Coronary abnormalities in TGA
Reading File
Finding Sources
Finding Sources
Searching PubMed
"transposition of great arteries" AND "coronary artery" AND anatomy
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced content. Let me compile the full answer.
Coronary Artery Abnormalities in Transposition of the Great Arteries (d-TGA)
Overview
In d-TGA, the coronary arteries arise from the facing sinuses - the two aortic sinuses that face the pulmonary artery. Because the aorta sits anterior-rightward to the pulmonary artery in d-TGA, correct identification of the coronary anatomy is essential before the arterial switch operation (ASO), as transfer of the coronary "buttons" to the neoaorta is the most technically demanding and critical step of the repair.
The Leiden Classification (most widely used)
- Sinus 1 = leftward/anterior facing sinus
- Sinus 2 = rightward/posterior facing sinus
- Coronary branches denoted as: LAD, LCx (Cx), and R (RCA)
Coronary Patterns in d-TGA
Here are the recognized variants, illustrated below:
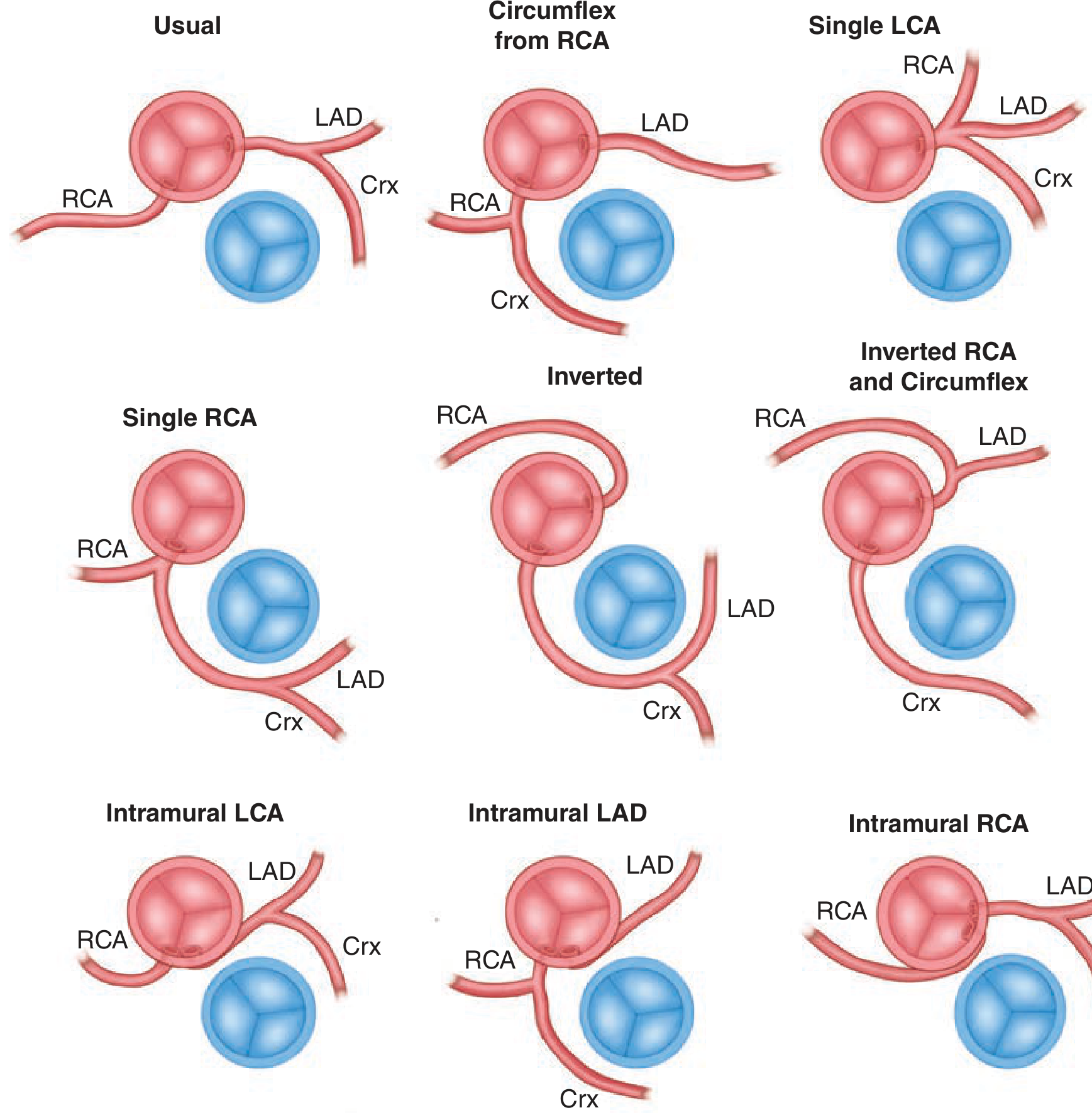
Figure: Different coronary artery patterns in d-TGA. (Fuster and Hurst's The Heart, 15th ed.)
| Pattern | Leiden Notation | Frequency |
|---|---|---|
| Usual - LM from sinus 1 (LAD + Cx), RCA from sinus 2 | 1LCx; 2R | ~67-68% (most common) |
| Circumflex from RCA - LM from sinus 1 gives only LAD; Cx arises from RCA | 1L; 2RCx | ~12% |
| Inverted - RCA + Cx from sinus 1, LAD from sinus 2 | 1RCx; 2L | ~5% |
| Single LCA - all three branches from sinus 1 | 1LRCx or similar | ~3% |
| Single RCA - all branches from sinus 2 | 2LRCx | ~3% |
| Inverted RCA and Circumflex | variant | rare |
The Yacoub and Radley-Smith classification (used in surgical literature) describes five basic patterns (A-E) based on how coronary ostia relate to the aortic and pulmonary valves, with pattern A corresponding to the usual Leiden 1LCx;2R arrangement.
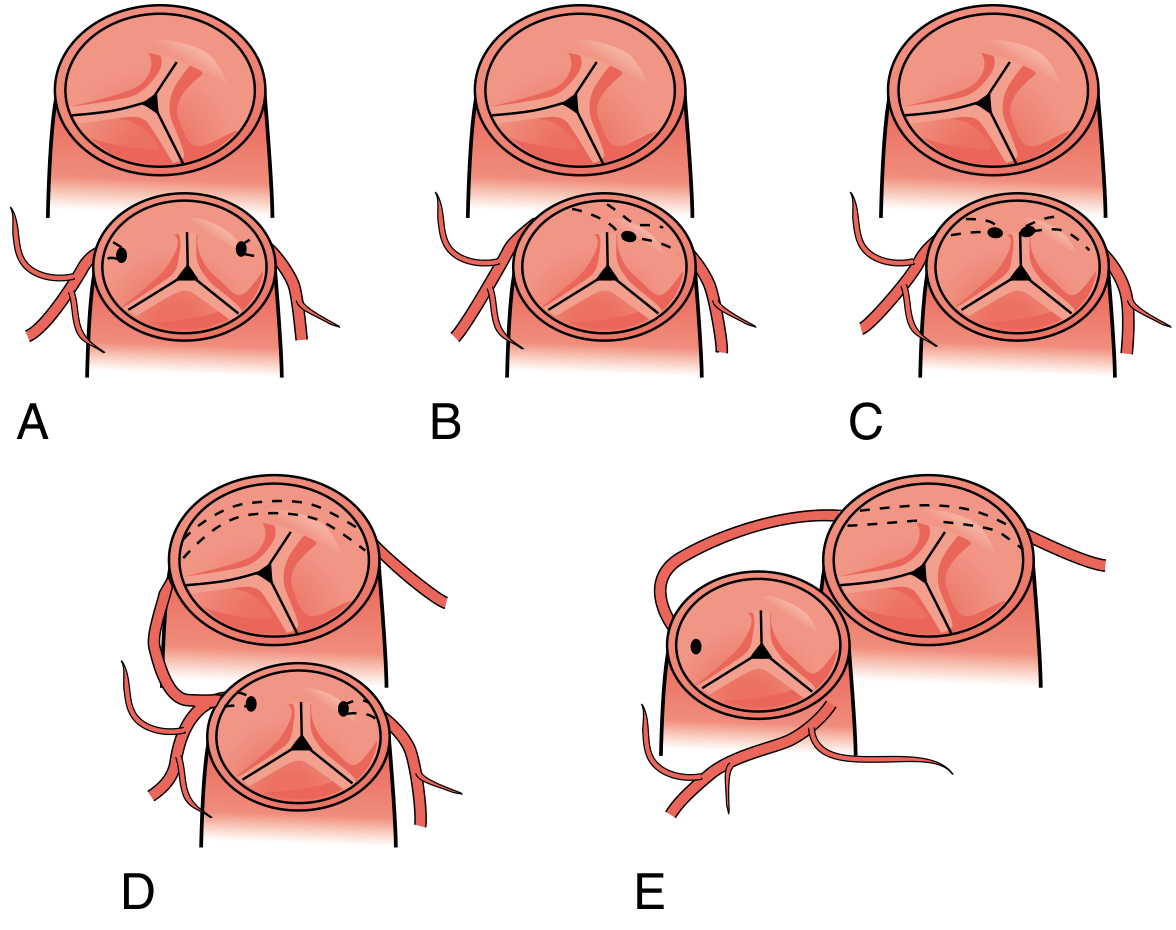
Figure: Five basic coronary configurations (A-E) by Yacoub and Radley-Smith. (Sabiston Textbook of Surgery, 21st ed.)
High-Risk Anatomical Variants
Intramural coronary course (seen in ~3% of cases):
- One coronary runs within the aortic wall (intramural/intramural-interarterial course) between the aorta and pulmonary artery
- Variants: Intramural LCA, Intramural LAD, or Intramural RCA
- Carries significant risk of early sudden cardiac death (SCD)
- Substantially increases surgical mortality of the ASO because the button technique must be modified (unroofing or trap-door technique)
Single coronary ostium (either single LCA or single RCA):
- The entire coronary circulation arises from one ostium
- Technically challenging to transfer during ASO but not a contraindication
- Requires meticulous surgical planning to avoid kinking or tension
Circumflex from RCA (~12%):
- The Cx arises as a branch of the RCA from sinus 2
- Important to recognize because both ostia arise from the same sinus or from the RCA; missing the Cx button is a well-described surgical error
Surgical Implications (Arterial Switch Operation)
Translocation of the coronary arteries is the most technically challenging step of the ASO:
- Both coronary ostia are excised as "buttons" with a rim of aortic wall
- They are reimplanted into the neoaorta (native pulmonary artery root) after the great vessels are transected and switched
- The Lecompte maneuver (anterior translocation of the pulmonary bifurcation) protects the translocated coronary arteries from compression
- Precise anatomic knowledge preoperatively is required for unusual patterns, though ASO is offered to all patients regardless of coronary pattern since techniques exist for every variant
Postoperatively, coronary complications after ASO (stenosis, occlusion, kinking) are a recognized cause of late sudden death and myocardial ischemia in survivors.
Key Teaching Points
- Coronaries always originate from the facing sinuses (adjacent to the PA) in TGA - this is the rule
- The Leiden classification is the standard nomenclature
- The usual pattern (1LCx; 2R) accounts for ~68% of cases
- Intramural course (~3%) is the highest-risk variant due to SCD risk and surgical difficulty
- No coronary pattern is a contraindication to the ASO; surgical technique is adapted accordingly
Sources: Fuster and Hurst's The Heart, 15th ed.; Sabiston Textbook of Surgery, 21st ed.; Braunwald's Heart Disease, 12th ed.
Direction of shunting at atrial ,ventricular and great artery level in TGA
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have excellent content. Now I can compile the full, comprehensive answer.
Direction of Shunting in d-TGA at Each Level
The Core Concept: Parallel Circulations
In normal physiology, the pulmonary and systemic circuits run in series. In d-TGA, they run in parallel - deoxygenated blood recirculates through the systemic circuit and oxygenated blood recirculates through the pulmonary circuit. Life is only possible if there is mixing between the two circuits.
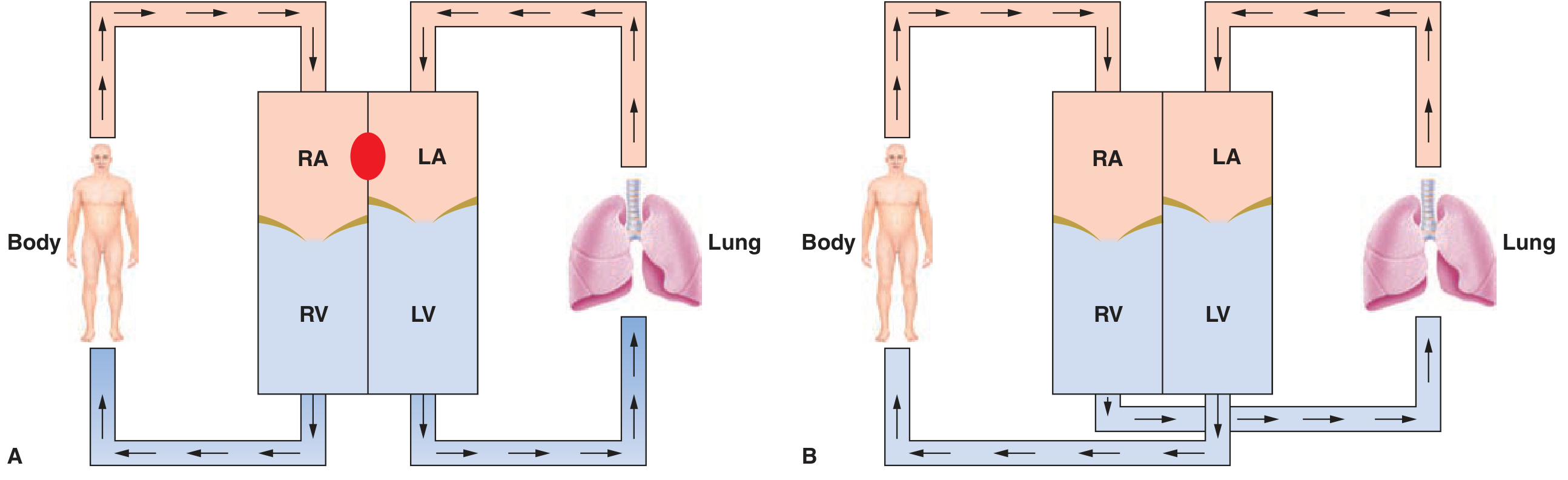
Figure: (A) Parallel circulation in d-TGA - two independent loops. (B) Normal series circulation. (Fuster and Hurst's The Heart, 15th ed.)
Key Principle: Bidirectional (Obligatory) Shunting
At every communication site in TGA, shunting must be bidirectional. This is a thermodynamic necessity:
- For every milliliter of deoxygenated blood that crosses from the systemic circuit to the pulmonary circuit (left-to-right shunt at that site), an equal volume of oxygenated blood must cross in the opposite direction (right-to-left) to maintain net zero blood balance
- This bidirectional obligatory mixing is what sustains systemic oxygenation
- The net shunt at any site depends on the local pressure gradient
Shunt Direction at Each Level
1. Atrial Level (ASD / Patent Foramen Ovale)
| Direction | From → To | Mechanism |
|---|---|---|
| Left → Right | LA → RA | LA pressure > RA pressure (pulmonary circuit is high-flow, high-return) |
| Right → Left | RA → LA | Obligatory bidirectional mixing for survival |
- Net direction: Left-to-Right (LA → RA)
- The left atrium in d-TGA receives well-oxygenated pulmonary venous return and has higher pressure than the RA, because the LV (which pumps to the PA) operates in a lower-resistance pulmonary circuit
- Therefore the dominant direction is L→R at atrial level, but flow is bidirectional
- This is why balloon atrial septostomy (Rashkind procedure) works: it enlarges the interatrial communication to allow more effective mixing. Without it, the neonate develops profound, refractory hypoxemia
- The atrial level is considered the most important mixing site in TGA with intact ventricular septum
2. Ventricular Level (VSD)
| Direction | From → To | Mechanism |
|---|---|---|
| Left → Right | LV → RV | LV (pulmonary) pressure initially < RV (systemic) pressure |
| Right → Left | RV → LV | Obligatory bidirectional component |
- Net direction: Left-to-Right (LV → RV) in most cases
- The LV in d-TGA drives the pulmonary circuit (lower resistance) and therefore has lower pressure than the RV, which drives the high-resistance systemic circuit
- A VSD allows oxygenated blood from the LV to cross into the RV (L→R), which then gets ejected into the aorta - this directly improves systemic oxygenation
- A large non-restrictive VSD produces more effective mixing and less cyanosis compared to intact ventricular septum
- If pulmonary vascular resistance rises (Eisenmenger), the net shunt can reverse to R→L, worsening cyanosis
3. Great Artery Level (PDA)
| Direction | From → To | Mechanism |
|---|---|---|
| Right → Left | Aorta → PA | Aortic (systemic) pressure > PA pressure |
| Left → Right | PA → Aorta | Obligatory bidirectional component |
- Net direction: Right-to-Left (Aorta → PA) - this is the reverse of a PDA in a normal heart
- In d-TGA, the aorta carries deoxygenated systemic venous blood at systemic pressure; the PA carries oxygenated pulmonary venous blood at lower pulmonary pressure
- Therefore the net flow through the ductus is from aorta → pulmonary artery (R→L), sending deoxygenated blood into the pulmonary circuit
- The oxygenated blood in the PA crosses into the aorta as a smaller bidirectional component - this is the beneficial mixing portion
- PGE1 is given to keep the ductus open, maintaining this mixing site until surgical repair
Summary Table
| Level | Communication | Net Shunt Direction | Driving Force | Clinical Significance |
|---|---|---|---|---|
| Atrial | ASD / PFO | L → R (LA → RA) | LA pressure > RA pressure | Most important mixing site; Rashkind BAS enlarges it |
| Ventricular | VSD | L → R (LV → RV) | RV (systemic) pressure > LV (pulmonary) pressure | VSD reduces cyanosis; large VSD = better mixing |
| Great Artery | PDA | R → L (Aorta → PA) | Aortic pressure > PA pressure | Opposite direction to normal PDA; PGE1 keeps it open |
Note: All communications are bidirectional - the "net direction" is the dominant flow. The counter-flow is the effective mixing component that sustains oxygenation.
The Concept of "Effective" Blood Flow
A helpful framework used in congenital cardiology:
- Effective pulmonary blood flow (Qep) = deoxygenated blood that actually reaches the lungs (must cross from systemic → pulmonary circuit)
- Effective systemic blood flow (Qes) = oxygenated blood that actually reaches the body (must cross from pulmonary → systemic circuit)
- In TGA, Qep = Qes (must be equal by conservation of flow)
- The larger these effective flows, the less cyanotic the patient
- A large ASD, VSD, or PDA all increase Qep and Qes, improving oxygenation
Sources: Fuster and Hurst's The Heart, 15th ed.; Sabiston Textbook of Surgery, 21st ed.; Tintinalli's Emergency Medicine; Grainger & Allison's Diagnostic Radiology
Please tell fast
Shunt Direction in d-TGA — Quick Summary
| Level | Net Direction | Why |
|---|---|---|
| Atrial (ASD/PFO) | L → R (LA → RA) | LA pressure > RA pressure |
| Ventricular (VSD) | L → R (LV → RV) | RV pressure > LV pressure (RV pumps to systemic) |
| Great Artery (PDA) | R → L (Aorta → PA) | Aortic pressure > PA pressure — opposite to normal PDA |
Key rule: All shunts are bidirectional (obligatory). The counter-flow is what mixes blood and keeps the baby alive.
PDA in TGA is R→L because the aorta carries deoxygenated blood at high systemic pressure into the low-pressure PA - hence PGE1 is given to keep it open.
Ecg in tga
Finding Sources
Reading File
Reading File
I have everything needed. Here's the concise answer:
ECG in d-TGA
Classic Findings
| Feature | Finding |
|---|---|
| Rate/rhythm | Sinus tachycardia (common in sick neonate) |
| Axis | Right axis deviation |
| Ventricular hypertrophy | Right ventricular hypertrophy (RVH) |
| Atrial | Usually normal; RAE may be present |
Key Points
In a neonate with intact ventricular septum:
- ECG may appear normal for age in the first day or two - because neonatal RV dominance is physiologically normal, so pure RVH blends in
- As systemic RV pressure loads, RVH becomes more evident - tall R in V1, deep S in V5-V6, upright T in V1 beyond the neonatal period
In TGA with VSD:
- Biventricular hypertrophy may be seen, as the LV is also pressure/volume loaded
- If large VSD with pulmonary overcirculation - LVH pattern may appear
Compared to other cyanotic CHDs (quick recall):
| Lesion | Axis | Hypertrophy |
|---|---|---|
| TGA | RAD | RVH |
| Tetralogy of Fallot | RAD | RVH |
| Tricuspid atresia | LAD / Superior axis | LVH |
| TAPVR | RAD | RVH + RAE |
| Truncus arteriosus | Normal/RAD | Biventricular |
The axis + RVH in TGA is non-specific - it is the CXR ("egg on a string" + increased pulmonary markings) combined with the ECG that points toward TGA rather than TOF (which has decreased pulmonary markings).
Source: Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart, 15th ed.
This is a shared conversation. Sign in to Orris to start your own chat.