency)
4. How It Works: Functioning
Light Wavelengths
Two light-emitting diodes (LEDs) emit at:
- 660 nm (red light): Deoxygenated Hb (deO2Hb) absorbs more strongly at this wavelength
- 940 nm (infrared light): Oxygenated Hb (O2Hb) absorbs more strongly at this wavelength
Because the absorption spectra of O2Hb and deO2Hb differ at these two wavelengths, the ratio of absorption allows the oximeter to calculate the proportion of each.
AC/DC Signal Separation
Light passing through tissue is absorbed by:
- Tissue (bone, fat, connective tissue) - constant, does not change with heartbeat
- Venous blood - constant (nonpulsatile, "DC component")
- Arterial blood at baseline - constant ("DC component")
- Pulsatile surge of arterial blood with each heartbeat - variable ("AC component")
The oximeter isolates the pulsatile (AC) component - which represents only arterial blood - by subtracting the nonpulsatile (DC) background from the total signal.
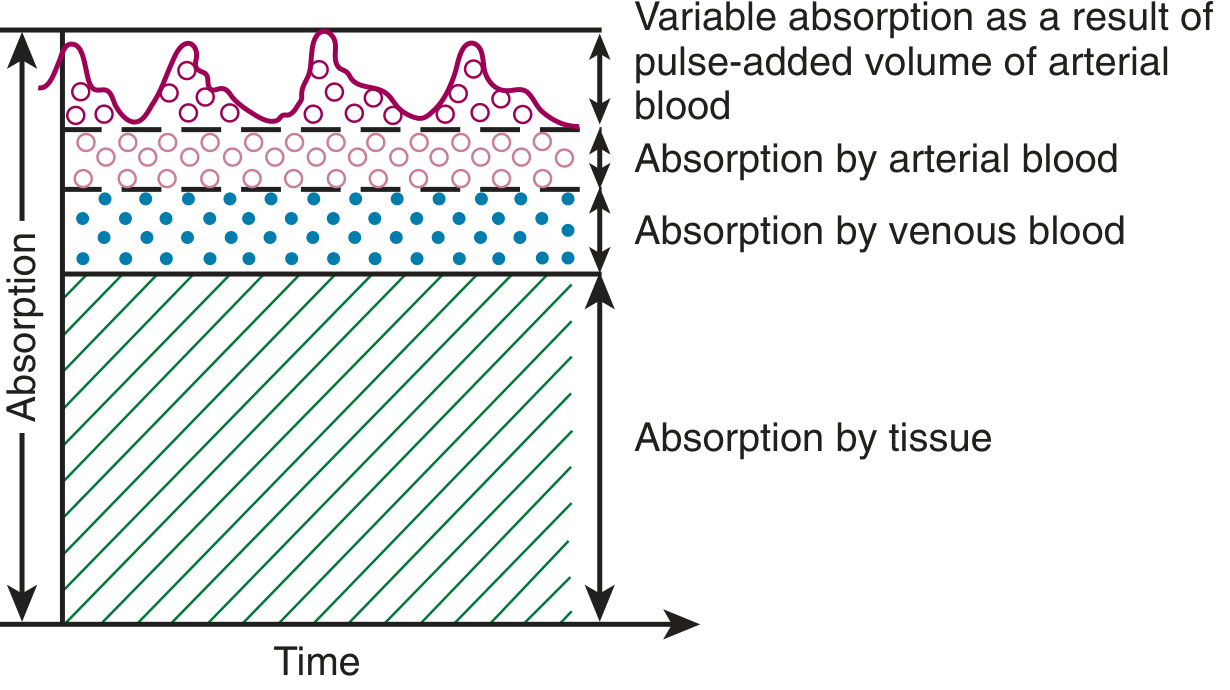
Figure: Factors influencing light absorption through a pulsatile vascular bed. The pulsatile top layer (arterial surge) is the only component that changes with each heartbeat and is isolated for SpO2 calculation. (From Roberts and Hedges' Clinical Procedures in Emergency)
The R Ratio
The ratio R is calculated as:
R = (AC660 / DC660) / (AC940 / DC940)
R is then mapped to SpO2 via an empirically derived internal calibration curve built into each device - developed by manufacturers using healthy volunteers breathing hypoxic gas mixtures across SpO2 70-100%.
(Miller's Anesthesia, 10e)
FDA Accuracy Standard
The FDA requires root mean square differences between SpO2 and true SaO2 of ≤3.0% for clip/wrap sensors and ≤3.5% for ear clip/reflectance sensors. Most manufacturers report accuracy of ±2-3% over the 70-100% SpO2 range.
Probe Design
- Transmission oximetry: Emitter and detector placed on opposite sides of tissue (e.g., fingertip over nailbed, toe, or earlobe)
- Reflectance oximetry: Emitter and detector on the same side; typically placed on the forehead
- The photodetector alternately cycles each LED on/off and measures ambient light (both LEDs off) to subtract background noise.
5. Clinical Applications
| Setting | Application |
|---|---|
| Operating room | Minimum intraoperative monitoring standard (ASA, WHO Safe Surgery Checklist) |
| ICU / Critical care | Continuous SpO2 monitoring; FiO2 and PEEP titration on mechanical ventilation; weaning assessment |
| Emergency department | Early detection of hypoxemia; procedural sedation monitoring |
| Neonatology | Universal newborn screening for critical congenital heart disease (SpO2 <95% or >2% difference between limbs) |
| Gastroenterology / Endoscopy | Monitoring during conscious sedation procedures |
| Postoperative ward | Detecting occult desaturation in post-surgical patients |
| COVID-19 / Remote monitoring | Remote and home-based SpO2 surveillance |
| Pediatrics | All age groups for hypoxemia detection |
Importantly, widespread pulse oximetry use has reduced the need for arterial blood gas (ABG) measurements in many clinical settings. (Schwartz's Principles of Surgery, 11e)
Photoplethysmography (Extra Capability)
Beyond SpO2, the pulse oximeter waveform can be used as a photoplethysmograph - the amplitude and variation of the waveform reflect changes in arterial blood volume and distensibility. Respiratory variation in the plethysmographic trace (pleth variability index, PVI) can estimate fluid responsiveness and hypovolemia during mechanical ventilation. (Miller's Anesthesia, 10e)
Multiwavelength / Pulse CO-Oximetry
Next-generation devices use up to 12 wavelengths to noninvasively measure:
- SpHb (total hemoglobin concentration)
- SpCO (carboxyhemoglobin)
- SpMet (methemoglobin)
This can potentially reduce the need for blood draws and enable early detection of hemorrhage. However, accuracy for SpHb remains limited at clinically relevant ranges (6-10 g/dL), and noninvasive COHb has not yet replaced laboratory co-oximetry. (Miller's Anesthesia, 10e; Schwartz's Surgery, 11e)
6. Complications and Sources of Error
A. Dyshemoglobinemias (Most Clinically Significant)
| Condition | Effect on SpO2 |
|---|---|
| Carbon monoxide poisoning (COHb) | SpO2 falsely elevated - COHb absorbs similarly to O2Hb at 660 nm and is misread as oxyhemoglobin. SpO2 may appear 98-100% while the patient is severely poisoned. |
| Methemoglobinemia | SpO2 trends toward 85% regardless of true saturation. At high MetHb levels the device reads approximately 85% independent of whether true SaO2 is higher or lower. |
| Sulfhemoglobin | May cause falsely low readings |
"In patients with methemoglobinemia or elevated carboxyhemoglobin levels, pulse oximetry does not accurately depict quantitative changes in hemoglobin O2 saturation."
- Roberts and Hedges' Clinical Procedures in Emergency
Management: Co-oximetry (ABG with co-oximetry) is required whenever dyshemoglobinemia is suspected.
B. Reduced Peripheral Perfusion / Low Signal States
Conditions that reduce pulsatility impair the ability to isolate the arterial AC component:
- Hypotension / circulatory shock
- Vasoconstriction (cold, vasopressors)
- Hypothermia
- Peripheral vascular disease
C. Motion Artifact
Patient movement causes false pulsatile signals. Most modern devices use signal processing algorithms to minimize this, but it remains a significant source of error, especially in agitated patients or during transport.
D. Venous Pulsation / Venous Congestion
Elevated venous pressure (e.g., tricuspid regurgitation, right heart failure, Blalock-Taussig shunts) can make venous blood pulsatile, causing the device to sample venous rather than arterial saturation - resulting in falsely low readings.
E. Skin Pigmentation / Racial Bias (Emerging Concern)
Multiple studies have confirmed that standard pulse oximeters overestimate true SaO2 in patients with darker skin pigmentation. In one large series of >48,000 paired measurements:
- Occult hypoxemia (SpO2 92-96% with true SaO2 <88%) occurred in 12-17% of Black patients vs. 3.6-6.2% of White patients.
- One study found occult hypoxemia was 3 times more frequent in Black vs. White patients at SpO2 92-96%.
The FDA and AARC have both flagged this as a patient safety issue requiring updated device testing and premarket standards. (Goldman-Cecil Medicine; Fishman's Pulmonary Diseases)
F. Nail Polish and External Interference
- Blue or green nail polish can artificially alter light absorption at the relevant wavelengths, causing inaccurate readings (similar effect to darker skin pigmentation per Goldman-Cecil).
- Bright ambient light (operating room lights, fluorescent lights) can be detected by the photodetector; most devices subtract ambient light when both LEDs are off, but very intense light may still cause interference.
- Intravenous dyes (e.g., methylene blue, indocyanine green) transiently lower SpO2 readings.
G. Anemia
Severe anemia alone does not cause false SpO2 readings (the device measures the saturation fraction, not absolute Hb content), but with very low Hb, even a "normal" SpO2 represents severe oxygen delivery failure.
7. Limitations
| Limitation | Clinical Implication |
|---|---|
| Cannot detect hyperoxia | Because PaO2 >70 mmHg all maps to ~99-100% SpO2, dangerous hyperoxia (e.g., in neonates) goes undetected |
| Insensitive to changes in PaO2 from 90 to 65 mmHg | Due to the flat portion of the oxyhemoglobin dissociation curve, large drops in PaO2 can occur without SpO2 changing until below ~70 mmHg |
| No CO2 or acid-base information | Cannot replace ABG for pH, PaCO2, bicarbonate, or base excess |
| Two-wavelength limitation | Only measures functional saturation; cannot detect COHb, MetHb, or other Hb variants |
| Accuracy declines at SpO2 <90% | Average SpO2-SaO2 discrepancy increases below 90%; readings below 85% are unreliable |
| Inaccurate below SpO2 ~70% | Calibration curves are not validated below 70% SpO2 (ethical limitations in calibration studies) |
| Delayed response | Probe site (finger) may lag central changes by 30-60 seconds |
| Cannot detect apnea without desaturation | In a patient pre-oxygenated with high FiO2, SpO2 can remain normal for several minutes during apnea - a dangerous false reassurance |
| Racial bias | Systematic overestimation in darker-skinned individuals |
8. Comparison: Pulse Oximetry vs. Co-Oximetry vs. ABG
| Feature | Pulse Oximetry | Co-Oximetry (ABG) |
|---|---|---|
| Invasive? | No | Yes (arterial blood) |
| Continuous? | Yes | No (point-in-time) |
| CO2/pH | No | Yes |
| COHb, MetHb | No | Yes |
| Dyshemoglobins | Cannot detect | Can quantify |
| Accuracy at low SpO2 | Reduced | High |
Summary
Pulse oximetry uses Beer-Lambert law and optical plethysmography, emitting red (660 nm) and infrared (940 nm) light to calculate the SpO2 from the pulsatile arterial blood signal. It is fast, noninvasive, continuous, and indispensable across anesthesia, critical care, emergency medicine, neonatology, and remote monitoring. Its key limitations are the inability to detect dyshemoglobinemias (most critically CO poisoning), reduced accuracy in low perfusion states and motion, the well-documented racial bias toward overestimating SpO2 in darker-skinned individuals, and insensitivity to hyperoxia and early drops in PaO2. In any situation where dyshemoglobinemia is suspected or SpO2 appears discordant with clinical status, co-oximetry via ABG is required.
Sources:
- Miller's Anesthesia, 10e, Chapter 37
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapters 1 and 25
- Goldman-Cecil Medicine International Edition, Chapter 89
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set, Chapter on Monitoring
- Schwartz's Principles of Surgery, 11e, Chapter on Physiologic Monitoring
This is a shared conversation. Sign in to Orris to start your own chat.