What is chalzion ?
Reading File
Searching the Web
chalazion eyelid meibomian gland treatment 2024
Finding Sources
Searching PubMed
chalazion meibomian gland treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of chalazion based on authoritative ophthalmology textbooks:
Chalazion (Meibomian Cyst)

Definition
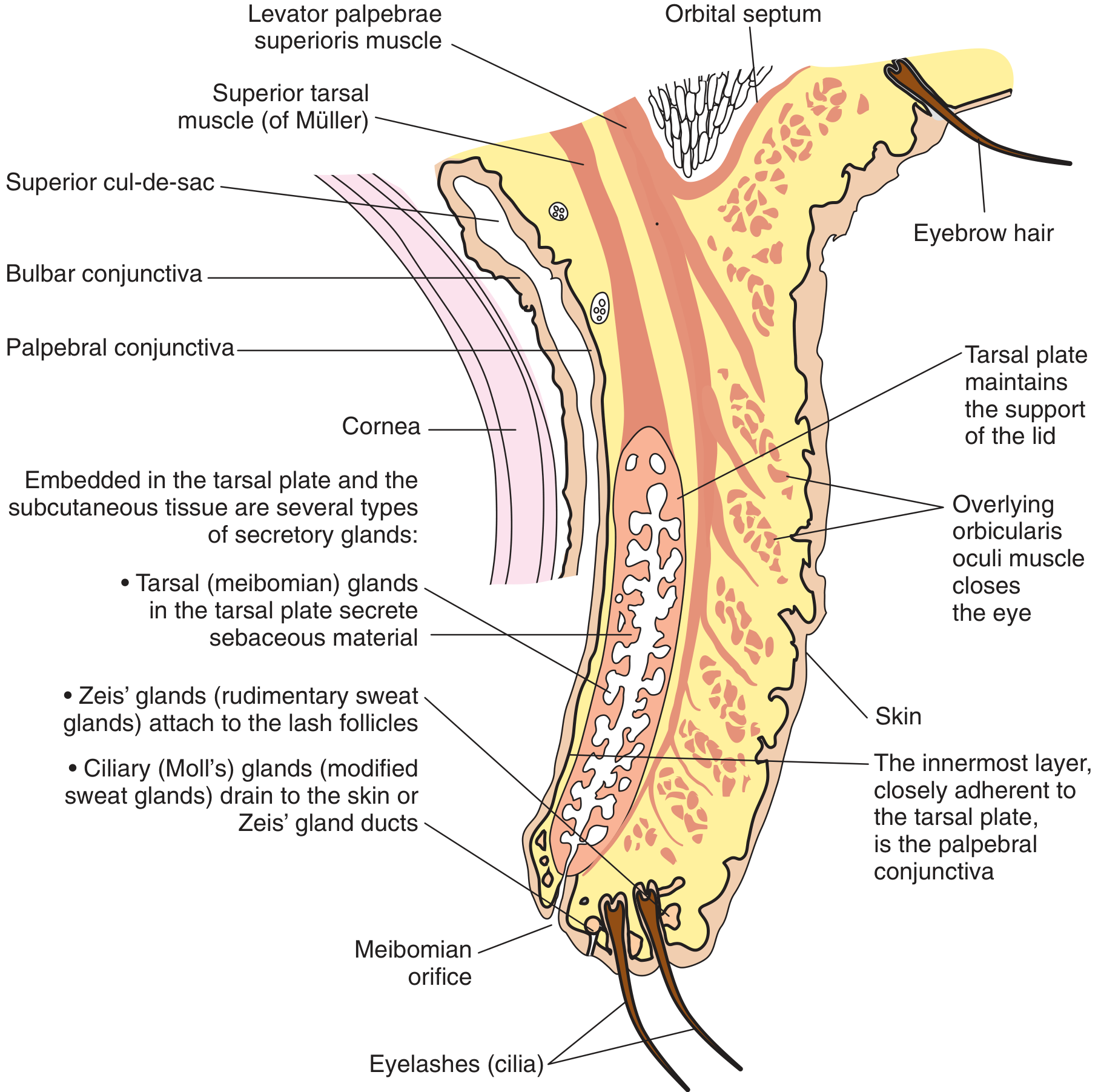
A chalazion is a focal, chronic granulomatous inflammatory lesion (lipogranuloma) within the eyelid caused by obstruction of a meibomian gland (or occasionally a gland of Zeis), resulting in retained sebaceous secretions. It is also called a meibomian cyst. - Wills Eye Manual, p. 381
Pathogenesis
When a meibomian gland becomes blocked, its oily secretions accumulate and leak into the surrounding tarsal tissue. This triggers a sterile chronic inflammatory reaction characterized histologically by:
- Extracellular fat deposits
- Lipid-laden epithelioid cells
- Multinucleated giant cells
- Lymphocytes
This pattern is called a lipogranuloma. - Kanski's Clinical Ophthalmology, 10th ed., p. 54
Predisposing conditions:
- Blepharitis (very commonly associated)
- Rosacea (associated with multiple and recurrent chalazia)
- Bortezomib therapy (a proteasome inhibitor used in multiple myeloma - can induce chalazia within 3 months of starting treatment)
Symptoms & Signs
| Feature | Detail |
|---|---|
| Presentation | Slow-growing, painless (or mildly tender) eyelid lump |
| Location | Upper or lower lid; can be on the tarsal or marginal surface |
| Feel | Smooth, firm, well-defined nodule - can be "rolled" over the tarsal plate |
| Acutely inflamed | May become red, swollen, and tender |
| Conjunctival surface | Appears as a localized red elevation when eyelid is everted |
Critical sign: A visible or palpable, well-defined, subcutaneous nodule in the eyelid is the hallmark finding. - Wills Eye Manual, p. 382
Chalazion vs. Hordeolum (Stye) - Key Differences
| Feature | Chalazion | Hordeolum (Stye) |
|---|---|---|
| Nature | Sterile lipogranuloma | Acute bacterial infection (usually Staph.) |
| Pain | Usually painless | Tender, painful |
| Location | Within the tarsal plate (meibomian gland) | Eyelid margin (gland of Zeis or lash follicle) |
| Onset | Gradual, chronic | Acute |
| Treatment | Warm compresses ± steroids ± I&C | Antibiotics + local heat |
Differential Diagnosis
- Preseptal cellulitis - diffuse eyelid/periorbital erythema and edema
- Pyogenic granuloma - deep-red, pedunculated conjunctival lesion
- Sebaceous carcinoma - suspect in older patients with recurrent chalazia, eyelid thickening, loss of eyelashes (madarosis), or chronic unilateral blepharitis. A recurrent chalazion in the same lid position in an older patient must be biopsied to exclude malignancy. - Kanski's, p. 54
Treatment
Step 1 - Conservative (First-line)
- Warm compresses for at least 10 minutes, 4 times daily, with gentle massage over the lesion
Step 2 - Medical
- Topical antibiotic/steroid (e.g., neomycin/polymyxin B/dexamethasone ointment b.i.d. for 1-2 weeks)
- For multiple or recurrent chalazia / ocular rosacea: low-dose doxycycline 20-50 mg orally daily to b.i.d. for its antibacterial and anti-inflammatory properties
Step 3 - Procedural (if no resolution after 3-4 weeks)
- Intralesional steroid injection - triamcinolone 40 mg/mL (0.2-1.0 mL, mixed 1:1 with lidocaine/epinephrine). Note: risk of permanent skin depigmentation/atrophy, especially in darker-skinned individuals. Rare but serious risk: retrograde intra-arterial injection causing central retinal artery occlusion.
- Incision and curettage (I&C) - performed from the conjunctival surface via a chalazion clamp, to avoid a visible skin scar. All excised material should be sent for histopathology.
- Wills Eye Manual, pp. 382-383; Bailey and Love's Surgery, 28th ed., p. 747
Important Clinical Tip
Any chalazion that recurs in the same position, especially in an older patient, must be biopsied to rule out masquerading sebaceous gland carcinoma. - Kanski's Clinical Ophthalmology, 10th ed.
Sources: Kanski's Clinical Ophthalmology, 10th ed. | Wills Eye Manual | Bailey and Love's Short Practice of Surgery, 28th ed.
Explain Ot procedure for it
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Now I have everything needed for a complete, well-illustrated answer.
OT Procedure for Chalazion: Incision and Curettage (I&C)
The standard operative procedure is Incision and Curettage (I&C) - a minor surgical procedure performed under local anaesthesia.
Anatomy Relevant to the Procedure
Indications for Surgery
- Chalazion unresponsive to 3-4 weeks of medical therapy
- Lesion large enough to palpate or cosmetically concerning
- Visual problems caused by the lump (e.g., astigmatism, blurry vision)
- Patient request for removal
Contraindications
- Chalazion that has recently drained through the skin (risk of "buttonhole" full-thickness lid defect)
- Skin markedly inflamed or crusted
- Chalazion near the lacrimal punctum (risk of damage to lacrimal drainage - refer to ophthalmologist)
- Anticoagulated patient (relative contraindication)
Equipment Required
| Item | Purpose |
|---|---|
| Topical anaesthetic drops (e.g., tetracaine) | Surface anaesthesia of conjunctiva |
| 2% lidocaine with epinephrine + 30G needle, 3 mL syringe | Local anaesthetic injection + haemostasis |
| Chalazion clamp (2-3 sizes) | Eversion, stabilisation, and haemostasis |
| No. 15 scalpel blade | Incision |
| Chalazion curettes (2 sizes) | Removal of granulomatous contents |
| Ocular tissue forceps (0.2 tips) | Removal of granulation tissue |
| Westcott conjunctival scissors | Trimming inflamed tarsus if needed |
| Cotton swabs + gauze | Haemostasis |
| Antibiotic-steroid ointment (e.g., TobraDex/Maxitrol) | Postoperative care |
| Eye patch + tape | Pressure dressing |
| 6-0 nylon suture (standby) | Only if accidental full-thickness lid defect occurs |
Pre-operative Preparation
- Discontinue aspirin/antiplatelet drugs 1 week before; anticoagulants 4 days before
- Counsel patient about: risk of scarring, recurrence, swelling/bruising, bleeding, infection, rare risk of lacrimal duct damage
- Mark the chalazion on the skin with a marking pen before injecting anaesthetic (LA injection can obscure the lesion by distorting tissue)
Step-by-Step Technique
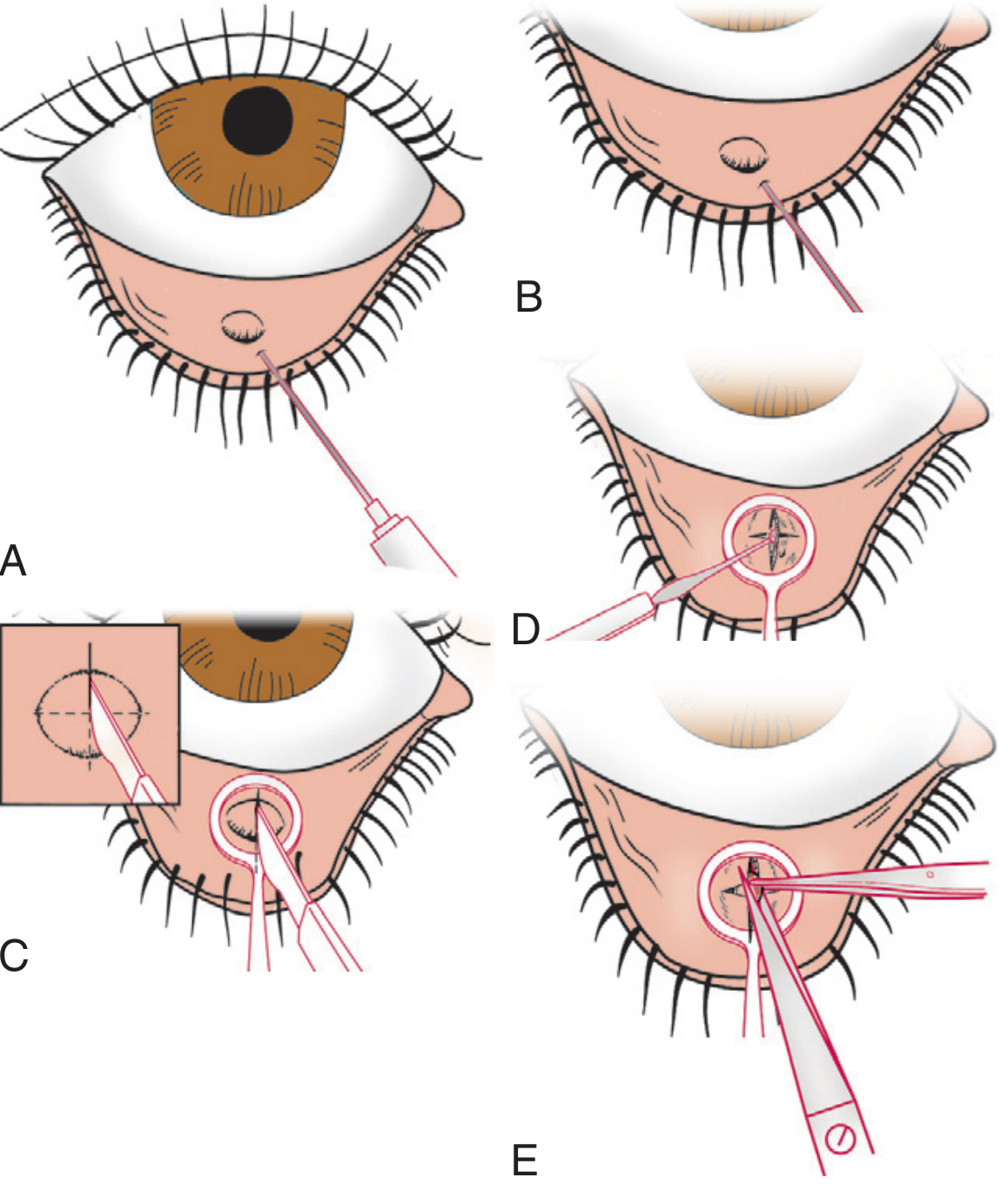
Step 1 - Anaesthesia
- Instil several drops of topical anaesthetic (tetracaine) into the eye
- Inject 2% lidocaine with epinephrine through the skin surface over the chalazion area where the clamp will be applied
- The epinephrine reduces bleeding during the procedure
Step 2 - Eyelid Eversion and Clamp Application
- Place the chalazion clamp over the eyelid with the open (ring) side on the conjunctival (inner) surface, centring the chalazion in the ring opening
- Tighten firmly (but do not over-tighten) - this provides haemostasis
- Evert the eyelid using the clamp as a lever so the conjunctival surface faces upward
- The chalazion will now be visible and bulging through the ring of the clamp
Step 3 - Incision
- Using a no. 15 scalpel blade, make two incisions in the form of a cross ("X") directly over the chalazion through the conjunctival surface
- The incision is vertical (along the axis of the meibomian gland) to avoid damaging adjacent glands
- Take care not to go through the eyelid skin - stay within the substance of the chalazion only
- Release of soft yellowish/grey material confirms correct placement
Step 4 - Curettage
- Use a chalazion curette to scrape and remove as much soft, gelatinous, inflamed material as possible
- Use cotton swabs to wipe out residual contents
- Remove granulation tissue with tissue forceps
Step 5 - Tarsus Trimming (if needed)
- If inflamed tarsal tissue is still present, use Westcott conjunctival scissors and forceps to remove a small amount of inflamed tarsal plate
- Caution: avoid "tenting" deep tissue which can create a full-thickness "buttonhole" defect through the skin
- Avoid damaging the eyelid margin at all times
Step 6 - Haemostasis and Dressing
- Remove the chalazion clamp - expect significant bleeding (eyelid is highly vascular)
- Apply direct pressure with cotton swabs/gauze for 5-10 minutes until haemostasis is achieved
- Apply antibiotic-steroid ointment (e.g., TobraDex)
- Apply a pressure patch over the eye
Postoperative Care
- Patient removes the eye patch the same evening
- Expect some clotted blood and mattering of the lids - reassure patient this is normal
- Apply antibiotic ointment (e.g., erythromycin) twice daily until the eye is "back to normal"
- Topical antibiotic three times daily for 5 days after curettage
- If sutures were placed, remove at 5 days
- If bleeding restarts, apply pressure and seek attention if it does not stop
Important Notes
- No sutures are placed inside the eyelid (conjunctival side) - a suture on the inner surface would cause corneal irritation/abrasion
- All excised material (especially recurrent or atypical chalazia) must be sent for histopathology to exclude sebaceous cell carcinoma
- For recurrent cysts, the entire cyst wall may need to be dissected away with scissors, not just curetted
- For marginal chalazia (near the lid margin), steroid injection is often preferred over I&C to avoid structural damage
Sources: Pfenninger & Fowler's Procedures for Primary Care, 3rd ed. | Kanski's Clinical Ophthalmology, 10th ed. | Bailey and Love's Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.