Renal failure
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive material for a full in-depth clinical review. Here is the complete answer:
Renal Failure: Types, Causes, and Pathophysiology
1. Terminology and Definition
The term acute renal failure (ARF) has been largely replaced by acute kidney injury (AKI), defined as an abrupt decline in glomerular filtration rate (GFR) sufficient to decrease elimination of nitrogenous waste products and uremic toxins. Standardized KDIGO definitions stage AKI based on the magnitude of serum creatinine rise and changes in urine output over 1 week. The broader umbrella term renal failure encompasses both acute and chronic forms.
- Comprehensive Clinical Nephrology, 7th Edition, p. 921
2. Classification: The Three-Category Framework
Renal failure is universally classified into three pathophysiologic categories:
| Category | Mechanism | Urine Na | Urine Osmolality |
|---|---|---|---|
| Prerenal | Reduced renal perfusion | <20 mmol/L | >500 mOsm/kg |
| Intrinsic | Direct parenchymal damage | >40 mmol/L | ~300 mOsm/kg (isosthenuria) |
| Postrenal | Urinary tract obstruction | Variable | Variable |
- Brenner and Rector's The Kidney, p. 2147; Tintinalli's Emergency Medicine, p. 1831
3. Prerenal AKI (40-55% of all AKI)
Prerenal azotemia is the most common form, accounting for 40-55% of all AKI cases.
Causes
- Absolute volume depletion: GI losses (diarrhea, vomiting, nasogastric suction), renal losses (overdiuresis, diabetes insipidus), third spacing (acute pancreatitis, burns)
- Effective intravascular volume contraction: Heart failure, liver failure, nephrotic syndrome - in these states absolute blood volume may be increased but arterial blood flow to kidneys is reduced
- Impaired renal autoregulation: NSAIDs block afferent arteriolar vasodilation; ACE inhibitors/ARBs block efferent vasoconstriction (angiotensin II) - both precipitate AKI under conditions of reduced perfusion
Pathophysiology
With moderate hypoperfusion, GFR is initially maintained by:
- Afferent arteriolar vasodilation (mediated by vasodilatory eicosanoids)
- Efferent arteriolar vasoconstriction (mediated by angiotensin II), increasing filtration fraction
When perfusion falls below the autoregulatory threshold, glomerular capillary filtration pressure drops and GFR falls. Tubular function remains intact - the kidney responds by avidly reabsorbing sodium and water, producing concentrated urine with low urinary sodium.
- Comprehensive Clinical Nephrology, 7th Edition, p. 930
4. Intrinsic AKI
Intrinsic AKI is categorized by the anatomic location of primary renal injury:
4a. Acute Tubular Necrosis (ATN) - most common intrinsic cause
Causes are broadly:
- Ischemic ATN: Prolonged prerenal azotemia or hypotension; even brief hypotension can cause tubular epithelial cell necrosis
- Septic ATN: Now recognized as having a complex pathogenesis beyond simple ischemia-reperfusion; may develop without overt hypotension
- Nephrotoxic ATN:
- Extrinsic: Iodinated contrast agents, aminoglycoside antibiotics, vancomycin, NSAIDs, chemotherapy (cisplatin, ifosfamide)
- Intrinsic: Myoglobin (rhabdomyolysis), hemoglobin (hemolysis), intratubular crystals (uric acid, oxalate, drug crystals)
Note: "ATN" is technically a misnomer - true cellular necrosis is often minimal in human disease. "Acute tubular injury (ATI)" is the preferred modern term.
Pathophysiology of ATN - Four Mechanisms
1. Vascular dysregulation: Ischemia causes loss of autoregulation with intense intrarenal vasoconstriction, reducing GFR directly.
2. Tubular obstruction: Sloughed epithelial cells and debris form casts that obstruct the tubular lumen, increasing intratubular pressure and opposing filtration.
3. Tubular cell injury: ATP depletion during ischemia disrupts Na/K-ATPase, causes cytoskeletal disassembly, and leads to cell swelling, loss of polarity, and cell death (apoptosis and necrosis).
4. Back-leak: Loss of adhesion molecules (E-cadherin) and tight junction proteins (ZO-1, occludin) allows filtrate to leak back into the renal interstitium, reducing measured GFR. In severe ATI, back-leak may account for up to 50% of GFR reduction.
Key Sites of Vulnerability
The diagram below shows why the S3 segment of the proximal tubule and the medullary thick ascending limb (mTAL) are most vulnerable to ischemic injury:
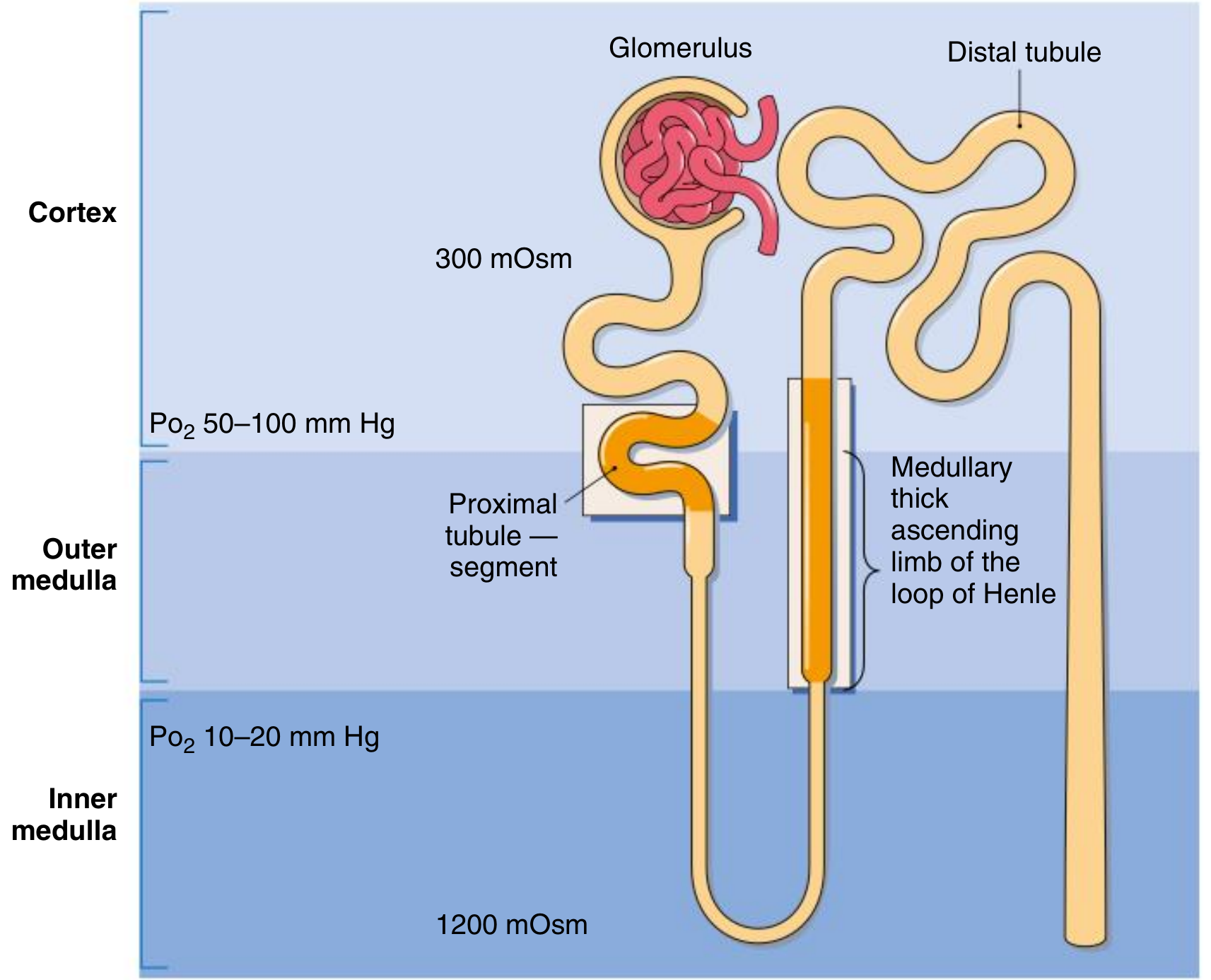
The outer medulla operates at a PO2 of only 10-20 mmHg, while these tubular segments have very high metabolic demands. This combination of borderline oxygen supply + high energy requirements makes them exquisitely sensitive to ischemia.
- Comprehensive Clinical Nephrology, 7th Edition, p. 1037-1059
4b. Endothelial Cell Injury
Ischemia and oxidant stress damage peritubular capillary (vasa rectae) endothelial cells, causing:
- Upregulation of adhesion molecules
- Recruitment of neutrophils and monocytes
- Decreased endothelial nitric oxide synthase → impaired vasodilation
- Peritubular congestion and interstitial edema → exacerbated hypoxia in the outer medulla
4c. Inflammatory Mechanisms
Both innate and adaptive immunity contribute:
- TLR2 and TLR4 are upregulated in the ischemic kidney, activated by danger-associated molecular patterns (DAMPs)
- Complement activation (predominantly alternative pathway) produces proinflammatory cytokines: TNF-alpha, IL-6, IL-1beta
- Neutrophil activation releases proteases and reactive oxygen species (ROS)
- A network of renal dendritic cells shapes the inflammatory response
4d. Vascular Causes
- Large vessel: Renal artery/vein thrombosis (uncommon)
- Atheroembolic disease: After aortic instrumentation
- Small vessel: Vasculitis, thrombotic microangiopathy (HUS/TTP), malignant hypertension, scleroderma renal crisis, DIC, eclampsia
4e. Glomerular Causes
All forms of acute glomerulonephritis can present as AKI (rapidly progressive GN, anti-GBM disease, ANCA vasculitis, lupus nephritis).
4f. Interstitial Causes
Acute Interstitial Nephritis (AIN) - most often allergic/drug-induced:
- Antibiotics (penicillins, cephalosporins, sulfonamides, quinolones)
- NSAIDs
- Proton pump inhibitors (more recently recognized)
- Systemic signs: fever, rash, eosinophilia (especially with antibiotics; often absent with NSAIDs)
5. Postrenal AKI
Obstruction can occur anywhere from the renal collecting system to the urethra. Bilateral obstruction (or unilateral in a solitary kidney) is required to produce significant AKI.
Common Causes
- Bladder outlet obstruction: BPH (most common in older men), urethral stricture, neurogenic bladder
- Bilateral ureteric obstruction: Retroperitoneal fibrosis, pelvic malignancy, bilateral calculi
- Intrarenal obstruction: Crystal nephropathy (uric acid, acyclovir, methotrexate)
Diagnosis
Renal ultrasound - detects hydronephrosis and hydroureter. Placement of a urinary catheter is both diagnostic and therapeutic for bladder outlet obstruction.
6. Chronic Kidney Disease (CKD)
CKD is defined as abnormalities of kidney structure or function present for at least 3 months with implications for health.
KDIGO CGA Staging
Classification is based on three dimensions: Cause, GFR category, and Albuminuria (the "CGA" staging framework):
| GFR Stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal or high (with other markers of CKD) |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mildly to moderately decreased |
| G3b | 30-44 | Moderately to severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | <15 | Kidney failure (ESKD) |
eGFR is estimated using the CKD-EPI equation (the MDRD equation has been replaced). The updated CKD-EPI formula eliminates race as a variable.
| Albuminuria Stage | AER (mg/24 h) | ACR (mg/mmol) |
|---|---|---|
| A1 | <30 | <3 |
| A2 | 30-300 | 3-30 |
| A3 | >300 | >30 |
Clinical Presentation
CKD is usually asymptomatic until late stage G4-G5. Symptoms are non-specific: fatigue, nocturia, pruritus, anorexia, nausea. Physical exam findings suggesting chronicity include skin pigmentation, scratch marks, LVH, and hypertensive fundal changes.
Common Risk Groups for CKD Screening
Diabetes, hypertension, prior AKI, cardiovascular disease, structural kidney disease, multisystem diseases (SLE), family history of ESKD, hereditary kidney disease.
- Comprehensive Clinical Nephrology, 7th Edition, p. 3674-3691
7. Acute-on-Chronic Kidney Disease
A clinically important pattern is AKI superimposed on pre-existing CKD ("acute-on-chronic kidney disease"). Among inpatients, prerenal azotemia and ATI (ATN) account for most AKI cases, often in this setting.
The KDIGO workgroup has also proposed the concept of Acute Kidney Disease (AKD) for conditions with a more subacute onset - kidney dysfunction lasting more than 7 days but less than 3 months.
8. Key Diagnostic Parameters Summary
| Parameter | Prerenal | ATN (Intrinsic) | Postrenal |
|---|---|---|---|
| Urine Na (mmol/L) | <20 | >40 | Variable |
| FENa | <1% | >2% | Variable |
| Urine osmolality | >500 | ~300 (isosthenuria) | Variable |
| Urine sediment | Bland/hyaline casts | Granular/muddy brown casts, RTECs | Variable |
| Response to fluids | Rapid improvement | No improvement | Variable |
FENa = (urine Na × plasma Cr) / (plasma Na × urine Cr) × 100
Exception: FENa <1% can occur in intrinsic AKI due to contrast nephropathy, early obstruction, myoglobinuria, and glomerulonephritis - clinical context is essential.
Sources: Comprehensive Clinical Nephrology, 7th Edition; Brenner and Rector's The Kidney, 2-Volume Set; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.