describe with all images and flowcharts about moisturizers related to unani and modern perspectives acoording to old and recent advancements
moisturizer skin barrier emollient humectant
moisturizer emollient skin barrier
skin moisturizer mechanism stratum corneum barrier diagram
Unani herbal plant oils skin treatment traditional medicine
Unani medicine moisturizers murattibal skin care traditional concepts emollients
Unani medicine skin aging moisturizer herbal
emollient humectant occlusive moisturizer classification types comparison
Unani skin aging innate moisture herbal formulation
PMID: 39715571
PMID: 40176773
PMID: 40231699
Moisturizers: Unani & Modern Perspectives — Old Traditions to Recent Advances
PART 1 — UNANI PERSPECTIVE
1.1 Foundational Concepts
| Unani Concept | Description |
|---|---|
| Hararat Ghariziyya (Innate Heat) | Vital thermal energy inherent in all living tissues |
| Rutubat Ghariziyya (Innate Moisture) | Natural body moisture sustaining tissue suppleness and vitality |
1.2 Unani Theory of Skin Mizaj (Temperament)
┌─────────────────────────────────────────────────────────────┐
│ UNANI TEMPERAMENT (MIZAJ) OF SKIN │
│ │
│ Hot + Moist (Dam / Sanguine) → Well-hydrated, radiant │
│ Hot + Dry (Safra / Bilious) → Oily, prone to acne │
│ Cold + Moist (Balgham / Phlegmatic) → Pale, puffy skin │
│ Cold + Dry (Sawda / Melancholic) → Dry, wrinkled skin │
│ ↓ │
│ Moisture-restoring therapies target: │
│ Cold + Dry Mizaj (Yabus + Bard) │
│ → Murattibal (Moistening) agents used │
└─────────────────────────────────────────────────────────────┘
1.3 Historical Unani Texts on Skin Cosmetics
| Scholar | Era | Contribution |
|---|---|---|
| Hippocrates | ~460–370 BCE | Foundation of temperament theory; basis of skin health |
| Dioscorides | 40–90 CE | Materia Medica — plant oils for skin |
| Galen | 129–216 CE | Stabilized theory of humors; introduced cold cream (Ceratum Galeni) |
| Razi (Zakariya al-Razi) | 854–925 CE | Chapter "Zeenat wa Araish" (Beautification) in Kitab al-Mansuri |
| Al-Zohrawi (Albucasis) | 936–1013 CE | Kitab al-Tasrif (30 volumes) — cosmetics as Adwiyat al-Zinat (beautifying drugs) |
| Ibn Sina (Avicenna) | 980–1037 CE | Al-Qanun fi'l-Tibb — detailed skin moisture management |
1.4 Unani Classification of Skin Moisturizing Agents
Murattibal (Moisteners — agents that add moisture)
UNANI MOISTURIZING DRUGS (MURATTIBAL)
│
├── PLANT-BASED (Nabati)
│ ├── Roghan Badam (Almond oil) — Softens, nourishes, repairs dry skin
│ ├── Roghan Zaitoon (Olive oil) — Rich emollient; used since antiquity
│ ├── Roghan Kunjad (Sesame oil) — Warming, penetrating emollient
│ ├── Roghan Narjeel (Coconut oil) — Occlusive; prevents TEWL
│ ├── Roghan Arandi (Castor oil) — Thick humectant/occlusive
│ ├── Aloe vera (Sibr) — Humectant, anti-inflammatory
│ ├── Honey (Asal) — Humectant, antimicrobial
│ └── Beeswax (Mom) — Occlusive, emulsifier in Unguents
│
├── ANIMAL-BASED (Hayawani)
│ ├── Mum (Beeswax) — Occlusive barrier former
│ ├── Fat of various animals — Historical occlusives
│ └── Milk (Sheer) / Butter (Makhkhan) — Soothing, emollient
│
└── MINERAL-BASED (Madani)
├── Multani mitti (Fuller's earth) — Absorbent cleanser
└── Kaolin/Clay minerals — Skin-softening
Mulayyinaat (Emollients — agents that soften skin texture)
- Smooth and soften the stratum corneum
- Correct Khushunat (roughness)
- Examples: Roghan-e-Badam Shirin (sweet almond oil), Roghan-e-Zaitoon
Murakhkhiyat (Relaxants — agents that relax contracted/tense skin)
- Relieve tightness and rigidity
- Used in conditions like Tashannuj (spasm) or chronically dry skin
1.5 Unani Cosmeceutical Formulations for Skin Moisture
| Formulation Type | Unani Name | Ingredients | Modern Equivalent |
|---|---|---|---|
| Ointment | Marham | Wax + oil base + botanicals | Ointment/unguent |
| Paste | Zimaad | Powder + oil/fat | Thick paste |
| Cream | Naqoo' | Water + oil emulsion | Cream |
| Oil | Roghan | Fixed vegetable/animal oils | Oil formulation |
| Poultice | Tila | Applied topically for skin care | Topical application |
- Beeswax + Rose water + Almond/Olive oil
- Galen (129–216 CE) described this as a water-in-oil emulsion — the earliest known moisturizing cream in history
1.6 Unani Management Protocol for Dry Skin (Yuboosat-e-Jild)
ASSESSMENT
│
▼
Identify Mizaj (Temperament) → Cold + Dry (Sawda)?
│
▼
RESTORE INNATE MOISTURE (Rutubat Ghariziyya)
│
├─── Tadbeer (Regimenal Therapy)
│ ├── Hammam (Steam bath) — hydrates and opens pores
│ ├── Taleeq (Massage with oils)
│ └── Appropriate diet (moist, warm foods)
│
└─── Ilaj-bil-Dawa (Drug Therapy)
├── Internal: Murattibal drugs (almond oil, honey)
└── External (Tila/Marham): Roghan Badam + Roghan Zaitoon
+ Mum (beeswax) + Rose water
PART 2 — MODERN SCIENTIFIC PERSPECTIVE
2.1 Skin Anatomy Relevant to Moisturization
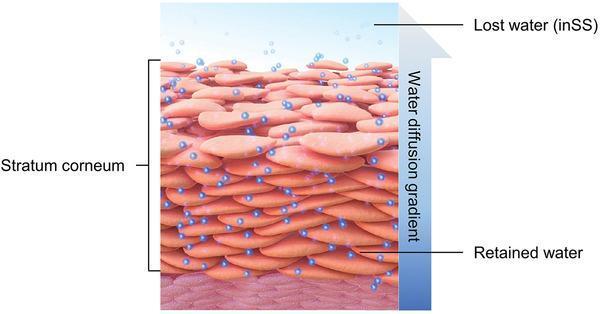
- Corneocytes — "bricks" (protein-rich, flattened dead cells)
- Intercellular lipid bilayers — "mortar" (ceramides + cholesterol + free fatty acids in 1:1:1 molar ratio)
- Natural Moisturizing Factor (NMF) — hygroscopic compounds derived from filaggrin breakdown (amino acids, pyrrolidone carboxylic acid, urocanic acid, lactate)
- Aquaporins — water channel proteins (AQP3 in keratinocytes)
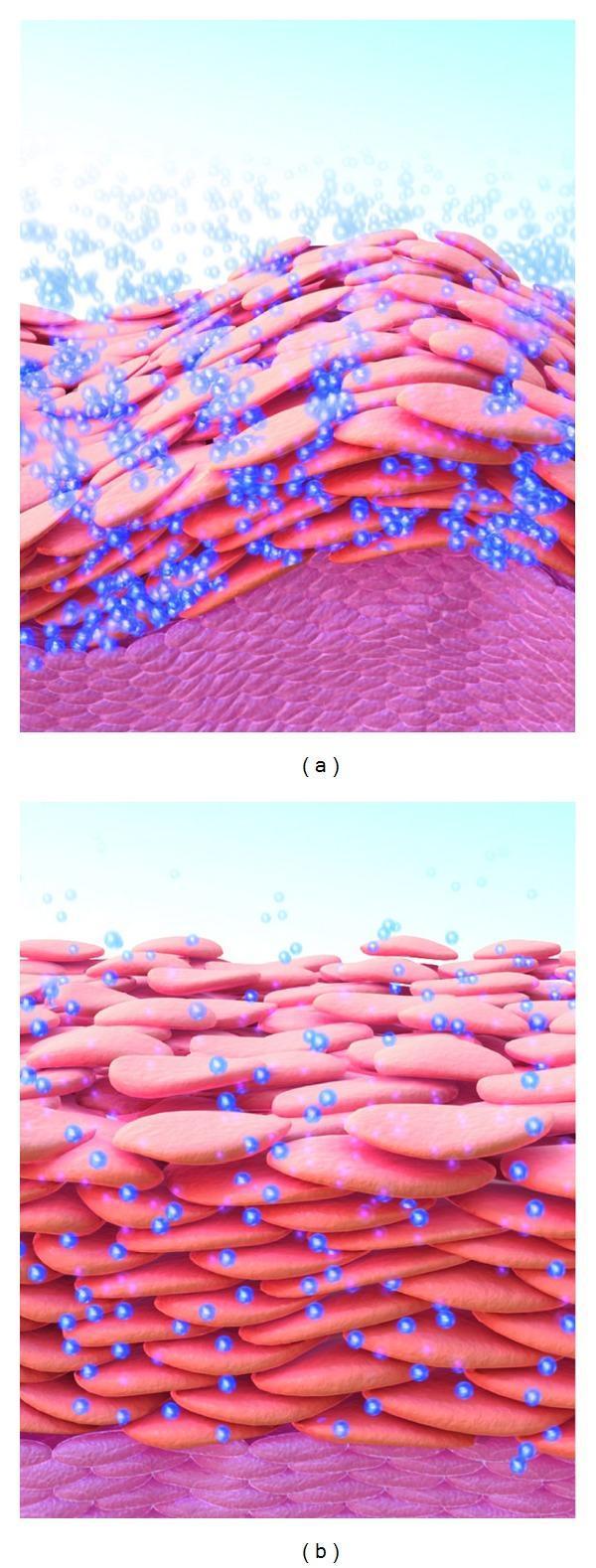
2.2 Transepidermal Water Loss (TEWL)
2.3 Modern Classification of Moisturizers
The Three Functional Classes
┌────────────────────────────────────────────────────────────────┐
│ MODERN MOISTURIZER CLASSIFICATION │
│ │
│ ┌─────────────┐ ┌────────────────┐ ┌──────────────────┐ │
│ │ OCCLUSIVES │ │ HUMECTANTS │ │ EMOLLIENTS │ │
│ │ │ │ │ │ │ │
│ │ Form oily │ │ Attract water │ │ Fill gaps between│ │
│ │ film on SC │ │ from dermis to │ │ corneocytes; │ │
│ │ → ↓ TEWL │ │ SC (& from air │ │ smooth texture │ │
│ │ │ │ if RH >70%) │ │ │ │
│ │ Petrolatum │ │ Glycerin │ │ Fatty acids │ │
│ │ (99% ↓TEWL)│ │ Hyaluronic acid│ │ Fatty alcohols │ │
│ │ Mineral oil │ │ Urea │ │ Lanolin │ │
│ │ Dimethicone │ │ Sodium lactate │ │ Plant oils │ │
│ │ Beeswax │ │ Propylene glycol│ │ Ceramides │ │
│ │ Lanolin │ │ Sorbitol │ │ Squalene │ │
│ │ Castor oil │ │ Honey │ │ Silicones │ │
│ │ Vegetable │ │ NaPCA │ │ Cholesterol │ │
│ │ waxes │ │ Aloe vera │ │ │ │
│ └─────────────┘ └────────────────┘ └──────────────────┘ │
│ │
│ MOST EFFECTIVE COMBINATION = Occlusive + Humectant + │
│ Emollient working together in one formulation │
└────────────────────────────────────────────────────────────────┘
2.4 Mechanism of Action — Step-by-Step Flowchart
DAMAGED / DRY STRATUM CORNEUM
(↓ NMF, ↓ ceramides, ↑ TEWL, tight/rough/flaky skin)
│
▼
APPLY MOISTURIZER
│
┌────┴─────────────────────────┐
│ │
▼ ▼
OCCLUSIVE LAYER HUMECTANT
(e.g. petrolatum) (e.g. glycerin)
│ │
▼ ▼
Fills interstices of SC Attracts water from
Reduces TEWL by up to 99% deeper dermal layers
│ │
└──────────┬───────────────────┘
▼
INCREASED SC WATER CONTENT
(target 10–30% optimal)
│
┌──────────┴──────────────────────┐
│ │
▼ ▼
EMOLLIENT ACTION BARRIER REPAIR SIGNAL
(ceramides, fatty acids) (some TEWL preserved
→ stimulates lipid synthesis)
│ │
▼ ▼
Fills gaps between SC synthesizes new
desquamating corneocytes intercellular lipids
→ Smooth texture → Long-term barrier repair
│
▼
RESTORED SKIN BARRIER
+ IMPROVED HYDRATION
+ SOFT TEXTURE
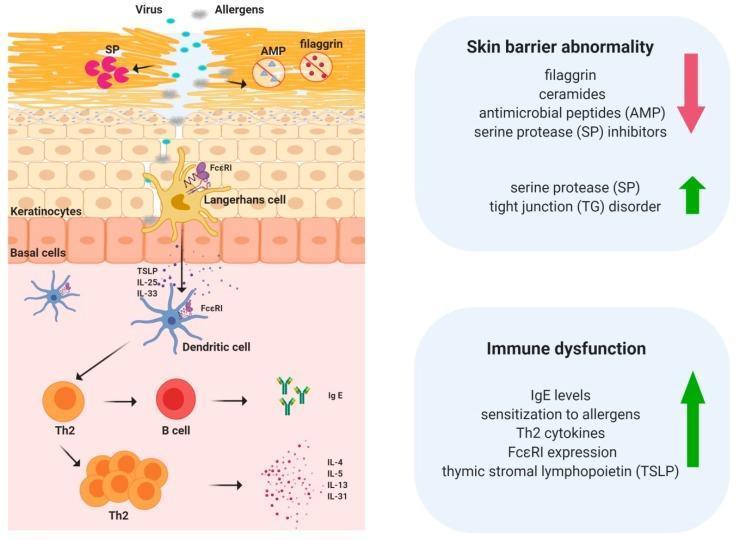
2.5 Skin Barrier & the Atopic Dermatitis Paradigm
2.6 Modern Moisturizer Types — Formulation Table
| Type | Composition | Best For | Examples |
|---|---|---|---|
| Oil only | Petrolatum | Severely dry/eczematous skin | Vaseline |
| Oil-in-water emulsion | Water + petrolatum | General dry skin | Eucerin, Vanicream |
| Polymer-based | Water + polyglyceryl-methacrylate + petrolatum | Sensitive skin | Cetaphil cream |
| Vegetable oil & wax | Castor oil, corn oil, beeswax, paraffin | Lips, very dry patches | Neutrogena formula |
| Glycerin-rich | Water + glycerin + petrolatum | Normal to dry skin | Neutrogena hand cream |
| Ceramide-based | Petrolatum + dimethicone + ceramides | Atopic dermatitis, eczema | CeraVe, EpiCream |
2.7 The Three-Product Skin Care System
SKIN CARE REGIMEN FLOWCHART
│
▼
1. CLEANSER
(Remove sebum, bacteria, dead cells)
├── True soap (pH 9–10) → best for oily/dirty skin
├── Syndet (pH 5.5–7) → best for sensitive/dry skin
└── Combar (pH 9–10) → best for normal skin
│
▼
2. ASTRINGENT / TONER (optional)
(Remove residue; deliver actives)
├── Oily skin: salicylic acid, witch hazel
└── Dry skin: propylene glycol, allantoin
│
▼
3. MOISTURIZER
(Repair & maintain epidermal barrier)
├── Dry skin → thicker, higher lipid content (cream/ointment)
├── Normal skin → lotion or light cream
└── Oily skin → gel-based, non-comedogenic
│
▼
OPTIONAL: SUNSCREEN (SPF ≥30, UVA+UVB)
├── Zinc oxide (inorganic, well-tolerated)
└── Titanium dioxide
PART 3 — PARALLEL COMPARISON: UNANI vs. MODERN
┌──────────────────────────────────┬──────────────────────────────────┐
│ UNANI CONCEPT │ MODERN EQUIVALENT │
├──────────────────────────────────┼──────────────────────────────────┤
│ Rutubat Ghariziyya (innate │ Natural Moisturizing Factor │
│ moisture) │ (NMF) in stratum corneum │
├──────────────────────────────────┼──────────────────────────────────┤
│ Murattibal (moistening agents) │ Humectants + Emollients │
├──────────────────────────────────┼──────────────────────────────────┤
│ Murakhkhiyat (relaxants) │ Emollients (texture improvement) │
├──────────────────────────────────┼──────────────────────────────────┤
│ Marham (ointment base) │ Oil-based / petrolatum ointment │
├──────────────────────────────────┼──────────────────────────────────┤
│ Mum (beeswax) │ Occlusive agent │
├──────────────────────────────────┼──────────────────────────────────┤
│ Roghan Zaitoon (olive oil) │ Squalene, fatty acids, occlusives│
├──────────────────────────────────┼──────────────────────────────────┤
│ Asal (honey) │ Humectant (hygroscopic agent) │
├──────────────────────────────────┼──────────────────────────────────┤
│ Sibr (Aloe vera) │ Humectant + anti-inflammatory │
├──────────────────────────────────┼──────────────────────────────────┤
│ Roghan Badam (almond oil) │ Emollient (oleic acid rich) │
├──────────────────────────────────┼──────────────────────────────────┤
│ Galenic cold cream │ Modern w/o emulsion moisturizer │
│ (beeswax + rose water + almond │ │
│ oil) │ │
├──────────────────────────────────┼──────────────────────────────────┤
│ Hammam (steam bath) │ Wet-wrap / soak-and-smear method │
├──────────────────────────────────┼──────────────────────────────────┤
│ Mizaj-e-Sawda (melancholic = │ Xerosis / dry skin / eczema │
│ Cold+Dry temperament) │ (SC barrier dysfunction) │
└──────────────────────────────────┴──────────────────────────────────┘
PART 4 — KEY UNANI HERBS WITH MODERN SCIENTIFIC VALIDATION
| Unani Drug | Active Constituents | Unani Action | Modern Mechanism |
|---|---|---|---|
| Roghan Badam (Almond oil) | Oleic acid (70%), linoleic acid, Vit E | Murattibal, Mulayyinaat | Emollient; restores SC lipids; antioxidant |
| Roghan Zaitoon (Olive oil) | Squalene, oleic acid, polyphenols | Murattibal, anti-aging | Emollient + antioxidant; SC lipid replenisher |
| Asal (Honey) | Fructose, glucose, organic acids | Murattibal | Humectant; osmotic antibacterial; wound healer |
| Roghan Narjeel (Coconut oil) | Lauric acid (50%), MCTs | Murattibal, Mulayyinaat | Occlusive + antimicrobial (lauric acid) |
| Sibr (Aloe vera) | Polysaccharides, acemannan | Murattibal, Mubarrid | Humectant; anti-inflammatory; promotes wound healing |
| Gule Surkh (Rose) | Flavonoids, terpenes, vitamin C | Mubarrid (cooling) | Antioxidant; skin barrier support |
| Sandal (Sandalwood) | α/β-Santalol | Mubarrid, anti-itch | Anti-inflammatory; soothes reactive skin |
| Roghan Kunjad (Sesame oil) | Linoleic acid, sesamin | Murattibal | Emollient; UV-absorbing; antifungal |
| Roghan Arandi (Castor oil) | Ricinoleic acid (90%) | Murattibal, Mulayyin | Thick humectant + occlusive; promotes barrier recovery |
| Mum (Beeswax) | Esters, hydrocarbons | Marham base | Occlusive; emulsifier; antimicrobial |
PART 5 — RECENT ADVANCES (2023–2026)
5.1 Molecular Targets of Modern Moisturizers
- ↑ Claudin-4 (CLD4) — tight junction protein; enhances barrier
- ↑ Aquaporin-3 (AQP3) — water transport into keratinocytes
- ↑ Hyaluronic Acid Synthase-2 (HAS2) — endogenous HA production
- ↓ Hyaluronidase-1 (HYAL1) — reduces HA degradation
- Clinical result: 116% improvement in skin hydration at 8 weeks
MODERN MOISTURIZER: MOLECULAR MECHANISM
│
Applied to SC
│
┌────┴────────────────────────┐
│ │
▼ ▼
Barrier proteins upregulated Water channel support
(Claudin-4, Filaggrin) (AQP3 ↑)
│ │
▼ ▼
↑ Tight junction integrity ↑ Transepidermal water delivery
│ │
└──────────┬──────────────────┘
▼
Hyaluronic acid synthesis ↑ (HAS2)
Hyaluronidase inhibited (HYAL1 ↓)
│
▼
SUSTAINED ENDOGENOUS HYDRATION
+ STRUCTURAL BARRIER RESTORATION
5.2 Current Standard of Care for Xerosis (2025)
- Skin hydration primarily mediated by SC's NMF and intercellular lipid bilayer
- Xerosis triggers: Cold weather, aging, pollution, medications, atopic dermatitis, psoriasis, diabetes, hypothyroidism
- Standard of care: Basic emollients with humectants (glycerol, urea, lactic acid) + occludents (petrolatum, liquid paraffin)
- Basic emollients remain first-line, long-term management for xerosis and associated inflammatory skin diseases
5.3 Ceramide-Centric Formulations
- Ceramide 1, 4, 7 — the three key SC ceramide species critical for lamellar bilayer organization
- Ceramides + cholesterol + free fatty acids must maintain 1:1:1 molar ratio for optimal barrier function
- Deficiency in any → altered bilayer → ↑ TEWL → dry skin / eczema — Dermatology 2-Volume Set 5e, p. 2636
5.4 Microbiome-Aware Moisturizers
- Support Staphylococcus epidermidis (commensal) over S. aureus (pathogen)
- Maintain optimal skin pH (5.4) which favors barrier enzyme function
SUMMARY MASTER FLOWCHART
┌──────────────────────────────────────────────────────────────────┐
│ MOISTURIZERS: FROM UNANI TO MODERN SCIENCE │
│ │
│ UNANI THEORY MODERN SCIENCE │
│ ───────────── ──────────────── │
│ Rutubat Ghariziyya ──► Natural Moisturizing Factor (NMF) │
│ Hararat Ghariziyya ──► Metabolic activity of keratinocytes │
│ Murattibal agents ──► Humectants (glycerin, HA, honey) │
│ Marham (ointment) ──► Occlusives (petrolatum, beeswax) │
│ Mulayyinaat agents ──► Emollients (ceramides, fatty acids) │
│ Hammam (steam bath) ──► Wet-wraps / hydration therapy │
│ │
│ TRADITIONAL PLANTS → MODERN VALIDATION │
│ Roghan Zaitoon → Squalene/oleic acid (emollient) │
│ Asal (honey) → Humectant + antimicrobial │
│ Sibr (aloe) → Polysaccharide humectant + anti-inflammatory │
│ Mum (beeswax) → Occlusive barrier former │
│ │
│ RECENT ADVANCES (2023–2026) │
│ ► Ceramide-centric formulations (CeraVe) │
│ ► AQP3 / Claudin-4 / HAS2 molecular targeting │
│ ► Microbiome-aware prebiotics in moisturizers │
│ ► Filaggrin-stimulating formulations (AD management) │
│ ► Bioactive NMF supplements (PCA, urocanic acid, amino acids) │
└──────────────────────────────────────────────────────────────────┘
Sources
- Dermatology 2-Volume Set 5e — pp. 3096–3098, 3708–3733 (Moisturizers & Skin Care Products)
- Fitzpatrick's Dermatology Vol. 1 & 2 — pp. 406, 2636 (Emollients, SC formation, atopic dermatitis)
- Pfenninger and Fowler's Procedures for Primary Care — Choosing a Skin Care Regimen
- Prevention and Management of Skin Aging in Unani System of Medicine — Bibi Chand & Husain Safder, Alt Ther Health Med, 2025 [PMID 39715571]
- Emollient-Rich Moisturizer: Three Elements of Natural Moisturization — Draelos ZD & Nelson DB, J Cosmet Dermatol, 2025 [PMID 40176773]
- Restoring Skin Hydration — Mechanistic Insights Into Basic Emollients — Fluhr JW et al., Int J Dermatol, 2025 [PMID 40231699]
- Microbiota and Skin Barrier in Aging Skin — Woo YR & Kim HS, Front Physiol, 2024 [PMID 38312314]
journal articles different types
Types of Journal Articles — Complete Guide
Overview Flowchart
JOURNAL ARTICLES
│
├── PRIMARY RESEARCH (Original data collected)
│ ├── Experimental
│ │ ├── Randomized Controlled Trial (RCT)
│ │ ├── Non-Randomized / Quasi-Experimental
│ │ └── Laboratory / In Vitro Study
│ └── Observational
│ ├── Cohort Study
│ ├── Case-Control Study
│ └── Cross-Sectional Study
│
├── SECONDARY RESEARCH (Synthesizes existing data)
│ ├── Systematic Review
│ ├── Meta-Analysis
│ └── Narrative Review
│
├── SPECIAL REPORT TYPES
│ ├── Case Report
│ ├── Case Series
│ ├── Technical Report / Short Communication
│ └── Conference Abstract
│
└── OPINION / EXPERT COMMENTARY
├── Editorial
├── Letter to the Editor
├── Commentary
└── Expert Opinion / Perspective
1. Randomized Controlled Trial (RCT)
Population
│
▼
RANDOMIZATION (random allocation)
│
├──── Intervention Group (receives treatment)
│ │
│ ▼
│ Outcome measured
│
└──── Control Group (placebo / standard care)
│
▼
Outcome measured
│
▼
COMPARISON of outcomes
| Feature | Detail |
|---|---|
| Hierarchy | Highest level for evaluating treatment efficacy |
| Blinding | Single-blind / double-blind / triple-blind |
| Allocation concealment | Prevents selection bias |
| CONSORT checklist | Reporting standard |
| Limitation | Expensive; ethical constraints; may lack real-world generalizability |
| Example | "Does ceramide moisturizer reduce TEWL vs. petrolatum in atopic dermatitis?" |
2. Systematic Review
CLINICAL QUESTION (PICO)
│
▼
Comprehensive database search
(PubMed, Cochrane, Embase, CINAHL...)
│
▼
Screening by title/abstract
│
▼
Full-text review
│
▼
Quality appraisal (Cochrane RoB, GRADE)
│
▼
Data extraction
│
▼
SYNTHESIS (Narrative or Quantitative)
│
▼
CONCLUSIONS + GRADE of evidence
| Feature | Detail |
|---|---|
| Hierarchy | Gold standard for evidence synthesis |
| PRISMA | Reporting standard (Preferred Reporting Items for Systematic Reviews) |
| Includes | Protocol, search strategy, inclusion/exclusion criteria, risk-of-bias assessment |
| Limitation | Only as good as included studies; publication bias possible |
3. Meta-Analysis
Study 1 (n=50) ────┐
Study 2 (n=80) ────┤
Study 3 (n=120) ────┤──► POOLED STATISTICAL ANALYSIS
Study 4 (n=60) ────┤ │
Study 5 (n=200) ────┘ ▼
FOREST PLOT
(Effect sizes + 95% CI)
│
▼
Combined effect estimate
Heterogeneity (I² statistic)
Funnel plot for publication bias
| Feature | Detail |
|---|---|
| Output | Forest plot; pooled OR/RR/MD; heterogeneity (I²) |
| Often combined with | Systematic review |
| Hierarchy | Highest level of quantitative evidence |
| Limitation | "Garbage in, garbage out" — poor input studies = poor pooled result |
4. Cohort Study
TIME LINE →→→→→→→→→→→→→→→→→→→→→→→→→→→→→→→
EXPOSED group ──────────────────► Outcome? (Disease / event)
│ (e.g., uses moisturizer)
│
├──── Outcome YES → Calculate incidence
└──── Outcome NO
NON-EXPOSED group ───────────────► Outcome? (Disease / event)
│
├──── Outcome YES → Calculate incidence
└──── Outcome NO
COMPARISON → Relative Risk (RR)
| Feature | Detail |
|---|---|
| Direction | Exposure → Outcome (forward in time) |
| Best for | Incidence, risk factors, natural history |
| Measure | Relative Risk (RR) |
| Limitation | Long follow-up; loss to follow-up; expensive |
| Example | "Do daily moisturizer users have lower incidence of eczema flares over 2 years?" |
5. Case-Control Study
TIME LINE ←←←←←←←←←←←←←←←←←←←←←
PRESENT ──────────────► PAST (look back)
CASES (WITH disease/outcome)
│
└──► Were they EXPOSED? YES / NO
CONTROLS (WITHOUT disease/outcome)
│
└──► Were they EXPOSED? YES / NO
COMPARISON → Odds Ratio (OR)
| Feature | Detail |
|---|---|
| Direction | Outcome → Exposure (backward in time) |
| Best for | Rare diseases; quick & cheap |
| Measure | Odds Ratio (OR) |
| Limitation | Recall bias; selection of controls is tricky |
| Example | "Were people who developed contact dermatitis more exposed to fragrance moisturizers?" |
6. Cross-Sectional Study
POPULATION
│
▼
SINGLE POINT IN TIME (snapshot)
│
├── Exposed + Disease
├── Exposed + No Disease
├── Not Exposed + Disease
└── Not Exposed + No Disease
│
▼
PREVALENCE calculated
ASSOCIATION measured → Prevalence Ratio / OR
| Feature | Detail |
|---|---|
| Direction | No time dimension — simultaneous |
| Best for | Prevalence, surveys, diagnostic studies |
| Measure | Prevalence ratio |
| Limitation | Cannot establish causality (chicken-and-egg problem) |
| Example | "What proportion of adults with dry skin use moisturizers regularly?" |
7. Narrative Review
| Feature | Detail |
|---|---|
| Scope | Broad; expert curated |
| Search strategy | Not pre-registered or systematic |
| Best for | Overviews, educational articles, clinical summaries |
| Limitation | Subject to author bias; not reproducible |
| Example | "A review of moisturizer mechanisms in atopic dermatitis" |
8. Case Report
Patient Demographics / Background
│
▼
Chief Complaint + History
│
▼
Clinical Examination Findings
│
▼
Investigations (labs, imaging, biopsy)
│
▼
Diagnosis
│
▼
Treatment & Response
│
▼
Follow-up / Outcome
│
▼
DISCUSSION: Why is this case unique? What does it teach?
| Feature | Detail |
|---|---|
| N = 1 | Single patient only |
| Best for | Novel diagnoses, rare reactions, new treatments, teaching lessons |
| Hierarchy | Lowest level of evidence for causality |
| Limitation | Cannot generalize; no statistical analysis |
| Example | "Severe contact allergy to lanolin in a moisturizer — a case report" |
9. Case Series
| Feature | Detail |
|---|---|
| N = multiple | Usually 3–20 patients |
| Best for | Rare conditions, new procedures, initial safety signals |
| Hierarchy | Low evidence; no comparison group |
| Limitation | No controls; selection bias; cannot prove causality |
| Example | "A series of 10 patients with moisturizer-induced perioral dermatitis" |
10. Short Communication / Brief Report
| Feature | Detail |
|---|---|
| Length | 1500–2500 words, 1–2 tables/figures |
| Best for | Pilot results, focused observations, quick reports |
| Review | Peer-reviewed like full articles |
11. Editorial
| Feature | Detail |
|---|---|
| Author | Editor-in-chief, section editor, or invited expert |
| Purpose | Contextualize published research; provide perspective |
| Evidence level | Very low (opinion) |
| Not peer-reviewed | Usually invited, not externally reviewed |
12. Letter to the Editor
| Feature | Detail |
|---|---|
| Length | 150–500 words |
| Purpose | Critique, correct, or add to a published article |
| May include | Re-analysis, additional data, rebuttal |
| Example | Disagreement with the results of an RCT on a specific moisturizer formulation |
13. Commentary / Perspective
| Feature | Detail |
|---|---|
| Length | 800–1500 words |
| Author | Usually senior expert in field |
| Purpose | Frame a debate, discuss implications, offer expert standpoint |
14. Conference Abstract / Proceedings
| Feature | Detail |
|---|---|
| Length | 150–300 words |
| Peer-review | Limited / abstract-only review |
| Status | Preliminary; may later become a full paper |
| Limitation | Not fully peer-reviewed; data may change |
Evidence Hierarchy Pyramid
┌───────────────────────┐
│ SYSTEMATIC REVIEW │ ← Highest evidence
│ + META-ANALYSIS │
└──────────┬────────────┘
│
┌──────────▼────────────┐
│ RANDOMIZED CONTROLLED │
│ TRIAL (RCT) │
└──────────┬────────────┘
│
┌──────────▼────────────┐
│ COHORT STUDY │
│ (Prospective/Retro) │
└──────────┬────────────┘
│
┌──────────▼────────────┐
│ CASE-CONTROL STUDY │
└──────────┬────────────┘
│
┌──────────▼────────────┐
│ CROSS-SECTIONAL │
│ STUDY │
└──────────┬────────────┘
│
┌──────────▼────────────┐
│ CASE SERIES / │
│ CASE REPORT │
└──────────┬────────────┘
│
┌──────────▼────────────┐
│ EXPERT OPINION / │
│ EDITORIAL │ ← Lowest evidence
└───────────────────────┘
Comparison Summary Table
| Article Type | Study Design | Evidence Level | Key Measure | Best Use |
|---|---|---|---|---|
| Meta-Analysis | Statistical pooling | ⭐⭐⭐⭐⭐ | Pooled OR/RR | Definitive effect size |
| Systematic Review | Synthesis | ⭐⭐⭐⭐⭐ | Qualitative/Quantitative | Evidence summary |
| RCT | Experimental | ⭐⭐⭐⭐ | Risk difference | Treatment efficacy |
| Cohort | Observational, prospective | ⭐⭐⭐ | Relative Risk (RR) | Risk factors, prognosis |
| Case-Control | Observational, retrospective | ⭐⭐ | Odds Ratio (OR) | Rare diseases |
| Cross-Sectional | Observational, snapshot | ⭐⭐ | Prevalence | Prevalence, surveys |
| Narrative Review | Synthesis (non-systematic) | ⭐ | Descriptive | Overview, education |
| Case Series | Descriptive | ⭐ | Descriptive | Rare conditions |
| Case Report | Descriptive | ⭐ | Descriptive | Unique presentations |
| Editorial | Opinion | — | Opinion | Context, debate |
| Letter | Opinion/brief data | — | Critique | Response to papers |
Key Acronyms You Will Encounter
| Acronym | Meaning | Used In |
|---|---|---|
| PICO | Population, Intervention, Comparison, Outcome | Systematic reviews, RCTs |
| CONSORT | Consolidated Standards of Reporting Trials | RCTs |
| PRISMA | Preferred Reporting Items for Systematic Reviews | Systematic reviews |
| STROBE | Strengthening the Reporting of Observational Studies | Cohort, case-control, cross-sectional |
| CARE | CAse REport guidelines | Case reports |
| GRADE | Grading of Recommendations Assessment | Evidence quality rating |
| RoB | Risk of Bias | Cochrane tool for RCT quality |
| NOS | Newcastle-Ottawa Scale | Quality of observational studies |
| OR | Odds Ratio | Case-control studies |
| RR | Relative Risk | Cohort studies |
| HR | Hazard Ratio | Survival/time-to-event analyses |
| CI | Confidence Interval | All quantitative studies |
| I² | Heterogeneity statistic | Meta-analyses |
make it ppt
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or does not exist"
mkdir -p /home/daytona/workspace/journal-articles-ppt && echo "created"
~/journal-articles-ppt/make_ppt.js
const pptxgen = require('pptxgenjs');
const pptx = new pptxgen();
pptx.layout = 'LAYOUT_WIDE';
pptx.author = 'Orris';
pptx.company = 'Orris';
pptx.subject = 'Types of Journal Articles';
pptx.title = 'Types of Journal Articles - Detailed Guide';
pptx.lang = 'en-US';
pptx.theme = {
headFontFace: 'Calibri',
bodyFontFace: 'Calibri',
lang: 'en-US'
};
const COLORS = {
bg: '0B1020',
card: '121A33',
accent: '3B82F6',
accent2: '14B8A6',
text: 'E6ECFF',
muted: 'A8B3CF',
white: 'FFFFFF'
};
function addHeader(slide, title, subtitle='') {
slide.background = { color: COLORS.bg };
slide.addShape(pptx.ShapeType.rect, {
x: 0, y: 0, w: 13.33, h: 0.7,
fill: { color: '0F1730' },
line: { color: '0F1730' }
});
slide.addText(title, {
x: 0.45, y: 0.14, w: 9.8, h: 0.35,
color: COLORS.text, bold: true, fontSize: 20, margin: 0
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.45, y: 0.5, w: 11.8, h: 0.25,
color: COLORS.muted, fontSize: 11, margin: 0
});
}
}
function addFooter(slide, n) {
slide.addShape(pptx.ShapeType.line, {
x: 0.45, y: 7.08, w: 12.4, h: 0,
line: { color: '233054', pt: 1 }
});
slide.addText(`Journal Article Types | Slide ${n}`, {
x: 0.45, y: 7.14, w: 12.4, h: 0.2,
color: '7F8DB2', fontSize: 9, align: 'right'
});
}
function addCard(slide, x, y, w, h, title, body, accent='3B82F6') {
slide.addShape(pptx.ShapeType.roundRect, {
x, y, w, h,
rectRadius: 0.06,
fill: { color: COLORS.card },
line: { color: '243357', pt: 1 }
});
slide.addShape(pptx.ShapeType.rect, {
x, y, w: 0.08, h,
fill: { color: accent }, line: { color: accent }
});
slide.addText(title, {
x: x + 0.18, y: y + 0.1, w: w - 0.24, h: 0.3,
color: COLORS.white, bold: true, fontSize: 14, margin: 0
});
slide.addText(body, {
x: x + 0.18, y: y + 0.45, w: w - 0.24, h: h - 0.5,
color: COLORS.text, fontSize: 11, valign: 'top'
});
}
// Slide 1: Title
{
const s = pptx.addSlide();
s.background = { color: COLORS.bg };
s.addShape(pptx.ShapeType.rect, {
x: 0.7, y: 1.0, w: 12.0, h: 5.2,
fill: { color: '111A35' }, line: { color: '243357', pt: 1 }
});
s.addText('Types of Journal Articles', {
x: 1.1, y: 2.0, w: 11.0, h: 0.9,
color: COLORS.white, bold: true, fontSize: 46, align: 'center'
});
s.addText('Detailed Guide with Study Designs, Evidence Hierarchy, and Use Cases', {
x: 1.1, y: 3.05, w: 11.0, h: 0.45,
color: COLORS.muted, fontSize: 18, align: 'center'
});
s.addShape(pptx.ShapeType.roundRect, {
x: 4.65, y: 4.15, w: 4.0, h: 0.55,
fill: { color: COLORS.accent }, line: { color: COLORS.accent }, rectRadius: 0.08
});
s.addText('Medical / Scientific Publishing', {
x: 4.8, y: 4.3, w: 3.7, h: 0.25,
color: COLORS.white, fontSize: 12, bold: true, align: 'center'
});
addFooter(s, 1);
}
// Slide 2: Classification overview
{
const s = pptx.addSlide();
addHeader(s, 'High-Level Classification', 'How journal articles are grouped');
addCard(s, 0.6, 1.0, 4.1, 2.5, 'Primary Research',
`Original data collection\n• Experimental: RCT, quasi-experimental, lab studies\n• Observational: cohort, case-control, cross-sectional\n\nAnswers: What happened in this specific sample?`, COLORS.accent);
addCard(s, 4.9, 1.0, 4.1, 2.5, 'Secondary Research',
`Synthesis of existing studies\n• Systematic review\n• Meta-analysis\n• Narrative review\n\nAnswers: What is the totality of evidence?`, '14B8A6');
addCard(s, 9.2, 1.0, 3.5, 2.5, 'Scholarly Discourse',
`Opinion and critique formats\n• Editorial\n• Letter\n• Commentary\n• Perspective`, 'F59E0B');
addCard(s, 0.6, 3.8, 12.1, 2.8, 'Flow Map',
`Journal Articles\n ├── Primary Research\n │ ├── Experimental -> RCT / Non-randomized / Lab\n │ └── Observational -> Cohort / Case-control / Cross-sectional\n ├── Secondary Research -> Systematic Review / Meta-analysis / Narrative Review\n ├── Special Reports -> Case report / Case series / Brief report / Conference abstract\n └── Opinion -> Editorial / Letter / Commentary`, '8B5CF6');
addFooter(s, 2);
}
// Slide 3: RCT
{
const s = pptx.addSlide();
addHeader(s, 'Randomized Controlled Trial (RCT)', 'Best design to evaluate treatment efficacy');
addCard(s, 0.6, 1.0, 6.2, 2.3, 'Core Structure',
`Population -> Randomization -> Intervention vs Control -> Outcome comparison\nBlinding: single, double, or triple\nReporting standard: CONSORT`, COLORS.accent);
addCard(s, 7.0, 1.0, 5.7, 2.3, 'Strengths & Limits',
`Strengths: strong internal validity, lower confounding\nLimits: cost, logistics, ethics, external validity challenges`, '14B8A6');
addCard(s, 0.6, 3.5, 12.1, 3.0, 'Flowchart',
`Eligible participants\n ↓\nRandom allocation\n ↙ ↘\nIntervention Control (placebo/standard care)\n ↓ ↓\nOutcome A Outcome B\n ↓\nBetween-group effect estimate (RR, ARR, NNT, CI)`, 'F59E0B');
addFooter(s, 3);
}
// Slide 4: Observational studies
{
const s = pptx.addSlide();
addHeader(s, 'Observational Designs', 'Cohort, Case-control, and Cross-sectional');
addCard(s, 0.6, 1.0, 4.0, 5.8, 'Cohort Study',
`Direction: Exposure -> Outcome\nProspective or retrospective\nMeasure: Relative Risk (RR)\nBest for: incidence, prognosis, risk factors\nLimitation: follow-up burden`, COLORS.accent);
addCard(s, 4.8, 1.0, 4.0, 5.8, 'Case-Control Study',
`Direction: Outcome -> Exposure (backward)\nMeasure: Odds Ratio (OR)\nBest for: rare diseases\nFast and cost-effective\nLimitations: recall & selection bias`, '14B8A6');
addCard(s, 9.0, 1.0, 3.7, 5.8, 'Cross-Sectional Study',
`Snapshot at one time point\nExposure and outcome measured together\nBest for: prevalence estimates\nLimitation: cannot establish temporality/causality`, 'F59E0B');
addFooter(s, 4);
}
// Slide 5: Secondary evidence
{
const s = pptx.addSlide();
addHeader(s, 'Systematic Review and Meta-Analysis', 'Highest-level evidence synthesis');
addCard(s, 0.6, 1.0, 6.2, 2.6, 'Systematic Review',
`Structured question (PICO)\nProtocol-driven search across databases\nScreening + quality appraisal + synthesis\nReporting standard: PRISMA`, COLORS.accent);
addCard(s, 7.0, 1.0, 5.7, 2.6, 'Meta-analysis',
`Quantitatively pools effect sizes from multiple studies\nOutputs: pooled effect, 95% CI, forest plot, I² heterogeneity\nRisk: garbage-in, garbage-out if source studies are weak`, '14B8A6');
addCard(s, 0.6, 3.9, 12.1, 2.7, 'Workflow',
`Question -> Search -> Screen -> Full-text eligibility -> Risk-of-bias assessment\n-> Data extraction -> Qualitative synthesis\n-> (Optional) Quantitative pooling (meta-analysis) -> GRADE certainty`, '8B5CF6');
addFooter(s, 5);
}
// Slide 6: Case report / case series
{
const s = pptx.addSlide();
addHeader(s, 'Case Report and Case Series', 'Useful for rare or novel clinical observations');
addCard(s, 0.6, 1.0, 6.0, 2.7, 'Case Report (N=1)',
`Detailed narrative of one patient\nIncludes: presentation, diagnostics, treatment, outcome\nBest for: rare events, new adverse effects, educational insights\nGuideline: CARE`, COLORS.accent);
addCard(s, 6.8, 1.0, 5.9, 2.7, 'Case Series (N>1)',
`Multiple similar cases without control group\nDetects early patterns and safety signals\nLimit: descriptive only, no causal inference`, '14B8A6');
addCard(s, 0.6, 4.0, 12.1, 2.5, 'Typical Case Report Structure',
`Patient profile -> History -> Examination -> Investigations -> Diagnosis\n-> Intervention -> Follow-up -> Learning points`, 'F59E0B');
addFooter(s, 6);
}
// Slide 7: Editorial/letter/commentary
{
const s = pptx.addSlide();
addHeader(s, 'Editorial, Letter, Commentary, Perspective', 'Scholarly interpretation and debate formats');
addCard(s, 0.6, 1.0, 3.0, 4.8, 'Editorial',
`Invited expert view\nFrames clinical significance\nUsually not original data`, COLORS.accent);
addCard(s, 3.8, 1.0, 3.0, 4.8, 'Letter',
`Brief response to published work\nCritique, clarification, or reanalysis\nCan trigger post-publication review`, '14B8A6');
addCard(s, 7.0, 1.0, 2.8, 4.8, 'Commentary',
`Focused interpretation of a topic\nDiscusses policy or practice implications`, 'F59E0B');
addCard(s, 10.0, 1.0, 2.7, 4.8, 'Perspective',
`Argumentative expert viewpoint\nOften future-facing recommendations`, '8B5CF6');
addCard(s, 0.6, 6.0, 12.1, 0.7, 'Note',
`These formats are valuable for context and critique but rank lower than controlled empirical studies for causal evidence.`, 'EF4444');
addFooter(s, 7);
}
// Slide 8: Evidence hierarchy
{
const s = pptx.addSlide();
addHeader(s, 'Evidence Hierarchy Pyramid', 'From highest certainty to lowest');
const levels = [
{ t: 'Systematic Review + Meta-analysis', c: '2563EB', w: 8.6 },
{ t: 'Randomized Controlled Trial', c: '1D4ED8', w: 7.5 },
{ t: 'Cohort Study', c: '0EA5E9', w: 6.4 },
{ t: 'Case-Control Study', c: '14B8A6', w: 5.3 },
{ t: 'Cross-Sectional Study', c: '22C55E', w: 4.2 },
{ t: 'Case Series / Case Report', c: 'F59E0B', w: 3.1 },
{ t: 'Editorial / Expert Opinion', c: 'EF4444', w: 2.0 }
];
let y = 1.1;
levels.forEach((lv, i) => {
const x = (13.33 - lv.w) / 2;
s.addShape(pptx.ShapeType.roundRect, {
x, y, w: lv.w, h: 0.65,
fill: { color: lv.c }, line: { color: lv.c }, rectRadius: 0.05
});
s.addText(lv.t, {
x, y: y + 0.16, w: lv.w, h: 0.3,
color: 'FFFFFF', bold: true, align: 'center', fontSize: 14
});
y += 0.72;
});
addFooter(s, 8);
}
// Slide 9: Reporting checklists and key metrics
{
const s = pptx.addSlide();
addHeader(s, 'Reporting Standards and Key Metrics', 'How quality and effect are communicated');
addCard(s, 0.6, 1.0, 6.0, 2.9, 'Reporting Guidelines',
`CONSORT - randomized trials\nPRISMA - systematic reviews/meta-analyses\nSTROBE - observational studies\nCARE - case reports\nGRADE - certainty of evidence`, COLORS.accent);
addCard(s, 6.8, 1.0, 5.9, 2.9, 'Common Statistics',
`OR: Odds Ratio\nRR: Relative Risk\nHR: Hazard Ratio\nCI: Confidence Interval\nI²: heterogeneity in meta-analysis`, '14B8A6');
addCard(s, 0.6, 4.2, 12.1, 2.4, 'Quick Interpretation Rule',
`Strong publication quality = robust design + transparent reporting + appropriate statistics + reproducibility cues.`, '8B5CF6');
addFooter(s, 9);
}
// Slide 10: Final comparison matrix
{
const s = pptx.addSlide();
addHeader(s, 'Comparison Matrix', 'Design, strength, and use case in one view');
const headers = ['Type', 'Design', 'Evidence', 'Primary Use'];
const rows = [
['Meta-analysis', 'Secondary (quantitative)', 'Very High', 'Pooled treatment effect'],
['Systematic Review', 'Secondary (structured)', 'Very High', 'Total evidence synthesis'],
['RCT', 'Experimental', 'High', 'Intervention efficacy'],
['Cohort', 'Observational', 'Moderate', 'Risk/prognosis'],
['Case-control', 'Observational', 'Moderate-Low', 'Rare disease associations'],
['Cross-sectional', 'Observational snapshot', 'Low-Moderate', 'Prevalence'],
['Case report/series', 'Descriptive', 'Low', 'Novel signal detection'],
['Editorial/Letter', 'Opinion/critique', 'Contextual', 'Debate and interpretation']
];
s.addTable([headers, ...rows], {
x: 0.6, y: 1.1, w: 12.1, h: 5.9,
border: { type: 'solid', pt: 1, color: '2A3A63' },
fill: '121A33',
color: 'E6ECFF',
fontFace: 'Calibri',
fontSize: 11,
rowH: 0.62,
valign: 'middle',
margin: 0.06,
colW: [2.6, 3.1, 2.0, 4.4],
autoFit: false,
align: 'left',
bold: false,
cellProps: {
0: { fill: '1F2D52', bold: true, color: 'FFFFFF', fontSize: 12 }
}
});
addFooter(s, 10);
}
pptx.writeFile({ fileName: '/home/daytona/workspace/journal-articles-ppt/Journal_Article_Types_Detailed.pptx' });
node "/home/daytona/workspace/journal-articles-ppt/make_ppt.js" && ls -la "/home/daytona/workspace/journal-articles-ppt/"
Journal Article Types Detailed
Presentation · PPTX