can u explain about wpw syndrome from harrisons textbook in simpler terms defination, causes, associated with ,pathophysiology, ecg findings,investigation,and treatment and also types
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content from Harrison's to write a thorough, simplified explanation. Let me compose the full answer.
Wolff-Parkinson-White (WPW) Syndrome - Simplified from Harrison's Principles of Internal Medicine (22nd Edition, 2025)
1. Definition (What is WPW?)
WPW syndrome is defined as two things happening together:
- A pre-excited QRS on the ECG during normal heart rhythm (sinus rhythm)
- Episodes of paroxysmal supraventricular tachycardia (PSVT) - sudden rapid heartbeats
Think of it like this: your heart normally has ONE electrical pathway from the top chambers (atria) to the bottom chambers (ventricles) - the AV node. In WPW, there is an extra shortcut wire called an accessory pathway (AP). Because the shortcut bypasses the normal "speed controller" (the AV node), the ventricles can get electrical signals too fast, too early ("pre-excitation"), causing dangerous rapid heart rhythms.
- Harrison's, Chapter 256, p.1983
2. Causes / Origin
- Accessory pathways are present from birth (congenital) - they result from failure of complete separation of the atrium and ventricle by the fibrous AV ring during fetal development
- They occur in 1 in 1,500-2,000 people
- Most patients have structurally normal hearts
- The pathway can exist anywhere around the AV valve ring
3. Associated Conditions
WPW is associated with:
| Condition | Notes |
|---|---|
| Ebstein's anomaly | Most well-known cardiac association (abnormal tricuspid valve) |
| Hypertrophic cardiomyopathy | Especially PRKAG2 mutations |
| Danon's disease | A lysosomal storage disorder |
| Fabry's disease | A metabolic disorder |
| Mitral valve prolapse | Less common |
| Transposition of great vessels | Congenital |
| Endocardial fibroelastosis | |
| Tricuspid atresia | |
| Idiopathic (no cause found) | Most common scenario |
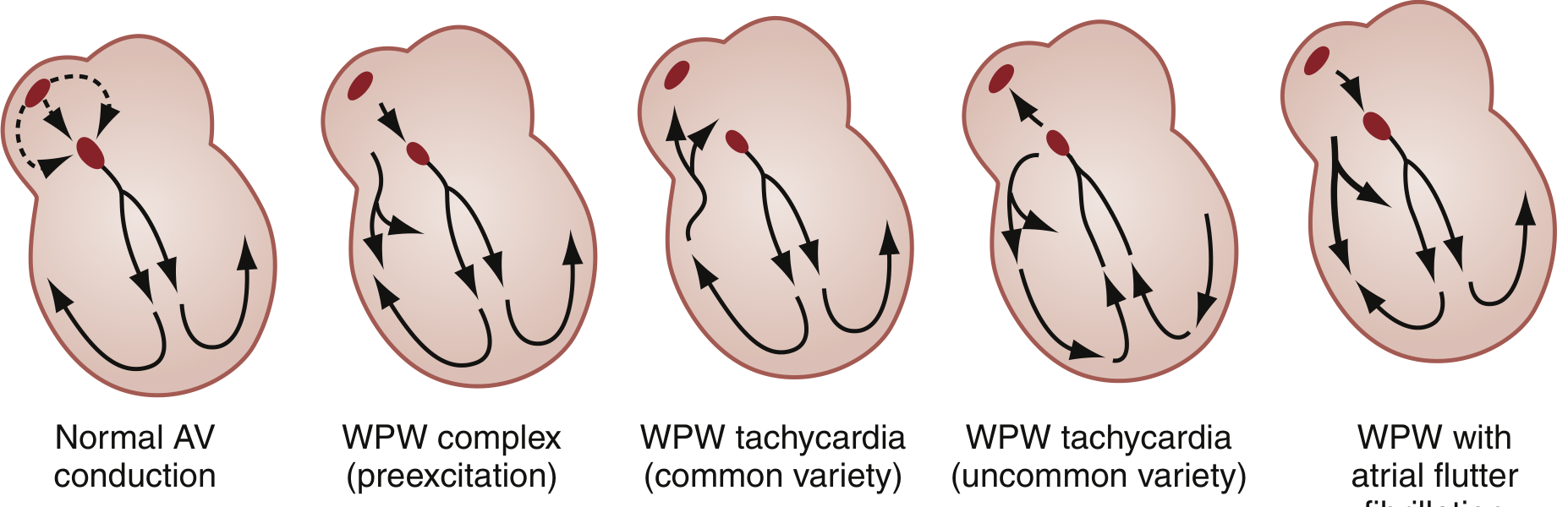
4. Pathophysiology (How Does it Cause Problems?)
Normal vs. WPW Conduction
In a normal heart, the electrical signal from the SA node travels to the AV node, which slows it down before allowing it to reach the ventricles. This delay is intentional - it lets the atria finish contracting before the ventricles contract.
In WPW, the accessory pathway bypasses the AV node. The signal reaches the ventricles EARLY (pre-excitation). This creates two problems:
1. Pre-excitation during normal rhythm:
- Part of the ventricle gets activated early via the AP
- The rest gets activated normally via the AV node
- This "fusion" of two activation wavefronts produces the characteristic ECG changes
2. Re-entry circuits causing tachycardia:
Because there are now TWO pathways between atria and ventricles, an electrical signal can go around in a loop - down one pathway, back up the other, and repeat. This loop is called a re-entry circuit and it's what causes the rapid heart rate (tachycardia).
5. Types of WPW / Accessory Pathways
By Conduction Direction:
| Type | Direction of Conduction | Preexcitation on ECG? | Can Cause Tachycardia? |
|---|---|---|---|
| Manifest AP | Both antegrade (A→V) and retrograde (V→A) | YES | YES |
| Concealed AP | Only retrograde (V→A) | NO | YES (orthodromic AVRT) |
| Fasciculoventricular connections | His bundle → ventricular septum | YES | NO (circuit too short for reentry) |
| Atriofascicular (Mahaim fibers) | Right atrium → right bundle branch | YES | Wide-complex tachycardia with LBBB pattern |
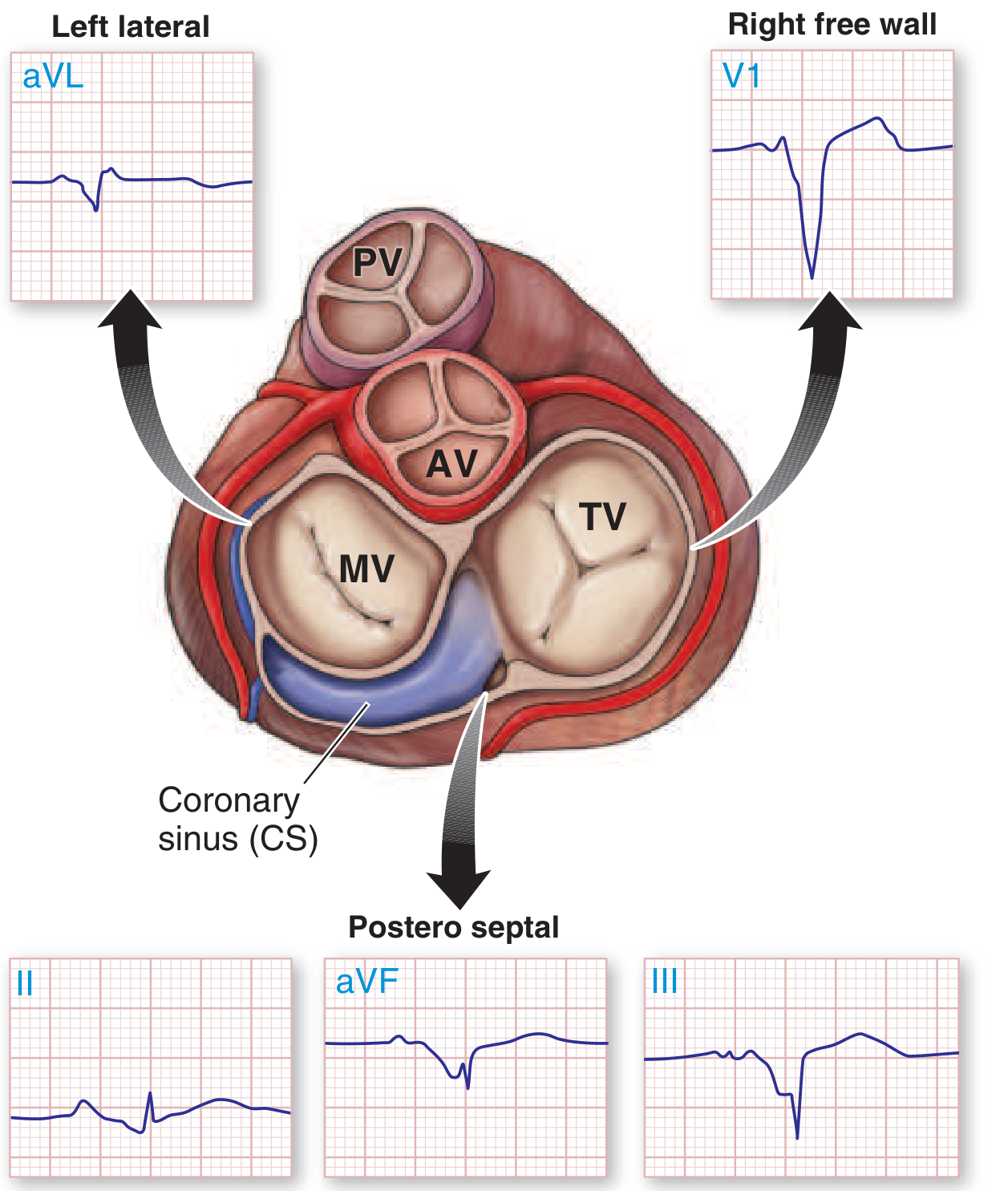
By Location (Pathway Position Around the AV Ring):
- Left free wall - Most common location; may show minimal preexcitation
- Posteroseptal - Second most common; produces negative delta waves in leads III and aVF (can mimic inferior MI)
- Right free wall - Produces LBBB-like pattern in V1
- Anteroseptal - Near AV node; highest risk of AV block if ablated
By Tachycardia Type:
1. Orthodromic AVRT (most common - ~95%)
- Signal goes: Atrium → AV node → Ventricle → AP (backward) → Atrium
- Narrow QRS tachycardia (normal-looking QRS because ventricles activated normally)
- P wave comes AFTER the QRS (in the ST segment)
2. Antidromic AVRT (less common - ~5%)
- Signal goes: Atrium → AP (forward) → Ventricle → AV node (backward) → Atrium
- Wide QRS tachycardia (looks like ventricular tachycardia - dangerous to confuse!)
- The QRS is "maximally preexcited"
3. Preexcited AF/flutter (most dangerous)
- During atrial fibrillation, all the very fast atrial signals (300-600/min) can shoot straight down the AP without being filtered by the AV node
- Can produce ventricular rates >250-300/min
- Can degenerate to ventricular fibrillation → SUDDEN DEATH
6. ECG Findings
Classic WPW Pattern (Sinus Rhythm):
| Finding | What it means | Value |
|---|---|---|
| Short PR interval | Signal bypasses AV node delay | < 0.12 seconds |
| Delta wave | Slurred upstroke at start of QRS | Caused by slow direct activation of ventricular muscle via AP |
| Wide QRS complex | Prolonged ventricular activation | > 0.12 seconds |
| Secondary ST-T changes | Opposite to delta wave direction | Not due to ischemia |
Simple way to remember the classic triad:
Short PR + Delta wave + Wide QRS = WPW
ECG Patterns by Location:
- Right-sided AP: LBBB-like pattern in V1 (the right ventricle is pre-excited)
- Left-sided AP: RBBB-like pattern in V1; negative delta in aVL (mimics lateral wall MI)
- Posteroseptal AP: Negative delta waves in leads III and aVF (mimics inferior MI)
During Tachycardia:
- Orthodromic AVRT: Narrow QRS, P wave in ST segment after QRS
- Antidromic AVRT: Wide bizarre QRS, indistinguishable from VT
- Preexcited AF: Irregularly irregular wide QRS, rate >250, QRS morphology changes beat-to-beat
7. Investigations
| Investigation | Purpose |
|---|---|
| 12-lead ECG | Diagnosis: shows short PR, delta wave, wide QRS |
| 24-hour Holter / ambulatory ECG | Detects intermittent preexcitation and arrhythmia episodes |
| Exercise stress test | Assesses risk: abrupt loss of preexcitation at physiologic heart rates = low-risk pathway |
| Echocardiogram | Rules out associated structural heart disease (Ebstein's, HCM, tachycardia-mediated cardiomyopathy) |
| Electrophysiology (EP) study | THE KEY INVESTIGATION - maps the AP location, determines if rapid conduction is possible, measures the shortest R-R interval during induced AF. Risk assessment for sudden death. Usually combined with ablation. |
Important note from Harrison's: Gradual loss of preexcitation on exercise does NOT reliably indicate low risk because AV nodal conduction shortening can account for this, not loss of AP function.
8. Treatment
Acute (Emergency) Management
If hemodynamically unstable (hypotension, collapse):
- Immediate electrical cardioversion (synchronized DC cardioversion) - regardless of the rhythm
If hemodynamically stable - depends on the rhythm:
| Situation | Treatment | What to AVOID |
|---|---|---|
| Orthodromic AVRT (narrow complex) | Vagal maneuvers first → IV adenosine → IV beta blocker or verapamil/diltiazem | - |
| Wide complex tachycardia (uncertain) | Treat as VT; IV adenosine trial if rhythm regular and stable | AV-nodal blockers if VT suspected |
| Preexcited AF (wide irregular, rate >250) | Electrical cardioversion OR IV procainamide or ibutilide | ABSOLUTELY AVOID: adenosine, digoxin, verapamil, diltiazem, beta blockers, IV amiodarone |
Why avoid AV-nodal blockers in preexcited AF?
These drugs block the AV node but leave the AP unblocked. This forces ALL the atrial signals through the AP, which can ACCELERATE the ventricular rate and trigger ventricular fibrillation.
Long-Term / Definitive Management
Catheter Ablation (Gold Standard):
- Efficacy: ~95% for most AP locations
- Procedure mortality: <1 in 1,000
- Major complications: <3% (AV block, cardiac tamponade, thromboembolism, coronary artery injury)
- Risk of AV block is higher for anteroseptal and mid-septal locations (near the AV node/His bundle)
- After successful ablation, AF typically does NOT recur (since AVRT that triggered AF is eliminated)
Indications for EP study + ablation:
- Symptomatic arrhythmias (palpitations, syncope, pre-syncope)
- High-risk occupations (pilots, police, military)
- Anyone who wants definitive evaluation of their risk
Drug therapy (for those who don't want or can't have ablation):
- Beta blockers, verapamil, diltiazem - for orthodromic AVRT / low-risk pathways
- Flecainide - reduces recurrence
- These are only used when AP is confirmed low-risk (no rapid antegrade conduction)
For asymptomatic adults with preexcitation:
- Sudden death risk: ~1 per 1,000 patient-years
- Routine observation without therapy is reasonable in low-risk individuals
- EP study advised if in a high-risk occupation
For children:
- Higher risk of sudden death (~2 per 1,000 patient-years)
- More proactive evaluation generally recommended
Quick Summary Table
| Feature | WPW Syndrome |
|---|---|
| Definition | Pre-excited QRS + episodes of PSVT |
| Mechanism | Accessory pathway bypasses AV node |
| Incidence | 1 in 1,500-2,000 people |
| ECG classic triad | Short PR (<0.12s) + Delta wave + Wide QRS |
| Most dangerous arrhythmia | Preexcited AF → risk of VF and sudden death |
| Drug to AVOID | Digoxin, verapamil, diltiazem, beta blockers, adenosine during preexcited AF |
| Definitive treatment | Catheter ablation (~95% success) |
| Key investigation | EP study (maps pathway + risk assessment) |
Based on Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 256 - Supraventricular Arrhythmias, and supported by Rosen's Emergency Medicine and Braunwald's Heart Disease.
This is a shared conversation. Sign in to Orris to start your own chat.