Normal and c section procedures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from authoritative textbooks. Here is the complete answer:
Normal (Vaginal) Delivery vs. Cesarean Section (C-Section)
PART 1: NORMAL (VAGINAL) DELIVERY
The Three Stages of Labor
Labor is a continuous process divided into three clinical stages, sourced from Tintinalli's Emergency Medicine and The Developing Human - Clinically Oriented Embryology:
Stage 1 - Cervical Dilation
The first stage runs from the onset of regular uterine contractions to full cervical dilatation (10 cm). It is subdivided into:
- Latent phase: Mild, infrequent, irregular contractions. The cervix gradually effaces (thins) and softens. This preparatory phase may last many hours.
- Active phase: Begins once the cervix reaches ~3-4 cm dilation. Cervical dilation proceeds at an average rate of 1.2 cm/hr in nulliparous (first-time) and 1.5 cm/hr in multiparous women.
Average duration:
- First pregnancy (primigravida): ~12 hours
- Subsequent pregnancies (multigravida): ~7 hours
| Feature | True Labor | False Labor |
|---|---|---|
| Rhythm | Regular | Irregular |
| Intervals | Gradually shorten | Unchanged |
| Intensity | Gradually increases | Unchanged |
| Discomfort location | Back and abdomen | Lower abdomen only |
| Effect of sedation | No effect | Usually relieved |
| Cervical dilation | Yes | No |
Stage 2 - Expulsion (Delivery of the Baby)
Begins at full cervical dilation and ends with delivery of the infant. During this stage the fetus descends through the cervix and vagina via six cardinal movements:
- Engagement - the widest diameter of the head passes the pelvic inlet
- Flexion - the head flexes onto the chest for a smaller diameter
- Descent - the head descends through the pelvis
- Internal rotation - the occiput rotates to face anteriorly (toward the pubic symphysis)
- Extension - the head extends as it passes under the pubic arch; "crowning" occurs
- External rotation (restitution) - the head turns to face the thigh, aligning the shoulders
Average duration: ~54 minutes for nulliparous, ~20 minutes for multiparous women.
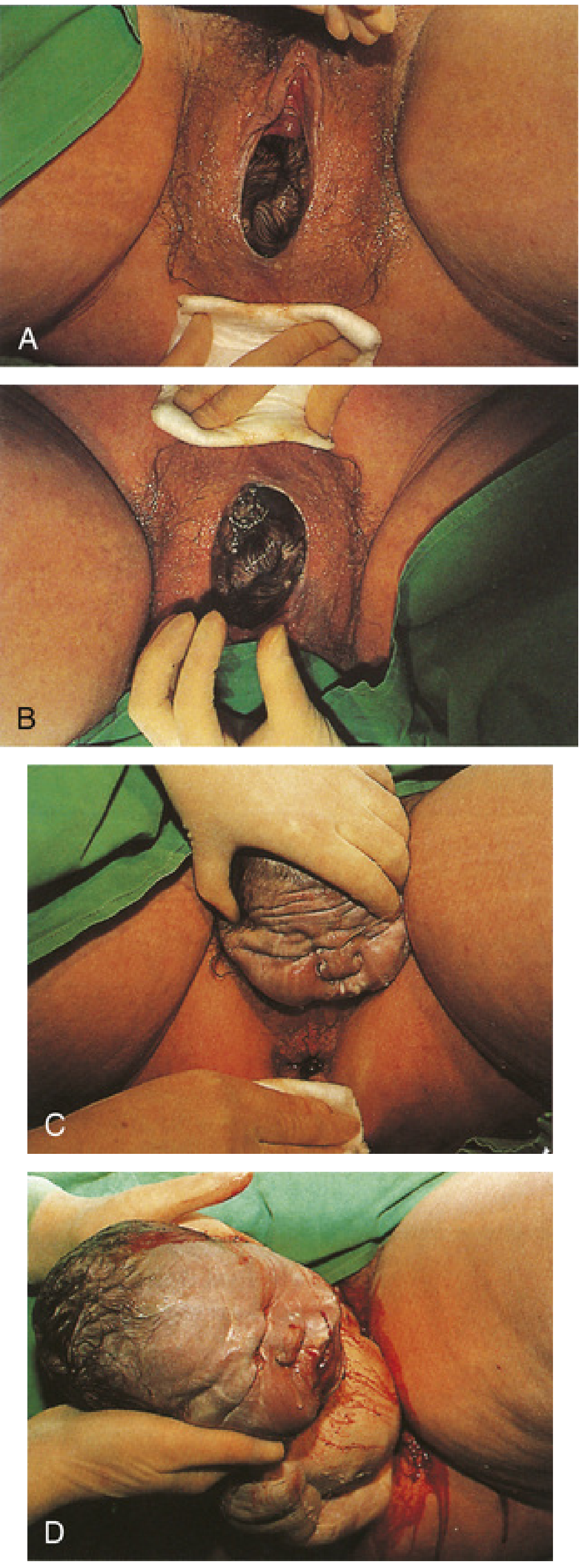
Fig: Spontaneous vaginal delivery. A - scalp visible with contractions. B - crowning of the head. C - head in anteroposterior position at delivery. D - delivery of the head and shoulders. (Developing Human - Clinically Oriented Embryology, p. 371)
Key steps during delivery:
- Prepare the perineum with soap, water, and povidone-iodine if time allows
- Gentle digital stretching of the inferior perineum to aid passage
- Episiotomy if needed (fetal distress, shoulder dystocia, instrumental delivery): inject 5-10 mL of 1% lidocaine; 2-3 cm incision either midline or mediolateral (45°). Mediolateral has lower risk of extension to the anal sphincter.
- Do not routinely suction the mouth and nose (can cause bradycardia and hypoxia)
- After head delivery: place the posterior hand under the axilla, grasp the ankles firmly ("don't drop the baby" - amniotic fluid, blood, and vernix make the infant very slippery)
Stage 3 - Placental Delivery
Begins after delivery of the infant and ends with expulsion of the placenta and membranes.
- Duration: completed within 15 minutes in ~90% of births
- A placenta not delivered within 60 minutes is classified as a retained placenta
- Retraction of the uterus reduces the placental attachment area; a hematoma forms beneath the placenta and separates it from the uterine wall
- Myometrial contractions constrict the spiral arteries, preventing excessive bleeding
Assessment During Labor
- Normal fetal heart rate: 120-160 beats/min
- Bradycardia: <110 bpm; Tachycardia: >160 bpm
- Fetal distress signs: persistent bradycardia, tachycardia, or late decelerations (drops in heart rate during AND >30 seconds after a contraction)
- Fundal height in cm approximates gestational age in weeks (±2 weeks) after 20 weeks
- Gestational age estimate: last menstrual period + 9 months and 7 days (Naegele's rule)
PART 2: CESAREAN SECTION (C-SECTION)
Definition and History
Cesarean delivery is surgical delivery of the infant through incisions in the abdominal wall and uterus. It is one of the most important developments in modern perinatal medicine - maternal mortality from cesarean operations in the 19th century exceeded 85%; by the 1980s it was performed safely in millions of women annually. (Creasy & Resnik's Maternal-Fetal Medicine, p. 957)
The C-section rate in the US reached a peak of 23.5% in 1988, driven by four main indications: dystocia, repeat cesarean, breech presentation, and fetal distress.
Indications for C-Section
C-section is indicated whenever delivery is necessary and vaginal delivery poses greater risk to mother or fetus than abdominal delivery. Common indications include:
- Dystocia (failure of labor to progress / cephalopelvic disproportion) - accounts for ~30% of cases
- Repeat cesarean delivery (prior uterine scar)
- Breech presentation (especially footling breech)
- Fetal distress (non-reassuring fetal heart rate patterns)
- Placenta previa (placenta covering the cervical os)
- Very low birth weight (<1500 g) - to avoid birth trauma
- Multiple gestation with first twin in non-vertex position
- Macrosomia (estimated fetal weight >4500 g, or >4000 g in a diabetic mother)
- Maternal HIV infection (to reduce vertical transmission)
- Perimortem (cardiac arrest in a pregnant woman)
- Active genital herpes infection
There are no absolute contraindications other than informed patient refusal after risks have been explained.
Types of Uterine Incisions
| Incision Type | Advantages | Disadvantages |
|---|---|---|
| Low transverse (Kerr) - most common, >90% | Thin, less vascular lower segment; heals well, lowest dehiscence risk | Risk of lateral extension into uterine vessels |
| Low vertical (Kronig) | Useful if lower segment thick or has fibroids; transverse lie; fetal anomalies | Requires greater bladder separation; repeat C-section needed if upper segment entered |
| Classic (midline vertical) | Fastest access; better exposure; good for emergencies | More blood loss; difficult 3-layer repair; 8x greater dehiscence risk; adhesion formation |
Step-by-Step Surgical Technique (Low Transverse / Pfannenstiel Approach)
Source: Pfenninger and Fowler's Procedures for Primary Care, p. 1135-1138
Preparation:
- Tilt table or place a wedge to the patient's left to improve venous return and fetal oxygenation
- Anesthesia: regional (epidural or spinal) preferred; general anesthesia when needed
- IV antibiotic prophylaxis: cefoxitin 1g IV (or clindamycin 600 mg IV for penicillin allergy) - given after cord clamping, reduces wound infection by 50%
Step-by-step incision and delivery:
- Pfannenstiel skin incision: horizontal incision ~13-15 cm wide, two fingerbreadths above the pubic symphysis (No. 20 blade)
- Subcutaneous dissection: carry down through fat to fascia; make a 2-cm horizontal fascial incision, extend laterally and superiorly with curved Mayo scissors
- Fascial elevation: grasp the superior fascial edge with Kocher clamps; bluntly dissect fascia off the underlying rectus muscle along the linea alba
- Peritoneal entry: bluntly separate the rectus muscles in the midline; tent the peritoneum with two hemostats and incise with the scalpel (keep above the bladder)
- Bladder retraction: place DeLee bladder retractor
- Bladder flap development: incise and dissect the peritoneum off the lower uterine segment ~12 cm wide; reapply the bladder retractor to protect the bladder
- Uterine incision (scoring): incise the lower uterine segment over the fetal head, proceeding mm by mm to avoid fetal injury; announce "uterine incision" for the anesthesiologist and nursery team
- Extend uterine incision: use fingers bluntly or bandage scissors (with two fingers inside protecting the fetus) to extend the incision ~10-11 cm in a curvilinear fashion
- Rupture membranes: with Allis clamp if not already ruptured
- Deliver the head: insert a cupped hand over the fetal head/occiput, keeping the wrist straight; gently lift upward. If the head is deeply engaged, an assistant pushes from below vaginally, or terbutaline 0.25 mg SC/IV is given to relax the uterus
- Deliver body: suction the infant's mouth and nose; deliver anterior shoulder, then posterior shoulder, then the rest of the body (same as vaginal delivery)
- Cord clamping: doubly clamp and cut the cord; send cord blood if required
- Placenta delivery: manually extract with fingers; remove membranes with ring forceps
- Uterine massage and inspection: Pennington clamps on bleeding edges; clean endometrium with moist lap sponges; if cervix closed, dilate with cervical dilators
- Uterine closure: running locked stitch with 0 chromic suture (avoid including the endometrium); add a second imbrication layer if bleeding continues
- Inspect: check uterus, tubes, ovaries; perform tubal ligation here if desired
- Irrigation: irrigate the pouch of Douglas and abdominal cavity with warm saline; inspect appendix and gallbladder
- Fascial closure: running stitch with 1-0 Vicryl, sutures no more than 1 cm apart
- Skin closure: irrigate subcutaneous fat; skin closure with staples or suture
Complications of C-Section
Maternal:
- Hemorrhage requiring transfusion
- Wound infection (reduced by prophylactic antibiotics)
- Bladder or ureteral injury
- Bowel injury
- Postoperative ileus
- DVT and pulmonary embolism
- Endometritis/peritonitis
- Need for hysterectomy (rare)
- Future pregnancy risks: uterine rupture at scar site (~0.5% with trial of labor after cesarean / TOLAC); placenta previa or accreta
Fetal:
- Accidental scalpel lacerations (1-2% of cases, usually cosmetic only; rarely serious)
- Transient tachypnea of the newborn (due to retained lung fluid, more common with elective C-section vs. vaginal delivery)
Emergency / Perimortem C-Section
For a pregnant woman in cardiac arrest (≥20 weeks gestation), the AHA advises beginning delivery after 4 minutes of CPR, completing delivery by 5 minutes (the "4-minute/5-minute rule"). Steps:
- Vertical skin incision from xiphoid to pubic symphysis
- Through skin, fat, fascia, and peritoneum
- Vertical uterine incision with two-finger protection of the fetus
- Deliver the fetus, suction airway, double-clamp and cut the cord
- Deliver the placenta and sweep the endometrial cavity
Key Comparisons: Normal Delivery vs. C-Section
| Feature | Normal Vaginal Delivery | Cesarean Section |
|---|---|---|
| Route | Through the vagina | Through abdominal and uterine incisions |
| Anesthesia | Epidural, local, or none | Spinal/epidural (preferred) or general |
| Duration (delivery phase) | Variable (stage 2: 20-54 min) | Skin-to-delivery ~5-10 min; total OR time ~45-60 min |
| Recovery | Faster (days) | Longer (weeks) |
| Maternal risk | Lower for uncomplicated delivery | Higher morbidity overall; 5-7x higher mortality if complications excluded |
| Neonatal respiratory adaptation | Better (birth canal squeezes fluid from lungs) | Higher risk of transient tachypnea |
| Future pregnancies | Normal risk | Scar risk: uterine rupture ~0.5% with TOLAC |
| Urinary incontinence risk | Higher | Lower |
Sources:
- The Developing Human - Clinically Oriented Embryology, pp. 370-372
- Tintinalli's Emergency Medicine, Ch. 101
- Pfenninger and Fowler's Procedures for Primary Care, Ch. 162
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Ch. 40
This is a shared conversation. Sign in to Orris to start your own chat.