Caplan syndrome for md exams 10 marks answer from fishman and murray only
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the key content from both Fishman's Pulmonary Diseases and Murray & Nadel's. Let me compile the comprehensive 10-mark answer.
Caplan Syndrome - 10 Marks Answer (Fishman & Murray & Nadel)
Definition
Caplan syndrome (also called rheumatoid pneumoconiosis) refers to the radiographic abnormality of large, discrete pulmonary nodules arising in workers who have both rheumatoid arthritis (RA) and pneumoconiosis. It was first described by Dr. A. Caplan in 1953 in Welsh coal miners suffering from rheumatoid arthritis (Caplan A. Thorax 1953;8:29-37).
"Caplan syndrome refers to a radiographic abnormality that developed in Welsh coal miners with rheumatoid arthritis and a pneumoconiosis. It consists of the sudden appearance of discrete nodules primarily in the upper lobes that are histologically identical to the necrobiotic nodule."
- Fishman's Pulmonary Diseases and Disorders
Historical Background
- First described by Anthony Caplan in Welsh coal miners in 1953
- Subsequently recognised in patients with silicosis, asbestosis, and other forms of pneumoconiosis
- The original term "rheumatoid pneumoconiosis" continues to be used interchangeably
Occupational Associations (Dust Exposures)
Caplan syndrome has been described with exposure to:
- Coal mine dust - Coal workers' pneumoconiosis (CWP) - the classical association
- Silica dust - Silicosis (hard-rock miners, foundry workers)
- Asbestos - Asbestosis
- Also described in farming, quarrying, construction, bricklaying, and electrical work
"Rheumatoid arthritis (with elevated anti-citrullinated protein antibody) with silica exposure (Caplan's syndrome); farming; mining; quarrying; electrical work; construction"
- Firestein & Kelley's Textbook of Rheumatology
Epidemiology / Incidence
- Uncommon: observed in less than 1% of autopsied cases of coal mine dust lung disease (CMDLD)
- More common in men with seropositive RA (high rheumatoid factor titers, subcutaneous nodules)
- Immunologic data: in studies of U.S. coal miners with CWP, elevated ANA (up to 27% in category C PMF) and rheumatoid factor (up to 18%) indicate significant immune activation in miners with pneumoconiosis
Pathogenesis
The precise mechanism involves an interaction between:
- Inhaled dust particles that are engulfed by alveolar macrophages and accumulate in airway walls and interstitium when clearance mechanisms are overwhelmed
- Rheumatoid immune dysregulation - the macrophage-driven granulomatous response is amplified by the presence of circulating rheumatoid factor and anti-citrullinated protein antibodies (ACPA)
- Immunologic activation: studies (Soutar et al.) showed elevated ANA in 17% and RF in 10% of miners with radiographic pneumoconiosis; elevated serum immunoglobulins (C3, IgA, IgG, alpha-1-antitrypsin) found particularly in those with anthracite coal mining history
- The result is a necrotising granulomatous nodule - histologically identical to the subcutaneous rheumatoid nodule, with a central zone of fibrinoid necrosis surrounded by palisading histiocytes and peripheral fibrosis
Pathology
- Nodules are histologically identical to necrobiotic (rheumatoid) nodules
- Central zone: fibrinoid necrosis with dust pigmentation and cholesterol clefts
- Surrounding zone: palisading macrophages/histiocytes
- Outer zone: fibrous capsule with lymphocytic infiltrate
- Nodules may contain dust particles embedded within the necrotic center
- Distinguishing feature from PMF: Caplan nodules develop rapidly and appear as discrete, well-defined lesions against a background that may have relatively little simple CWP change
Radiological Features
Chest X-ray:
- Sudden appearance of multiple, discrete, well-defined rounded nodules
- Size: 5 to 50 mm in diameter (Murray & Nadel)
- Predominantly in upper and mid zones (upper-lobe predilection)
- Typically bilateral
- Background of small pneumoconiotic opacities may or may not be prominent - nodules may appear without a background of smaller opacities (distinguishing from PMF)
- Nodules may cavitate (~50% of necrobiotic nodules undergo cavitation due to proteolytic enzymes)
- Spontaneous resolution and recurrence can occur
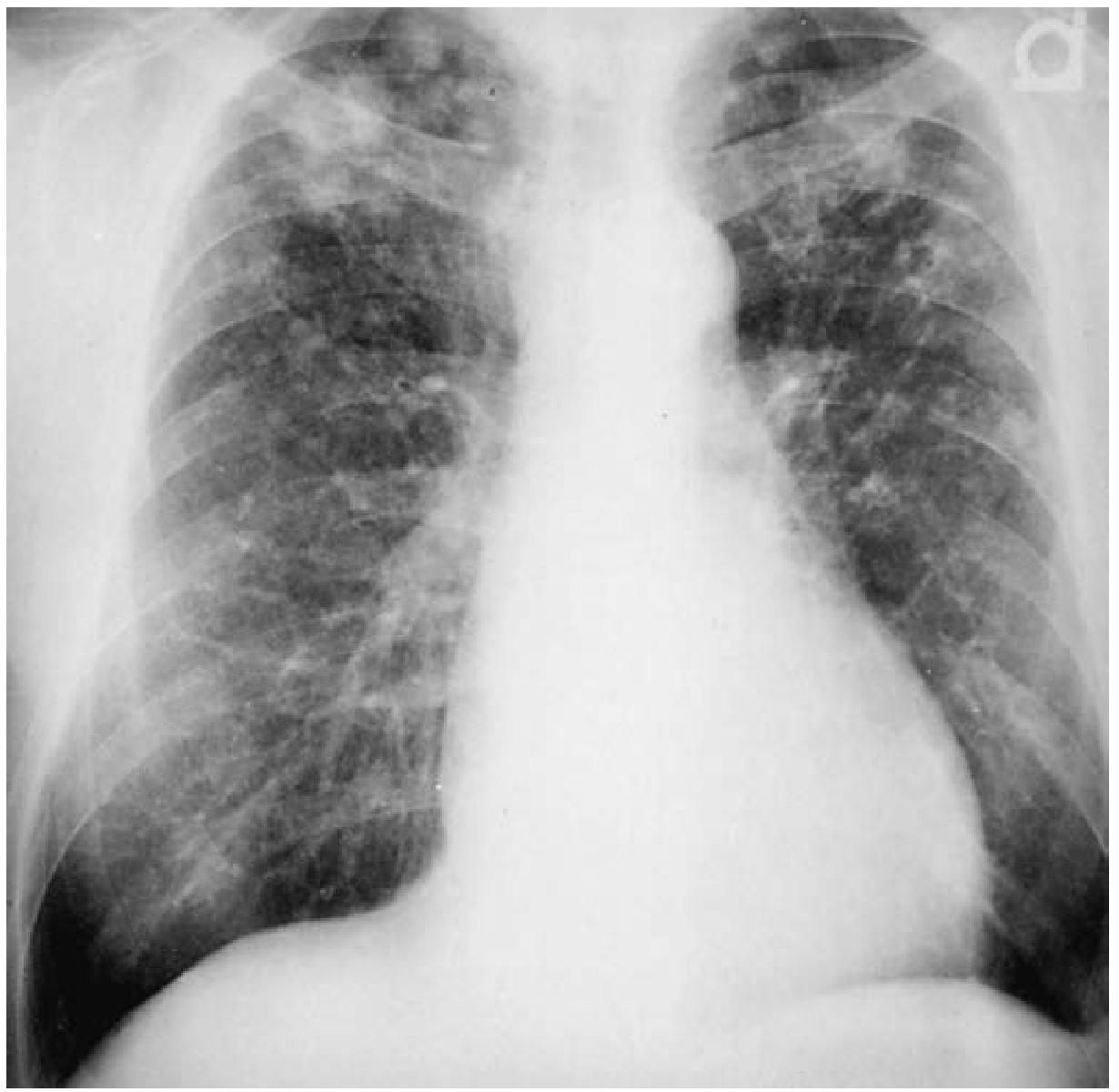
Figure 58-13 (Fishman's): Caplan syndrome in a patient with RA and silicosis (hard-rock miner). Multiple small nodules in the middle and upper lung representing silicosis. In addition, multiple upper-zone rheumatoid nodules are present.
"The chest radiograph typically demonstrates large, well-defined nodules or masses, ranging from 5 to 50 mm in diameter, typically without a background of smaller opacities."
- Murray & Nadel's Textbook of Respiratory Medicine
Clinical Features
- Nodules are primarily a radiographic finding and largely asymptomatic in most patients
- The underlying rheumatoid arthritis is seropositive (RF positive, often ACPA positive)
- Articular symptoms of RA may precede, coexist with, or follow the pulmonary nodules
- Complications of nodules:
- Cavitation - may suggest superimposed infection (TB, fungal)
- Pneumothorax - from rupture of cavitated nodule (requires tube thoracostomy)
- Pleural effusion - from rupture into pleural space
- Hemoptysis - rare
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Progressive massive fibrosis (PMF) | Large confluent masses (>2 cm), background simple CWP present, no RA |
| Pulmonary tuberculosis | AFB positive, cavitation usually upper lobe, single or few lesions |
| Fungal infections (histoplasmosis, cryptococcosis) | Serologic/culture positivity, epidemiologic exposure |
| Lung cancer (primary bronchogenic) | Rapid growth, FDG-avid on PET, unilateral, no RA/dust background |
| Simple necrobiotic RA nodules | No dust exposure history, smaller, less numerous |
"Pulmonary tuberculosis and fungal infections may need to be considered in some cases, particularly when nodules cavitate."
- Murray & Nadel's Textbook of Respiratory Medicine
"The major problem is differentiating the necrobiotic nodule from either malignant or infectious granulomatous disease, particularly given the increased risk of lung cancer in patients with RA."
- Fishman's Pulmonary Diseases and Disorders
Diagnosis
- Clinical: combination of seropositive RA + dust exposure history + characteristic CXR
- Serology: positive rheumatoid factor, elevated ACPA
- HRCT thorax: better delineates nodule characteristics, detects cavitation, identifies background pneumoconiosis
- Biopsy (if needed): shows histology of necrotising rheumatoid nodule with embedded dust particles
- No specific laboratory test exists for CMDLD, but elevated ANA, RF, or ACE may be found
Management
- No specific treatment is required for the nodules themselves in most cases
- Treatment of underlying RA - DMARDs (methotrexate, biologics): treatment of the underlying rheumatoid disease frequently results in improvement in pulmonary nodules
- Dust exposure cessation - removal from occupational exposure
- Complications: cavitated nodules with bronchopleural fistula require surgical intervention; pneumothorax requires tube thoracostomy
- Surveillance: continuous nodule growth must prompt aggressive diagnostic workup (biopsy to exclude malignancy)
- Monitor for increased risk of mycobacterial infections in the setting of pneumoconiosis and RA
Key Points for Exam
| Feature | Detail |
|---|---|
| First described | Caplan, Welsh coal miners, 1953 |
| Classic triad | Seropositive RA + Pneumoconiosis + Upper-lobe nodules |
| Nodule size | 5-50 mm |
| Histology | Identical to necrobiotic (subcutaneous RA) nodule |
| Background opacities | May be absent (unlike PMF) |
| Cavitation | ~50% of necrobiotic nodules |
| Incidence | <1% of autopsied CMDLD cases |
| Dusts implicated | Coal, silica, asbestos |
| Treatment | Treat underlying RA; no specific nodule therapy |
Sources:
- Fishman's Pulmonary Diseases and Disorders, 5th Ed. - Chapter 58 (Rheumatoid Arthritis, pp. 1025-1026) and Chapter on Coal Mine Dust Lung Disease (Biology section, p. 1548)
- Murray & Nadel's Textbook of Respiratory Medicine, 7th Ed. - Chapter 101 (Coal Mine Dust Lung Disease), Section: Rheumatoid Pneumoconiosis, p. 2349
This is a shared conversation. Sign in to Orris to start your own chat.