Ultrasound scan for kidney
Reading File
Finding Sources
Finding Sources
Searching the Web
kidney renal ultrasound scan normal findings indications technique 2024
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have comprehensive, authoritative content to write a thorough answer. Let me compile everything.
Kidney Ultrasound (Renal Sonography)
Ultrasound is the first-line imaging modality for the kidney - it is non-invasive, radiation-free, widely available, and provides real-time structural information. Here is a complete overview.
Indications
Renal ultrasound is used to evaluate:
- Acute kidney injury (AKI) - to exclude urinary obstruction as a cause
- Chronic kidney disease (CKD) - assess kidney size, echogenicity, and chronicity
- Hydronephrosis - grading and identifying the level of obstruction
- Renal colic / suspected stones - detect nephrolithiasis
- Urinary tract infection (UTI) - especially in children; detect congenital anomalies, abscess, or pyonephrosis
- Haematuria - detect masses, cysts, or stones
- Hypertension - evaluate kidney size and detect renal artery abnormalities
- Transplant kidney - monitor for rejection, perinephric collections, and vascular complications
- Guidance for biopsy and percutaneous procedures
(Comprehensive Clinical Nephrology, 7th Ed.)
Technique
Probe and Patient Position
- A curvilinear (convex) transducer is the standard choice. A phased array probe can be used as a substitute but offers inferior parenchymal detail.
- Patient is typically supine, though lateral decubitus, oblique, or prone positions may be needed (especially for the left kidney, where overlying bowel gas is a challenge).
- Acoustic windows:
- Right kidney - imaged through the liver
- Left kidney - imaged through the spleen
- This avoids bowel gas interference.
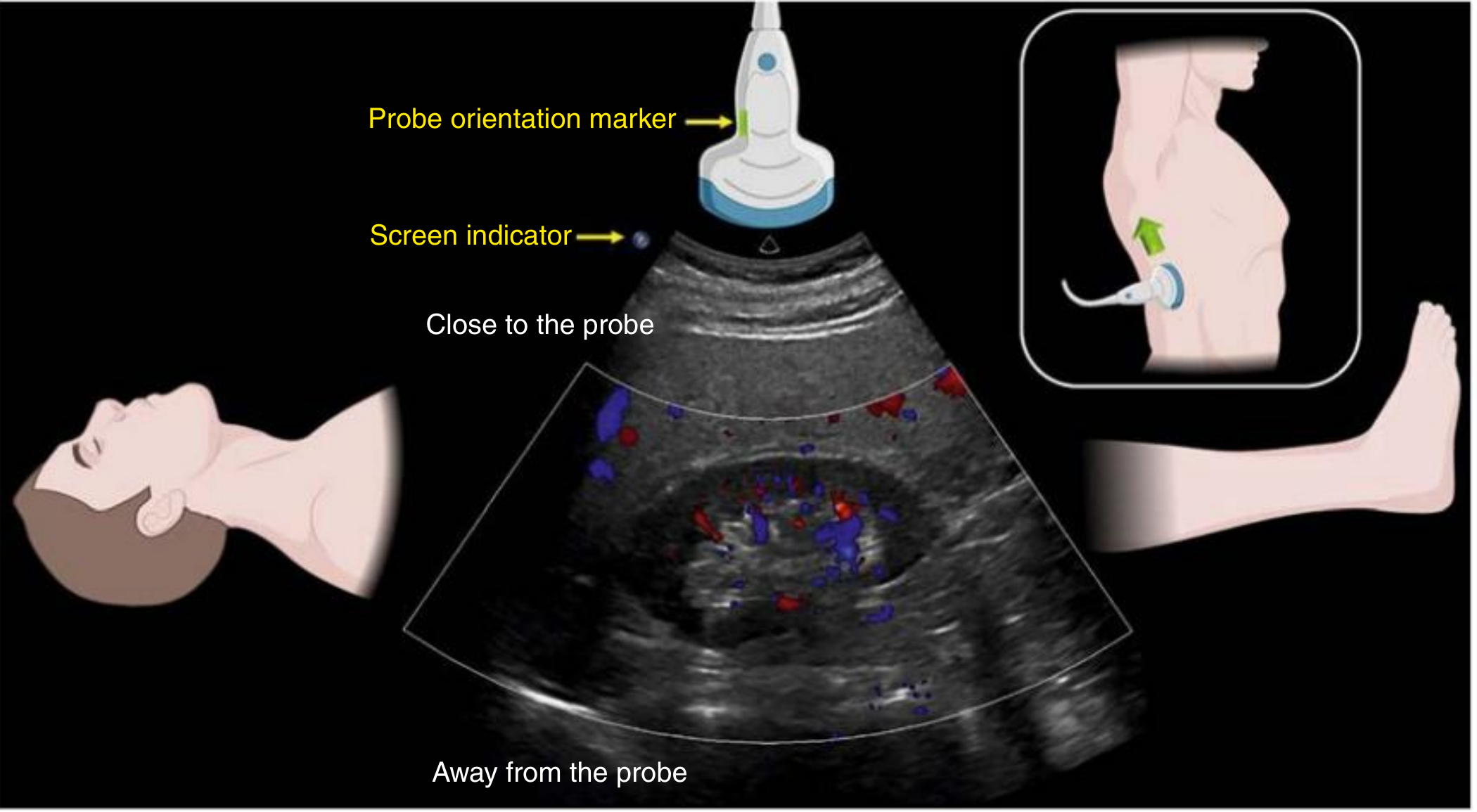
Probe Positioning
- Place the transducer in the mid- or anterior axillary line at the 10th rib interspace, orientation marker pointing toward the patient's head, angled slightly posteriorly.
- Fan (tilt) anteriorly and posteriorly to image the kidney completely in longitudinal view.
- Rotate 90 degrees counterclockwise for the short axis (transverse) view, then fan superiorly and inferiorly to image from pole to pole.
- Color Doppler should always be added for global perfusion assessment and to differentiate vascular structures from dilated collecting systems.
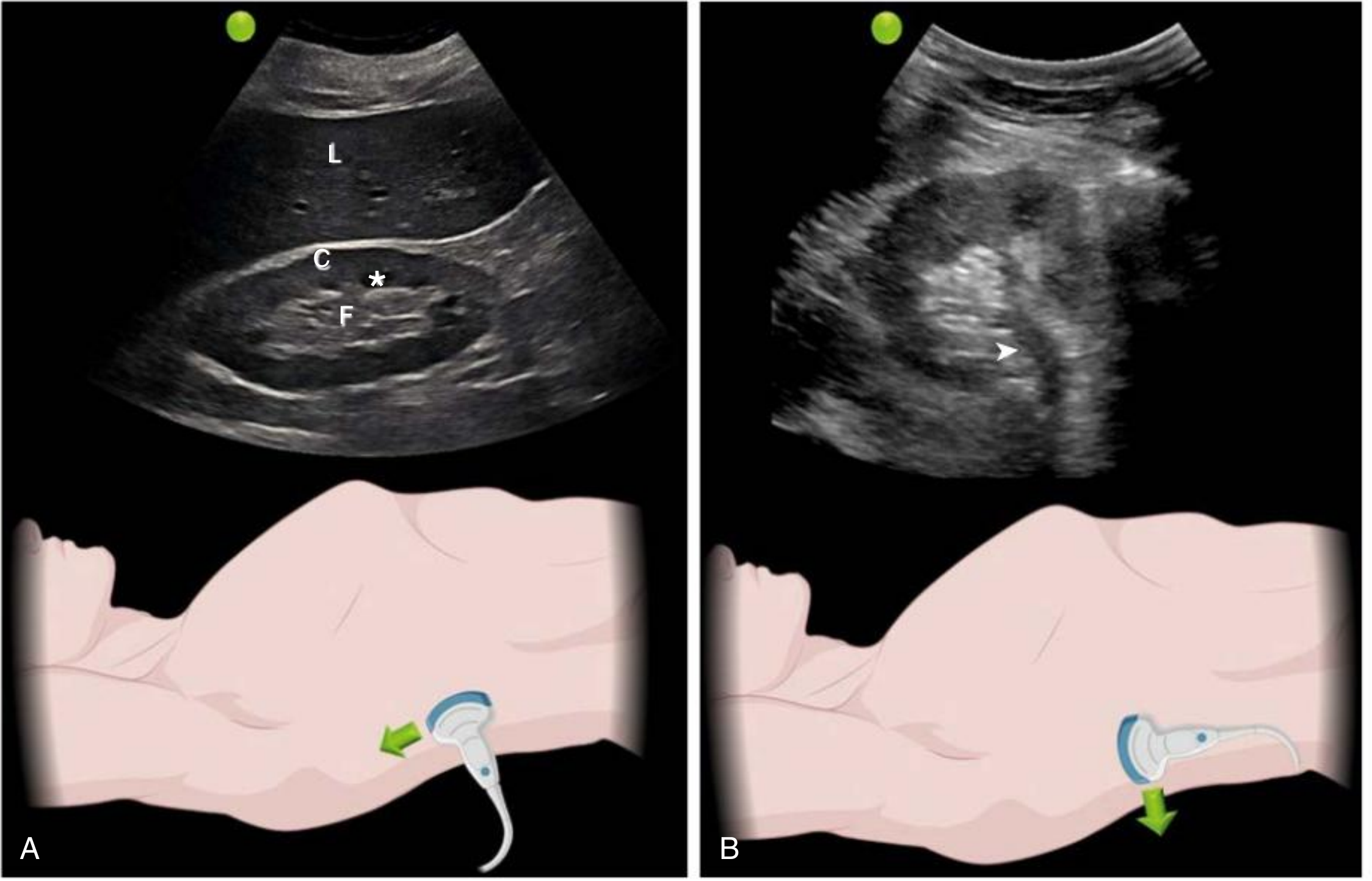
Normal Sonographic Appearances
| Feature | Normal Finding |
|---|---|
| Shape | Well-defined, bean-shaped with echogenic capsule |
| Size | 9-12 cm in longitudinal plane (varies with body height) |
| Cortex | Hypoechoic or isoechoic relative to liver/spleen |
| Medullary pyramids | Anechoic or hypoechoic compared to cortex; prominent in children |
| Columns of Bertin | Cortical tissue separating pyramids (can hypertrophy and mimic a mass) |
| Sinus fat | Echogenic; occupies inner kidney; encases collecting system |
| Collecting system | Not visible when undilated; any anechoic area in sinus fat raises suspicion for hydronephrosis |
| Transverse (short axis) view | C-shaped at midportion; circular at poles |
Key Pathological Findings
1. Hydronephrosis
Appears as anechoic branching, interconnected areas in the collecting system (backlogged urine).
| Grade | Features |
|---|---|
| Mild | Dilation of renal pelvis and calyces; parenchymal architecture intact |
| Moderate | Medullary pyramids begin to flatten; increasing pelvicalyceal dilation |
| Severe | Ballooned pelvis and calyces; corticomedullary differentiation lost; thin parenchyma |
- If internal echoes are present within the hydronephrotic area → consider pyonephrosis (pus in the collecting system), especially with fever and flank pain.
- Pitfall: Color Doppler differentiates blood vessels (show flow) from hydronephrosis (no flow). Parapelvic cysts can mimic hydronephrosis but are round, well-circumscribed, and not connected to the ureter.
2. Kidney Stones (Nephrolithiasis)
- Appear as hyperechoic structures with posterior acoustic shadow (signal void beyond the stone).
- On color Doppler: exhibit the "twinkling sign" - a rapidly alternating color Doppler signal that is more pronounced with rough-surfaced stones.
3. Echogenicity Changes (CKD / AKI)
- Normal cortex is hypoechoic compared to liver.
- Increased cortical echogenicity (cortex brighter than liver) = parenchymal disease (CKD, glomerulonephritis, diabetic nephropathy, etc.)
- In CKD: kidneys become small and echogenic, with loss of corticomedullary differentiation.
- In AKI: kidneys are often normal or slightly enlarged; echogenicity alone cannot distinguish cause.
4. Renal Cysts
- Appear as smooth, round, anechoic structures with posterior acoustic enhancement.
- Simple cysts: thin walls, no internal echoes = benign.
- Complex cysts: internal echoes, septations, or thick walls = require further evaluation (CT or MRI).
5. Masses
- Solid renal masses appear as hyper- or isoechoic lesions disturbing normal architecture.
- Ultrasound is a screening tool; CT or MRI is needed for characterization.
6. Renal Vein Thrombosis
- Kidney enlargement, loss of corticomedullary differentiation, linear echogenicity radiating from the renal hilum (from venous clot).
- Doppler shows absent or reversed diastolic flow.
Doppler Assessment
| Application | Finding |
|---|---|
| Color Doppler | Global perfusion; differentiates vessels from hydronephrosis/cysts |
| Spectral Doppler (RI) | Resistive Index (RI) = (Peak systolic velocity - End diastolic velocity) / Peak systolic velocity |
| Normal RI | < 0.70 |
| Elevated RI (>0.70) | Suggests obstruction, rejection (transplant), or parenchymal disease |
| Renal artery stenosis | Peak systolic velocity > 180-200 cm/s at stenosis; dampened waveform ("tardus-parvus") distally |
Limitations of Renal Ultrasound
- Operator-dependent - image quality and interpretation vary with experience.
- Bowel gas - can obscure the left kidney.
- Body habitus - difficult in obese patients.
- Not sensitive for acute pyelonephritis - abnormalities found in only 20-69% vs. 40-92% with DMSA scintigraphy.
- Not diagnostic for vesicoureteral reflux (VUR) or kidney scarring.
- False negatives for hydronephrosis - can occur with acute/partial obstruction, volume depletion, or retroperitoneal fibrosis.
- Cannot assess function - functional studies (DMSA, MAG3 scintigraphy) or GFR measurement needed for functional information.
Clinical Decision Points
| Clinical Question | Role of Ultrasound |
|---|---|
| AKI - is it obstructive? | Rule out hydronephrosis (high sensitivity) |
| CKD - how chronic? | Small, echogenic kidneys = chronic; normal size with AKI = acute |
| Renal colic | Detect stones and hydronephrosis; CT KUB more sensitive for small stones |
| Haematuria | Screen for mass, cyst, stone |
| Paediatric UTI | Detect congenital anomalies (CAKUT), abscess, pyonephrosis |
| Transplant monitoring | Perinephric collections, Doppler for rejection |
| Pre-biopsy | Confirm kidney position, size, and guide needle placement |
Sources: Comprehensive Clinical Nephrology, 7th Edition (Chapter 5 - Kidney and Bladder Ultrasound, p. 80-82); Brenner and Rector's The Kidney, 2-Volume Set (Imaging Tests chapter)
This is a shared conversation. Sign in to Orris to start your own chat.