Tell me everything about pneumonia and how it occurs and what are the effects in body and the treatment that is followed for it and days of recovery just like you're telling a doctor
Reading File
Finding Sources
Finding Sources
Searching PubMed
pneumonia management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
pneumonia lung consolidation chest X-ray histology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Goldman-Cecil Medicine, Fishman's Pulmonary Diseases, Robbins Pathology, Murray & Nadel's Respiratory Medicine, and Rosen's Emergency Medicine. Let me synthesize the complete clinical answer.
Pneumonia: A Comprehensive Clinical Overview
1. Definition
Pneumonia is acute infection of the lung parenchyma associated with at least one respiratory symptom (cough, dyspnea, pleuritic chest pain) and abnormal opacities on lung imaging, with or without fever, in the absence of an alternative diagnosis. It represents the most common infectious cause of hospitalization and death in the United States. — Goldman-Cecil Medicine, p. 990
2. Classification
| Category | Definition | Typical Pathogens |
|---|---|---|
| CAP (Community-Acquired) | Acquired outside hospital / within 48h of admission | S. pneumoniae, H. influenzae, Mycoplasma, Legionella, viruses |
| HAP (Hospital-Acquired) | ≥48h after hospitalization | S. aureus (MRSA), Gram-negative bacilli (Pseudomonas, Acinetobacter) |
| VAP (Ventilator-Associated) | ≥48–72h after endotracheal intubation | Same as HAP, often more resistant |
| Aspiration Pneumonia | Macro- or microaspiration of oropharyngeal contents | Anaerobes, mixed oral flora |
| Pneumonia in immunocompromised | HIV, transplant, neutropenic patients | All of above + PCP, Cryptococcus, CMV, Aspergillus |
3. Epidemiology
- CAP accounts for 7 annual healthcare visits/1000 young adults but 96 visits/1000 adults ≥85 years — exponential increase with age
- Hospitalization rates: ~1–2/1000 in young adults → 40/1000 in those ≥85 years
- Seasonal peak: November–March (coincides with influenza and other respiratory viral surges)
- ~35% of CAP hospitalizations in the U.S. involve patients with recent healthcare exposure; ~25% have immunocompromising conditions
- Goldman-Cecil Medicine, p. 990
4. Etiology & Common Pathogens
Bacterial (most common causes of severe CAP)
| Organism | Notes |
|---|---|
| Streptococcus pneumoniae | Most common bacterial cause overall; lobar pattern; bacteremia in 25–30% |
| Haemophilus influenzae | COPD exacerbations; non-typeable strains |
| Moraxella catarrhalis | Mostly in COPD patients |
| Staphylococcus aureus | Post-influenza; MRSA causes necrotizing pneumonia |
| Klebsiella pneumoniae | Debilitated/malnourished/"currant jelly sputum"; lobar upper-lobe pattern |
| Legionella pneumophila | Organ transplant recipients, water systems; hyponatremia, diarrhea |
| Mycoplasma pneumoniae | "Walking pneumonia" in ages >5y; self-limited; extrapulmonary features |
| Chlamydophila pneumoniae | Atypical; gradual onset |
| Pseudomonas aeruginosa | Cystic fibrosis, burn patients, neutropenia; bilateral bronchopneumonia |
Viral (up to 90% of pediatric pneumonias)
- SARS-CoV-2 (COVID-19), Influenza A/B, RSV, Human metapneumovirus, Parainfluenza, Adenovirus
- Characterized by inflammation predominantly confined to alveolar septa, with respiratory distress often out of proportion to radiologic signs
- Robbins & Kumar Basic Pathology, p. 497
5. Pathogenesis — How Pneumonia Occurs
Step 1: Breach of Host Defenses
The lung is protected by multiple layers: nasal hair, mucociliary escalator, cough reflex, alveolar macrophages, secretory IgA, and surfactant. Pneumonia occurs when these are overwhelmed by:
- High inoculum (aspiration)
- Highly virulent organisms (S. pneumoniae capsule evades phagocytosis)
- Impaired host defenses (viral infection→ epithelial damage; smoking; immunosuppression; intubation bypassing upper airway)
Step 2: Microbial Invasion of Alveolar Space
Once pathogens reach the alveoli, they trigger the innate immune response:
- Pattern recognition receptors (TLRs) recognize bacterial PAMPs
- Pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-8) are released
- Massive neutrophil recruitment ensues
- The alveolar capillary membrane is disrupted → exudative fluid fills alveoli
Step 3: Morphologic Stages of Lobar Pneumonia (Robbins Pathology)
Classic four stages of bacterial lobar consolidation:
| Stage | Timing | Pathology |
|---|---|---|
| 1. Congestion | Day 1–2 | Vascular engorgement, serous exudate, few bacteria; lung heavy and red |
| 2. Red Hepatization | Day 2–4 | Massive neutrophil + RBC + fibrin exudate; lung "liver-like" in consistency; red/airless |
| 3. Gray Hepatization | Day 4–8 | RBC lysis; macrophage predominance; fibrinous exudate persists; lung gray |
| 4. Resolution | Day 8+ | Enzymatic digestion of exudate; macrophages clear debris; normal architecture restored |
Bronchopneumonia (patchy pattern): multifocal alveolar consolidation centered around bronchioles — S. aureus, H. influenzae, Pseudomonas, Klebsiella
Robbins & Kumar Basic Pathology, p. 497
6. Physiological Effects on the Body
Pulmonary Effects
Gas Exchange Failure — the central pathophysiological mechanism:
- Consolidated alveoli receive blood flow but contain no air → true intrapulmonary shunt (perfusion without ventilation)
- In mild-moderate pneumonia: shunt fraction ~7.5%, low V/Q regions ~4.2% → mild hypoxemia (PaO₂ ~74 mmHg)
- In severe pneumonia requiring mechanical ventilation: shunt fraction rises to ~21.9%, low V/Q regions to ~10.9%
- As consolidation worsens, both shunt and low V/Q areas increase; the greater the shunt fraction, the poorer the response to supplemental O₂
- Murray & Nadel's Respiratory Medicine (MIGET studies)
Systemic Inflammatory Response
- Bacteremia in 10–25% (especially S. pneumoniae)
- Sepsis → systemic vasodilation, third-spacing, hypotension, end-organ hypoperfusion
- SIRS criteria frequently met: fever/hypothermia, tachycardia, tachypnea, leukocytosis/leukopenia
- Progression to septic shock in ~5–10% of hospitalized CAP
Cardiac Complications
Critically underrecognized: nearly 25% of hospitalized CAP patients experience at least one new cardiovascular event within the first 3 days:
- Decompensated heart failure
- New atrial fibrillation or flutter
- Acute coronary syndrome (demand ischemia from hypoxia + inflammation)
- Stroke
- Goldman-Cecil Medicine, p. 991 (Prognosis section)
Pulmonary Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion | Exudative pleural effusion in ~40% of bacterial pneumonia |
| Empyema thoracis | Infected pleural fluid; requires drainage; especially S. pyogenes (30–40%) |
| Lung abscess | Cavitation; especially Klebsiella, anaerobes, S. aureus |
| ARDS | Bilateral infiltrates, PaO₂/FiO₂ <300; life-threatening; occurs with severe pneumococcal/MRSA/Gram-neg |
| Pneumothorax | Especially with Pneumocystis, necrotizing infections |
| Organizing pneumonia | Fibroproliferative phase; may persist as post-infectious organizing pneumonia |
Other Systemic Effects
- Hyponatremia: SIADH (especially Legionella)
- Hepatic dysfunction: elevated transaminases from sepsis/hypoperfusion
- Renal impairment: AKI from sepsis, dehydration, nephrotoxic antibiotics
- Metabolic acidosis with multi-organ involvement
7. Clinical Presentation
Typical (Bacterial) Pneumonia
- Abrupt onset of fever (>38.5°C), rigors, productive cough with purulent/rust-colored sputum
- Pleuritic chest pain (parietal pleura involvement)
- Dyspnea proportional to extent of consolidation
- On auscultation: bronchial breath sounds, egophony (E→A change), increased tactile fremitus, dullness to percussion over consolidated area
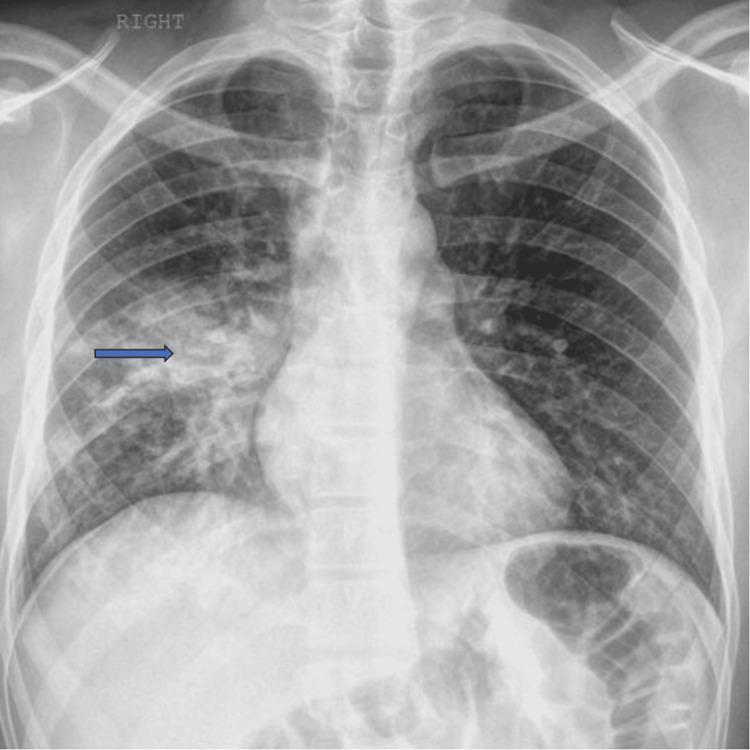
- Chest X-ray: lobar or segmental consolidation, air bronchograms
Atypical Pneumonia (Mycoplasma, Chlamydophila, Legionella)
- Gradual onset over days
- Dry, non-productive cough; prominent extrapulmonary features (headache, myalgia, diarrhea, rash)
- CXR: diffuse bilateral interstitial/patchy infiltrates, worse than physical exam suggests
- "Walking pneumonia" — patient ambulatory despite bilateral infiltrates
Viral Pneumonia
- Respiratory distress out of proportion to radiologic signs
- Interstitial pattern on CXR/CT; ground-glass opacities
- Inflammation confined to alveolar septa; no consolidative exudate initially
Chest X-ray Patterns

8. Diagnosis
Clinical Criteria
- ≥1 respiratory symptom (cough, dyspnea, pleuritic pain) + radiographic opacity + no alternative diagnosis
Laboratory Workup
| Test | Purpose |
|---|---|
| CBC | Leukocytosis (bacterial) or normal/low WBC (viral, Legionella) |
| CMP | Electrolytes (hyponatremia in Legionella), BUN/Cr (renal function) |
| Blood cultures x2 | Before antibiotics; positive in ~10–25% of hospitalized CAP |
| Sputum Gram stain + culture | Most useful if obtained before antibiotics; >25 PMN/LPF |
| Procalcitonin | Useful to guide antibiotic initiation/de-escalation |
| Urinary antigens | Pneumococcal and Legionella urinary antigens — rapid, high specificity |
| Nasopharyngeal PCR | Multiplex panels for viral/atypical pathogens |
| MRSA nasal swab | NPV >98% for MRSA pneumonia if negative — can guide de-escalation |
| ABG | PaO₂/FiO₂ ratio, degree of hypoxemia, need for ventilatory support |
Imaging
- CXR: First-line; lobar consolidation, air bronchograms, pleural effusion
- CT thorax: More sensitive; reveals cavitation, empyema, pulmonary emboli; useful when CXR equivocal or no improvement after 72h
Severity Scoring — Site-of-Care Decision
PSI (Pneumonia Severity Index) / PORT Score: Gold standard; classifies I–V; Class I–II → outpatient; III → observation; IV–V → hospital/ICU
CURB-65 (simpler bedside tool):
| Parameter | Score |
|---|---|
| Confusion | 1 |
| Urea >7 mmol/L | 1 |
| Respiratory rate ≥30/min | 1 |
| BP systolic <90 or diastolic ≤60 | 1 |
| Age ≥65 | 1 |
- Score 0–1: Outpatient
- Score 2: Short hospital admission
- Score 3–5: ICU consideration
IDSA/ATS Major Criteria for ICU Admission (either 1 major = ICU):
- Septic shock requiring vasopressors
- Invasive mechanical ventilation
9. Treatment
General Principles
- Empiric therapy based on disease severity, comorbidities, risk for drug-resistant organisms, and local antibiograms — per IDSA/ATS 2019 guidelines
- Time-to-antibiotics matters: each hour of delay in septic shock/hypotension increases mortality by 7–8%
- De-escalate based on cultures, procalcitonin trends, and MRSA nasal swab results
Outpatient Treatment (CURB-65 0–1, PSI Class I–II)
| Patient Type | Preferred Regimen |
|---|---|
| Healthy, no comorbidities, no recent antibiotics | Amoxicillin 1g TID × 5d OR Doxycycline 100mg BID × 5d |
| Comorbidities (DM, COPD, CHF, immunosupp.) | Combination: Amoxicillin-clavulanate + macrolide (azithromycin/clarithromycin) OR Respiratory fluoroquinolone monotherapy (levofloxacin 750mg QD or moxifloxacin 400mg QD) |
| Atypical suspected (younger, gradual onset) | Azithromycin 500mg Day 1 → 250mg Days 2–5 OR Doxycycline |
Inpatient — Non-ICU (CURB-65 2–3, PSI Class III–IV)
| First-Line | Alternative |
|---|---|
| β-lactam + macrolide (ampicillin-sulbactam or ceftriaxone + azithromycin) | Respiratory fluoroquinolone monotherapy (levofloxacin or moxifloxacin) |
- Observational studies show fluoroquinolone monotherapy achieves 30–45% relative mortality reduction vs. β-lactam alone for hospitalized CAP
- Duration: 5 days in clinically stable patients (afebrile ≥48h, tolerating PO, SpO₂ ≥90% on room air)
Inpatient — ICU / Severe CAP
| Regimen | Notes |
|---|---|
| β-lactam (ceftriaxone/ampicillin-sulbactam) + macrolide | Mainstay; macrolide addition shows 3% absolute mortality reduction (RR 0.82) in meta-analysis of 9850 ICU patients |
| β-lactam + respiratory fluoroquinolone | Alternative |
| Add MRSA coverage (vancomycin IV 15–20 mg/kg q8–12h or linezolid 600mg BID) | If: prior MRSA infection, hospitalization + IV antibiotics within 90 days, positive MRSA nasal swab |
| Add anti-pseudomonal β-lactam (pip-tazo, cefepime, meropenem) | If: risk factors for P. aeruginosa (structural lung disease, prior culture, prior antibiotics) |
Fishman's Pulmonary Diseases, p. 2264
Hospital-Acquired Pneumonia (HAP) / VAP
- Risk-stratify for MDR organisms (prior antibiotics within 90 days, hospitalization >5 days, prior MDR isolation, immunosuppression)
- Low MDR risk: piperacillin-tazobactam OR ceftriaxone OR levofloxacin
- High MDR risk: two anti-pseudomonal agents (e.g., pip-tazo + aminoglycoside OR fluoroquinolone) + vancomycin or linezolid for MRSA
- "PES pathogens" (Pseudomonas, ESBL-Enterobacterales, MRSA) account for up to 6% of hospitalized CAP but require broader spectrum coverage
Supportive Treatment (All Severities)
| Intervention | Notes |
|---|---|
| Supplemental oxygen | Target SpO₂ ≥94% (or ≥88–92% in COPD); high-flow nasal cannula (HFNC) in hypoxic CAP |
| IV fluid resuscitation | For sepsis-associated hypoperfusion; avoid over-resuscitation (worsens pulmonary edema) |
| Bronchodilators | If reactive airway component or COPD overlap |
| Chest physiotherapy | Aids secretion clearance |
| Antipyretics/analgesia | Acetaminophen/NSAIDs for fever and pleuritic pain |
| DVT prophylaxis | Heparin for all hospitalized patients |
| Early mobilization | Reduces VAP risk and promotes resolution |
| Corticosteroids | Dexamethasone (6mg/day × 3–5d) for severe CAP with ARDS or septic shock (select cases) |
| Mechanical ventilation | Low tidal volume strategy (6 mL/kg IBW) if ARDS develops; PEEP optimization |
| Pleural drainage | For empyema or large parapneumonic effusion |
Treatment Failure — When to Reassess (Goldman-Cecil, Table 85-7)
If no improvement at 48–72h, consider:
- Wrong antibiotic choice or inadequate dosing
- Drug-resistant organism (not covered by empiric regimen)
- Loculated empyema requiring drainage
- Endobronchial obstruction (cancer, foreign body)
- Non-infectious mimics: PE, malignancy, cryptogenic organizing pneumonia, heart failure
10. Duration of Therapy
| Setting | Antibiotic Duration |
|---|---|
| Outpatient CAP (healthy) | 5 days |
| Outpatient CAP (comorbidities) | 5–7 days |
| Hospitalized non-severe CAP | 5 days (if clinical stability criteria met) |
| Severe CAP (ICU) | 7–8 days |
| HAP/VAP (non-MDR) | 7 days |
| Legionella pneumonia | 7–14 days |
| S. aureus (MSSA) pneumonia | 14 days minimum |
| Lung abscess | 4–6 weeks |
Clinical stability criteria for stopping (when met): afebrile ≥48h, HR <100, RR <24, SpO₂ ≥90% on room air, tolerating oral intake, normal mentation. Procalcitonin trending down supports de-escalation.
11. Recovery Timeline
Outpatient (Mild CAP)
- Fever resolves: 2–4 days
- Cough improves: 5–14 days
- Fatigue may persist: 2–4 weeks
- Radiographic clearing: 4–8 weeks (longer in elderly, lobar pneumonia, bacteremic disease)
- Return to normal activity: 1–3 weeks
- Prognosis for full recovery is excellent for outpatients — Goldman-Cecil Medicine, p. 991
Hospitalized Patients
- ~85% of hospitalized patients respond within 7 days: improved cough and dyspnea, afebrile, tolerating oral intake → in-hospital mortality 1%, 30-day mortality 5%
- All-cause mortality:
- In-hospital: ~6%
- 30-day: ~13%
- 6-month: ~23%
- 1-year: ~30% (reflects comorbidities and underlying frailty)
- 70% discharged home (~one-third need home health follow-up); 30% discharged to nursing home or rehabilitation
- 30-day readmission rate: ~15% (higher in those requiring home health)
- Goldman-Cecil Medicine, p. 991
Predictors of Delayed Recovery / Poor Outcome
- Need for ICU at presentation
- Obesity, diabetes, active malignancy
- Age ≥65
- Bacteremia
- Causative organisms: MRSA, Legionella, Gram-negatives
- Delayed appropriate antibiotics
Mycoplasma Pneumonia Recovery
- Usually benign, self-limited with excellent prognosis
- Hospitalized adults: 8% mortality, particularly elderly
- ARDS/death rare
- Murray & Nadel's Respiratory Medicine
12. Prevention
| Strategy | Details |
|---|---|
| Pneumococcal vaccines | PCV20 (adults ≥65) or PCV15 + PPSV23 (1 year apart); 85% protection against serotype-specific CAP; conjugate vaccine given first |
| Influenza vaccine | Annual; significantly reduces viral CAP and secondary bacterial superinfection |
| RSV vaccine | Now available for adults ≥60 |
| Smoking cessation | Restores mucociliary function; major modifiable risk factor |
| Head-of-bed elevation (30–45°) | Reduces microaspiration risk, especially in ventilated/tube-fed patients |
| Oral hygiene | Chlorhexidine rinses in ICU — reduces VAP incidence |
| Hand hygiene | Reduces nosocomial transmission |
| Aspiration precautions | Swallowing assessment; avoid unnecessary nasogastric tubes |
Summary for Quick Reference
PNEUMONIA AT A GLANCE
─────────────────────────────────────────────────────────────
Definition: Acute lung parenchyma infection + imaging opacity
Top CAP bug: S. pneumoniae → lobar consolidation, bacteremia
Top HAP bug: S. aureus (MRSA), Pseudomonas, Gram-negatives
Pathophysiology: Intrapulmonary shunt → V/Q mismatch → hypoxemia
Key stages: Congestion → Red hepatization → Gray hepatization → Resolution
Severity tool: CURB-65 (0-1: outpatient; 2: admit; 3-5: ICU)
Mild CAP Rx: Amoxicillin 1g TID × 5d OR Doxycycline × 5d
ICU CAP Rx: β-lactam + macrolide ± MRSA/anti-Pseudomonal cover
Duration: 5 days (outpatient/non-severe) to 7-14 days (severe/special bugs)
85% respond: Within 7 days of hospitalization
30-day mortality: ~5% (outpatient) → ~13% (hospitalized)
Vaccine: PCV20 ≥65y, annual influenza
─────────────────────────────────────────────────────────────
Sources:
- Goldman-Cecil Medicine International Edition, Chapter 85: Overview of Pneumonia
- Robbins & Kumar Basic Pathology, Chapter: Community-Acquired Pneumonia
- Fishman's Pulmonary Diseases and Disorders, Chapters 122, 125, 129: CAP guidelines, antibiotic principles
- Murray & Nadel's Textbook of Respiratory Medicine: Gas exchange in pneumonia (MIGET studies)
- Rosen's Emergency Medicine: Pediatric pneumonia chapter
This is a shared conversation. Sign in to Orris to start your own chat.