I want to learn 2 d echo
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have everything I need. Now let me compile a thorough, well-structured guide to learning 2D echocardiography.
A Complete Guide to Learning 2D Echocardiography
Based on the Textbook of Clinical Echocardiography (Otto CM, Elsevier)
1. What is 2D Echocardiography?
2D echocardiography (2D echo) uses a phased-array transducer to electronically sweep an ultrasound beam across a tomographic plane, generating real-time cross-sectional images of the heart at ≥30 frames per second. It is the clinical standard for most cardiac indications - assessing chambers, valves, wall motion, pericardium, great vessels, and more.
2. Ultrasound Physics - The Foundation
Before touching a probe, you need to understand why the image looks the way it does.
Ultrasound Waves
- Sound waves with frequency >20,000 Hz (cardiac probes: 1-8 MHz)
- The fundamental equation: wavelength = speed / frequency (speed in tissue ~1540 m/s)
- Higher frequency = better resolution but less penetration
- Lower frequency = deeper penetration but less resolution
Tissue Interactions
| Interaction | What Happens | Clinical Impact |
|---|---|---|
| Reflection | Wave bounces back at a tissue interface | Creates the image signal |
| Scattering | Irregular reflection from small structures | Creates speckle (grain) |
| Refraction | Beam bends at an interface | Can cause positioning artifacts |
| Attenuation | Signal weakens with depth | Requires time-gain compensation (TGC) |
The Transducer
- Contains piezoelectric crystals that convert electricity to sound and back
- Acts as both transmitter and receiver
- Pulse Repetition Frequency (PRF): how many pulses per second - limited by imaging depth
3. Image Production - How the 2D Picture is Made
A 2D image is built by sweeping the beam line-by-line across the sector:
- A short ultrasound pulse is fired along each scan line
- Reflected signals return to the transducer, with:
- Amplitude proportional to angle of incidence and acoustic impedance difference
- Timing proportional to distance from transducer (depth = time x speed/2)
- Signals undergo amplification, time-gain compensation (TGC), and gray-scale mapping
- All lines are assembled into one image frame
Frame rate vs. quality trade-off:
- More scan lines = better image density but slower frame rate
- Standard: ≥30 frames/second for cardiac motion (128 scan lines at 20 cm depth)
- Cardiac imaging needs high frame rate - do not sacrifice it for width
Key Instrument Controls
| Control | What It Does | How to Optimize |
|---|---|---|
| Frequency | Sets resolution vs. penetration | Use highest frequency that gives adequate depth |
| Gain | Overall image brightness | Avoid over-gain (obscures borders) or under-gain (missed echoes) |
| TGC | Compensates for depth attenuation | Adjust so image is uniformly bright near and far |
| Depth | How deep the image goes | Set just past the structure of interest |
| Sector width | Standard 60° sector angle | Narrow it to increase frame rate when needed |
| Dynamic range | Range of gray shades displayed | Adjust to optimize tissue-to-blood contrast |
4. M-Mode vs. 2D vs. 3D
| Mode | What It Shows | Best For |
|---|---|---|
| M-mode | Depth vs. time along a single line; very high temporal resolution | Valve timing, rapid motion (mitral flutter in AR), precise wall measurements |
| 2D | Real-time cross-sectional tomographic image | Standard clinical imaging, spatial relationships, wall motion |
| 3D | Volumetric dataset; spatial relationships in all planes | Valve anatomy, LV volumes, congenital defects |
2D imaging is the clinical standard - M-mode and 3D are used as supplements.
5. Acoustic Windows - Where You Put the Probe
Acoustic windows are areas where sound can reach the heart without being blocked by bone or lung. There are four main transthoracic windows:
| Window | Patient Position | Key Views Obtained |
|---|---|---|
| Parasternal | Left lateral decubitus | Long-axis (PLAX), short-axis (PSAX), RV inflow/outflow |
| Apical | Steep left lateral decubitus | 4-chamber, 2-chamber, long-axis, 5-chamber |
| Subcostal | Supine, legs slightly bent | 4-chamber, short-axis, IVC view |
| Suprasternal notch | Supine, neck extended | Aortic arch, descending aorta |
6. The Standard Views - Systematic 2D Echo Exam
Parasternal Long-Axis (PLAX)
- Position: Left 3rd-4th intercostal space, adjacent to sternum; patient in left lateral decubitus
- What you see: Aortic valve, mitral valve, LV (basal/mid), LA, proximal ascending aorta, RV outflow tract, pericardium
- Structures NOT seen: Apical LV segments, RV apex
- Key measurements: LV wall thickness, LV internal dimension, aortic root diameter, LA diameter
Parasternal Short-Axis (PSAX)
- Rotate probe 90° clockwise from PLAX
- Sweep from base to apex to visualize different levels:
- Aortic valve level - "Mercedes-Benz" aortic valve, LA, RA, RV, pulmonary valve, MPA
- Mitral valve level - "Fish-mouth" MV opening, LV as circle
- Papillary muscle level - Medial and lateral papillary muscles, LV wall segments
- Apical level - LV tapers to a point
Apical Four-Chamber View (A4C)
- Position: Directly over the LV apex; patient in steep left lateral decubitus
- What you see: All 4 chambers simultaneously, both AV valves, interatrial septum, interventricular septum
- Key uses: LV/RV size and function, mitral/tricuspid valve disease, LV wall motion
- Pitfall: Foreshortening - if the LV looks too spherical, move medially until the true apex is seen
Apical Two-Chamber View (A2C)
- Rotate probe ~60° counterclockwise from A4C
- What you see: LV only (anterior and inferior walls), LA, mitral valve
- Used together with A4C for biplane LV volumes (Simpson's method)
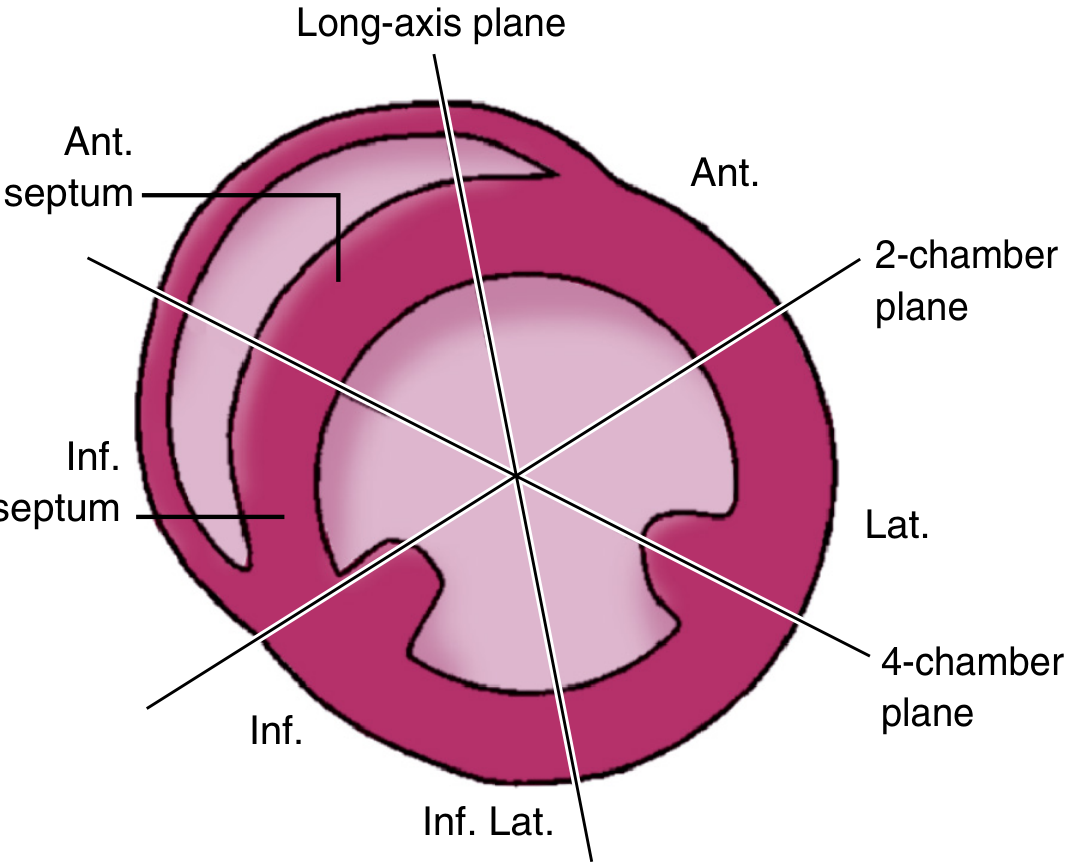
Apical Long-Axis View (A-LAX / Apical 3-Chamber)
- Rotate another ~60° counterclockwise from A2C
- What you see: Aortic valve, mitral valve, LV (inferoseptum and anterolateral wall), LA, aortic root
- Equivalent plane to PLAX but from the apex - confirms PLAX findings
The three apical planes are ~60° apart from each other, as shown below:
Subcostal Views
- Subcostal 4-chamber: Excellent for IAS (best view for detecting ASD), when parasternal/apical windows are poor (COPD, post-surgery)
- Subcostal short-axis: RV, aortic valve, pulmonary valve, IAS
- IVC view: Assess IVC diameter and collapsibility (used to estimate right atrial pressure)
Suprasternal Notch
- Aortic arch anatomy, coarctation assessment, descending aorta Doppler
7. Best Views for Each Structure
| Structure | Best Views |
|---|---|
| Aortic valve | PLAX, PSAX, Apical long-axis |
| Mitral valve | PLAX, PSAX-MV level, A4C, Apical long-axis |
| Pulmonary valve | PSAX (AV level), RV outflow |
| Tricuspid valve | RV inflow, A4C, Subcostal 4-chamber |
| Left ventricle | PLAX, PSAX, A4C, A2C, A-LAX, Subcostal |
| Right ventricle | RV inflow, PSAX, A4C, Subcostal 4-chamber |
| Interatrial septum | PSAX, Subcostal 4-chamber (best) |
| Aortic arch | Suprasternal notch |
| Descending aorta | Suprasternal notch, PLAX (posterior) |
8. Imaging Artifacts - Don't Be Fooled
| Artifact | Cause | How to Recognize |
|---|---|---|
| Reverberation | Multiple reflections between two strong reflectors | Equally spaced repeated lines |
| Side lobe artifact | Energy from outside the main beam | Structure appears in wrong location |
| Shadowing | Calcification or prosthetic material blocks beam | Acoustic shadow behind dense structure |
| Near-field clutter | Strong reflections near transducer | Blurring close to probe |
| Cardiac motion artifact | Heart moves during data acquisition | Blurring of moving borders |
9. What to Assess Systematically on Every Echo
A complete 2D echo examination covers:
- LV size and function - chamber dimensions, wall thickness, regional wall motion, ejection fraction
- RV size and function - RV/LV ratio, wall motion, TAPSE
- LA and RA size - chamber dimensions
- Aortic valve - leaflet number, thickening/calcification, opening, any stenosis/regurgitation signs
- Mitral valve - leaflet morphology, motion, prolapse, rheumatic changes
- Tricuspid and pulmonary valves
- Pericardium - effusion (size, location), tamponade signs (RA/RV collapse)
- Aorta - root and ascending diameter, arch
- IVC - diameter and respiratory variation (RA pressure estimation)
10. Key Measurements (Normal Values)
| Measurement | Normal Range |
|---|---|
| LV internal dimension (diastole) | ≤5.6 cm (men), ≤5.2 cm (women) |
| LV wall thickness (IVS/PW) | 0.6-1.0 cm |
| Ejection fraction (biplane) | ≥55% |
| LA diameter (PLAX) | ≤4.0 cm (men), ≤3.8 cm (women) |
| Aortic root (sinus of Valsalva) | ≤4.0 cm (men), ≤3.6 cm (women) |
| IVC diameter | ≤2.1 cm (collapses >50% with sniff = RA pressure ≤5 mmHg) |
11. How to Learn - Practical Pathway
Step 1 - Master physics first (1-2 weeks)
Read the physics chapter of a dedicated echo textbook. Understand why artifacts happen.
Step 2 - Learn normal anatomy in each view (2-4 weeks)
Use the standard views systematically. Always start PLAX → PSAX → Apical → Subcostal.
Step 3 - Perform supervised scans (ongoing)
No substitute for hands-on practice. The apical window is the hardest to find in most patients - practice positioning.
Step 4 - Learn pathology view-by-view
Aortic stenosis, mitral regurgitation, LV dysfunction, pericardial effusion - learn how each appears on 2D.
Step 5 - Add Doppler (pulsed-wave, continuous-wave, color, tissue Doppler)
2D gives structure; Doppler gives function and hemodynamics.
Resources
- Textbook of Clinical Echocardiography by Catherine M. Otto (Elsevier) - the gold standard reference used above
- American Society of Echocardiography (ASE) guidelines: aseuniversity.org - free online guidelines with images
- EchoFirst app and online simulators for self-study of views
Summary: Start with physics → understand how the image is made → learn the 4 acoustic windows → master the standard views (PLAX, PSAX at 3 levels, A4C, A2C, A-LAX, subcostal) → practice systematically on every patient → add Doppler last.
- Textbook of Clinical Echocardiography (Otto CM, Elsevier, 9780323882088)
Complete practical views and steps and what to use like ow and cw and when how tell report and values
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
This is the complete practical 2D echo guide. Here's a summary of what's covered:
What this guide covers:
Part 1 - The Doppler Toolkit
- PW Doppler: Range-specific, low velocities - mitral inflow, LVOT VTI, pulmonary veins. Max ~1 m/s at 6 cm
- CW Doppler: No range limit, high velocities - aortic stenosis, TR jet for PASP, MR for dP/dt. Uses ΔP = 4V²
- Color Doppler: Shows WHERE flow is going, screens for regurgitation, guides CW beam alignment
- Tissue Doppler: Measures myocardial motion at the annulus - e', s', a' - key for diastolic function (E/e' ratio)
Part 2 - Step-by-step exam (PLAX → PSAX 3 levels → A4C → A2C → A-LAX → Subcostal → Suprasternal) with what 2D, color, PW, and CW to do at each window
Part 3 - Calculations - Simpson's EF, CO/SV formula, diastolic grading (4-variable algorithm), PASP, AS grading (continuity equation), MS (PHT), MR (PISA/vena contracta), RV function (TAPSE)
Part 4 - Report writing - full template with example language for each section
Part 5 - Normal values quick card - all chambers, Doppler values, pressures in one table
Part 6 - Which Doppler quick decision chart
Complete practical views of adult echo with steps of toolbkit use in every view with images and steps and what to use like ow and cw and when how tell report and values
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
This is the complete illustrated practical guide. Here's what it covers:
12 standard views with anatomy images + step-by-step Doppler toolkit for each:
| View | Key Toolkit Steps |
|---|---|
| PLAX | M-mode dimensions, Color for AR/MR, LVOT diameter measurement |
| RV Inflow | CW for TR jet → PASP calculation |
| PSAX-AV | 2D for AV cusp number, Color + PW for pulmonary valve |
| PSAX-MV | 2D "fish-mouth" opening, planimetry MVA in stenosis |
| PSAX-PM | 6-segment wall motion analysis, D-sign for RV overload |
| A4C | Biplane EF, PW mitral inflow, PW pulmonary vein, TDI e'/s', CW TR, TAPSE |
| A2C | Biplane EF pair with A4C, inferior/anterior wall |
| A-LAX | PW LVOT VTI, CW aortic stenosis + AR PHT, continuity equation AVA |
| A5C | Best CW alignment for AS |
| Subcostal 4C | Color for ASD/PFO (IAS perpendicular to beam) |
| Subcostal IVC | IVC diameter + sniff test → RA pressure table |
| Suprasternal | Aortic arch, coarctation, AR holodiastolic reversal |
Plus: PW sample volume locations table, CW calculation table, diastolic function 4-criteria algorithm with grading, full echo report template you can use directly, and complete normal values quick-reference card.
How to check Aorta value Pjv Ajv And tapse Mitral E/a values how to check?
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.