Phenytoin
Reading File
Finding Sources
Searching PubMed
phenytoin antiepileptic
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated response. Here is the full summary:
Phenytoin
Class: Hydantoin antiseizure medication (ASM)
Also known as: Diphenylhydantoin (DPH)
First identified: 1938 - the oldest non-sedating antiseizure drug
Structure & Formulations
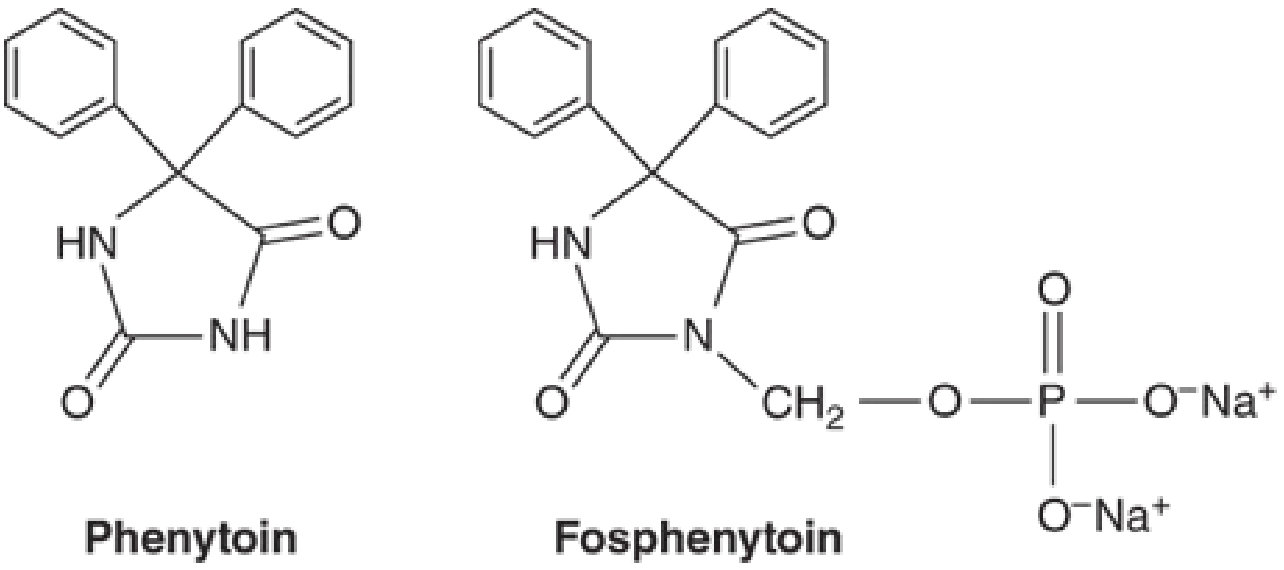
Phenytoin is the 5,5-diphenyl-substituted analog of hydantoin - a five-membered ring structurally similar to barbiturates (six-membered ring). The free base (pKa 8.06-8.33) is poorly water-soluble; phenytoin sodium dissolves in water at 17 mg/mL.
Available formulations:
| Form | Absorption characteristics |
|---|---|
| Extended-release capsule (phenytoin sodium) | Peak level 4-12 h; allows once-daily dosing |
| Prompt capsule (phenytoin sodium) | Peak level 1.5-3 h; requires more frequent dosing |
| Suspension & chewable tablets (free base) | Immediate-release |
| IV solution (pH 12, propylene glycol + alcohol) | Risk of purple glove syndrome; rate ≤50 mg/min |
| Fosphenytoin (IV/IM prodrug) | Water-soluble; converted by phosphatases in liver/RBCs; t½ conversion = 8-15 min; preferred over IV phenytoin |
IM administration of phenytoin (not fosphenytoin) is not recommended - absorption is unpredictable and precipitation in muscle occurs.
Mechanism of Action
Phenytoin is a voltage-gated sodium channel blocker. It slows the rate of recovery of Na⁺ channels from inactivation, making it both:
- Voltage-dependent - greater effect when the membrane is depolarized
- Use-dependent - greater effect with repetitive firing
At therapeutic concentrations, phenytoin selectively limits repetitive high-frequency action potential firing without affecting basal neuronal activity or responses to GABA/glutamate. At 5-10x therapeutic concentrations, additional effects emerge (GABA enhancement, reduced spontaneous activity), which underlie phenytoin toxicity.
"Phenytoin limits the repetitive firing of action potentials evoked by a sustained depolarization... This effect is mediated by a slowing of the rate of recovery of voltage-activated Na⁺ channels from inactivation." - Goodman & Gilman's, p. 411
Clinical Uses
Effective for:
- Focal (partial) onset seizures
- Focal-to-bilateral tonic-clonic seizures
- Generalized tonic-clonic seizures (including in idiopathic generalized epilepsy)
- Acute treatment of status epilepticus (IV/fosphenytoin)
May worsen:
- Absence seizures
- Juvenile myoclonic epilepsy (JME)
- Dravet syndrome
- Myoclonic seizures
Due to its adverse effects and drug interactions, phenytoin is no longer considered first-line chronic therapy, though it remains important for status epilepticus.
Pharmacokinetics
Absorption
- Highly formulation-dependent (particle size, excipients matter)
- Absorption from GI tract nearly complete in most patients; time to peak ranges from 3-12 hours
Protein Binding
- ~90% bound to serum albumin
- Small changes in the bound fraction dramatically alter free (active) drug
- Displacement occurs with: hyperbilirubinemia, warfarin, valproate, sulfonamides, phenylbutazone
- Low albumin states (liver disease, nephrotic syndrome, neonates, elderly) → elevated free drug → toxicity even at "therapeutic" total levels
Volume of distribution
- Low Vd = 0.6-0.7 L/kg in adults (due to high protein binding)
Metabolism
- 95% metabolized in hepatic ER by CYP2C9/2C10 (primarily) and CYP2C19
- Principal metabolite: parahydroxyphenyl derivative (inactive)
- Only a small proportion excreted unchanged in urine
Nonlinear (Zero-Order / Michaelis-Menten) Kinetics - KEY CONCEPT
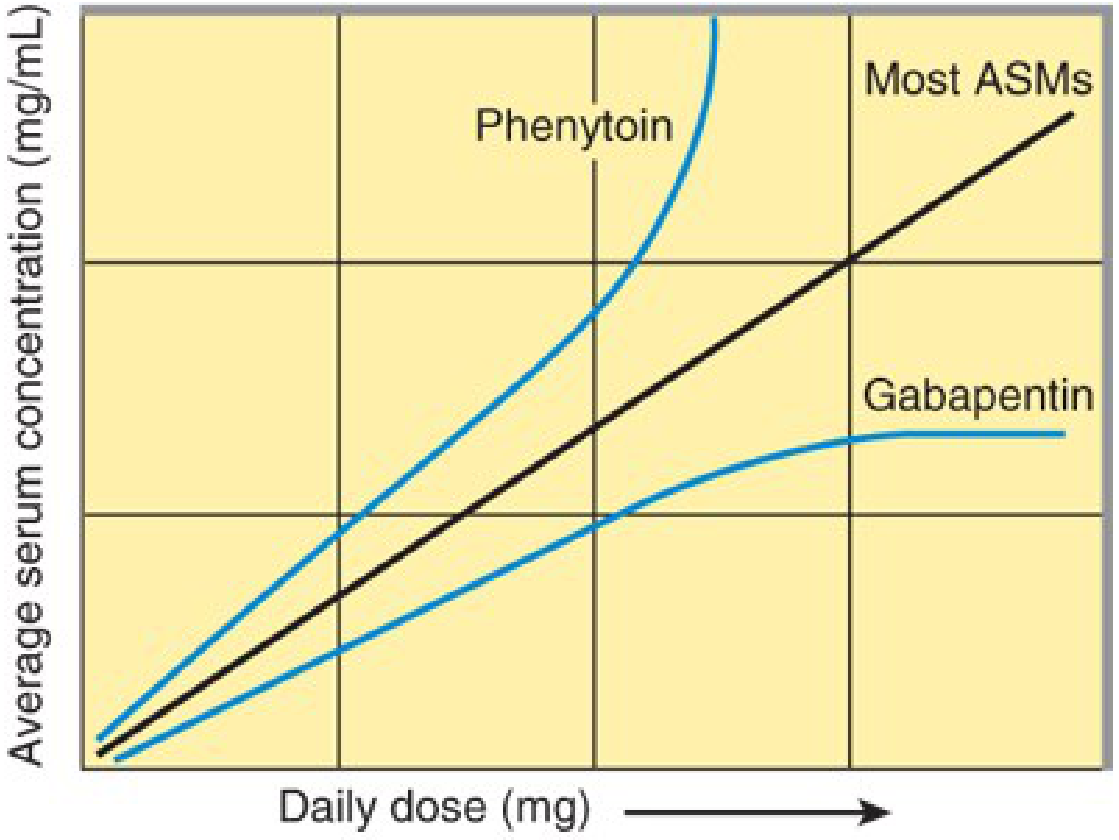
At low levels: first-order kinetics (constant fraction eliminated per unit time). As levels rise within the therapeutic range, hepatic metabolism becomes saturated, shifting to zero-order kinetics (constant amount eliminated per unit time). This means:
- Small dose increases → disproportionately large rise in serum level
- Half-life increases markedly at higher concentrations (t½ = 12-36 h average; much longer at high levels)
- Steady state after a dose change takes 5-7 days at low-mid levels, and 4-6 weeks at higher levels
- Therapeutic drug monitoring (TDM) is essential
Therapeutic range (total): 10-20 mcg/mL
Free phenytoin therapeutic range: 1-2 mcg/mL
Free phenytoin therapeutic range: 1-2 mcg/mL
Correction for hypoalbuminemia (Winter-Tozer equation): Corrected level = measured total ÷ [(0.2 × albumin) + 0.1]
Enzyme Induction
Phenytoin is a major CYP inducer (CYP1A2, CYP2C, CYP3A4). Clinically important inductions include:
- Oral contraceptives (CYP3A4) → contraceptive failure → unplanned pregnancy (especially dangerous given phenytoin's teratogenicity)
- Warfarin (CYP2C9) → reduces anticoagulant effect initially, but phenytoin also displaces warfarin from proteins - complex interaction
- Valproate, tiagabine, ethosuximide, lamotrigine, topiramate, oxcarbazepine
Drug Interactions
Drugs that INCREASE phenytoin levels (CYP2C9/2C19 inhibitors):
- Isoniazid (especially in slow acetylators)
- Fluoxetine, fluvoxamine
- Metronidazole
- Miconazole
- Omeprazole
- Valproate (also displaces from protein binding)
- Fluorouracil
- Sulfonamides
Drugs that DECREASE phenytoin levels:
- Alcohol (chronic use), barbiturates, carbamazepine (CYP inducers → increased metabolism)
- Antacids (reduce absorption)
Phenytoin REDUCES levels of:
- Oral contraceptives
- Warfarin
- Most other ASMs (valproate, lamotrigine, topiramate, tiagabine)
- Corticosteroids, cyclosporine, some antibiotics
Adverse Effects
Dose-Related (CNS) - most common
| Level (mcg/mL) | Signs |
|---|---|
| 10-20 (therapeutic) | Mild sedation in some |
| 20-30 | Nystagmus (horizontal) |
| 30-40 | Ataxia, dysarthria, diplopia |
| >40 | Mental confusion, lethargy, encephalopathy |
| Very high | Paradoxical seizure worsening, decerebrate rigidity |
Chronic Use Effects
- Gingival hyperplasia - occurs in ~20% of patients; due to altered collagen metabolism; especially problematic in children
- Hirsutism - particularly distressing in women
- Coarsening of facial features
- Peripheral neuropathy - diminished deep tendon reflexes
- Cerebellar atrophy - with high chronic doses
- Megaloblastic anemia - due to folate interference
- Osteomalacia / decreased bone density - via induction of vitamin D metabolism (CYP3A4)
- Behavioral changes
Cardiovascular (IV administration)
- Cardiac arrhythmias with hypotension when infused too rapidly - minimize by infusing phenytoin at ≤50 mg/min (or fosphenytoin at ≤150 mg phenytoin equivalents/min)
- Greater risk in elderly and those with cardiac disease, but can occur in young healthy patients
- Purple glove syndrome - purplish-black discoloration + edema + pain distal to injection site; fosphenytoin has lower incidence
Idiosyncratic / Hypersensitivity (drug allergy)
- Skin reactions: rash, Stevens-Johnson syndrome (rare)
- Bone marrow suppression (rare)
- Hepatotoxicity (rare)
- These require drug withdrawal
Teratogenicity - Fetal Hydantoin Syndrome
- Craniofacial abnormalities, limb defects, growth retardation, cognitive impairment
- Use during pregnancy requires careful risk-benefit assessment; folate supplementation is recommended
Special Situations
Hypoalbuminemia / Renal failure:
Report free phenytoin levels rather than total. In uremia, not only is albumin reduced, but the protein binding affinity is also decreased - total levels are misleading. Use the Winter-Tozer correction formula.
Report free phenytoin levels rather than total. In uremia, not only is albumin reduced, but the protein binding affinity is also decreased - total levels are misleading. Use the Winter-Tozer correction formula.
Status Epilepticus:
Use IV fosphenytoin (preferred over phenytoin IV due to safety profile). Dosing as "phenytoin equivalents" (PE): loading dose 15-20 mg PE/kg IV.
Use IV fosphenytoin (preferred over phenytoin IV due to safety profile). Dosing as "phenytoin equivalents" (PE): loading dose 15-20 mg PE/kg IV.
Drug-drug interactions in ICU:
Phenytoin is notorious for complex interactions with antibiotics, antifungals, and sedatives used in critically ill patients.
Phenytoin is notorious for complex interactions with antibiotics, antifungals, and sedatives used in critically ill patients.
Summary Table
| Property | Value |
|---|---|
| Class | Hydantoin |
| Mechanism | Voltage-gated Na⁺ channel blockade |
| Seizure types | Focal, focal-to-bilateral tonic-clonic, generalized tonic-clonic; IV for status epilepticus |
| Protein binding | ~90% (albumin) |
| Vd | 0.6-0.7 L/kg |
| Metabolism | CYP2C9 >> CYP2C19 (hepatic); zero-order (saturation) kinetics |
| Half-life | 12-36 h (average 24 h; longer at high levels) |
| Therapeutic range | Total: 10-20 mcg/mL; Free: 1-2 mcg/mL |
| Key adverse effects | Nystagmus → ataxia → encephalopathy; gingival hyperplasia; hirsutism; teratogenicity |
| Key interactions | CYP2C9/2C19 inhibitors ↑ levels; phenytoin induces CYP3A4 ↓ OCP/warfarin |
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 651-652
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 411-413
- Tietz Textbook of Laboratory Medicine, 7th Ed.
Recent evidence note (2025): A network meta-analysis in Neurology (PMID 39808752) comparing antiseizure medications for post-stroke seizures, and NCS guidelines on seizure prophylaxis in intracerebral hemorrhage (PMID 39707127), both suggest that phenytoin/fosphenytoin is being replaced by levetiracetam and newer agents in acute neurocritical care settings due to its interaction profile and adverse effects - consistent with its declining role as a first-line agent.
Summarise it
Phenytoin - Summary
Class: Hydantoin antiseizure drug (oldest non-sedating AED, since 1938)
Mechanism: Blocks voltage-gated Na⁺ channels - slows recovery from inactivation, limiting repetitive high-frequency neuronal firing.
Uses
- Focal seizures, tonic-clonic seizures, status epilepticus (IV)
- Avoid in: absence seizures, JME, Dravet syndrome (can worsen them)
- No longer first-line for chronic epilepsy
Key Pharmacokinetics
- Protein binding: ~90% to albumin - free drug rises dangerously in hypoalbuminemia
- Metabolism: CYP2C9 > CYP2C19; saturable (zero-order/Michaelis-Menten kinetics)
- Narrow therapeutic index: 10-20 mcg/mL (total); small dose increases → disproportionate level rise
- Half-life: 12-36 h (longer at high concentrations)
- Enzyme inducer: Reduces OCP, warfarin, and many other drug levels
Adverse Effects
| Dose-related (CNS) | Chronic use | Idiosyncratic |
|---|---|---|
| Nystagmus → ataxia → encephalopathy | Gingival hyperplasia | SJS/rash |
| Paradoxical seizures at toxic levels | Hirsutism, coarse facies | Hepatotoxicity |
| IV: arrhythmia, hypotension | Osteomalacia, megaloblastic anemia | Bone marrow suppression |
- Teratogenic - fetal hydantoin syndrome (craniofacial defects, cognitive impairment)
- Purple glove syndrome with IV extravasation - use fosphenytoin IV instead
Key Interactions
- Levels increased by: isoniazid, fluconazole, valproate, fluoxetine, metronidazole
- Phenytoin lowers: oral contraceptives, warfarin, lamotrigine, most other AEDs
One-liner
Phenytoin = Na⁺ channel blocker with saturation kinetics, narrow therapeutic window, extensive interactions, and significant chronic toxicity - largely replaced by newer agents but still relevant for status epilepticus.
This is a shared conversation. Sign in to Orris to start your own chat.