Ultrasonography vs Mammography in diagnosis of breast cancer
Reading File
Finding Sources
Searching PubMed
ultrasonography mammography breast cancer diagnosis comparison
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have enough high-quality content from multiple authoritative surgery and radiology textbooks to produce a comprehensive comparison. Let me compile this into a well-structured response.
Ultrasonography vs Mammography in Breast Cancer Diagnosis
Overview
Both mammography and breast ultrasound (ultrasonography) are first-line imaging investigations in women with breast symptoms. They are used together within the "triple assessment" framework — combining imaging, clinical examination, and needle biopsy — which is the gold standard for breast diagnosis.
"Mammography and ultrasound are the first-line imaging investigations in women with breast symptoms." — Grainger & Allison's Diagnostic Radiology
1. Mammography
Principle
Mammography uses low-energy X-rays (typically molybdenum/molybdenum target/filter combination, 17.5–19.6 keV) to image compressed breast tissue. Two standard views are taken: mediolateral oblique (MLO) and craniocaudal (CC).
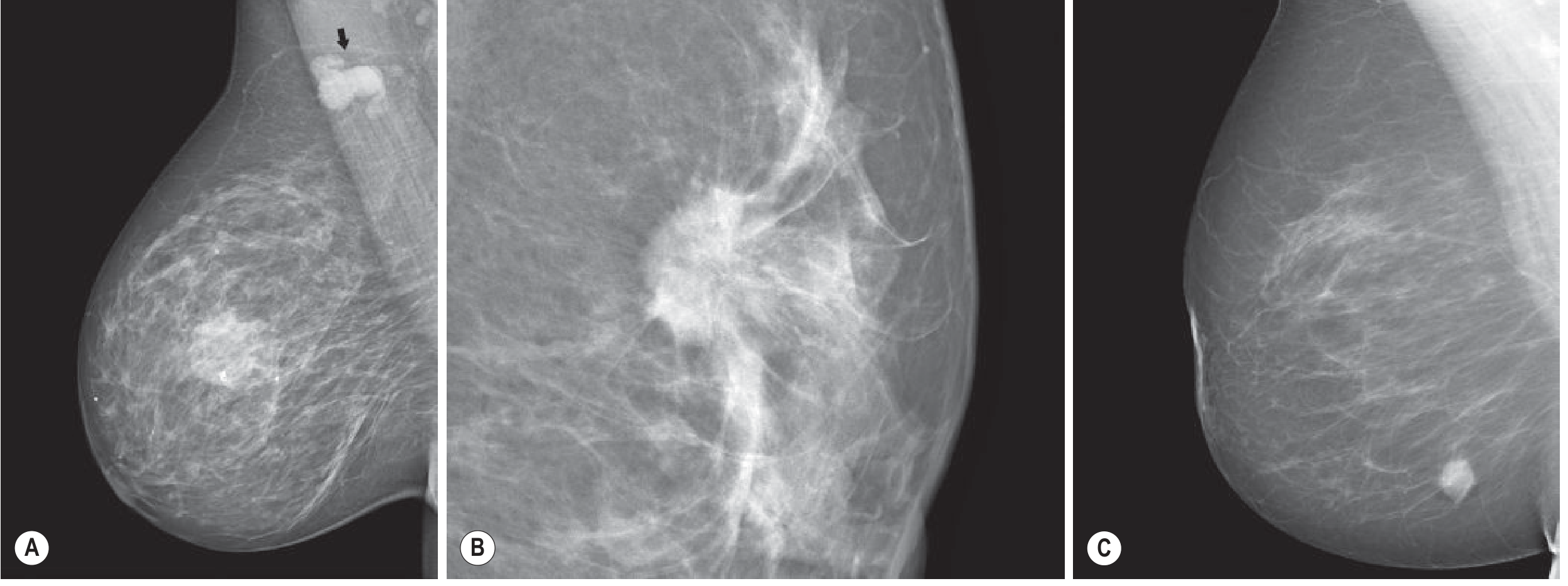
Key Radiological Findings Suggestive of Malignancy
| Finding | Features |
|---|---|
| Spiculated mass | ~90% associated with invasive cancer |
| Microcalcifications | 0.1–1 mm, clustered (≥4–5/cm³), linear branching pattern = highly suspicious |
| Architectural distortion | Disruption of normal breast tissue pattern |
| Asymmetric density | Without a corresponding mass |
BI-RADS Classification (ACR)
| Category | Definition | Malignancy Risk | Management |
|---|---|---|---|
| 0 | Incomplete | — | Additional imaging |
| 1 | Negative | 0% | Annual screening |
| 2 | Benign | 0% | Annual screening |
| 3 | Probably benign | <2% | 6-month follow-up |
| 4a/4b/4c | Suspicious | 2–95% | Biopsy |
| 5 | Highly suggestive | >95% | Biopsy |
| 6 | Known malignancy | — | As indicated |
Applies to mammography, ultrasound, and MRI.
Sensitivity & Limitations
- Sensitivity is significantly reduced by breast density — in dense breasts (BI-RADS C/D), sensitivity can fall below 50%
- 10–15% of clinically evident breast cancers are mammographically occult
- Dense breast tissue is also an independent risk factor for breast cancer (4–6× higher risk in extremely dense vs. fatty breasts)
- False positives occur — 75–80% of biopsied mammographic findings are benign
- Uses ionising radiation (~3 mGy per standard two-view exam); radiation risk is low and benefits far outweigh harms (~300:1 lives saved to induced cancers)
Strengths
- Gold standard for screening — primary modality for population-based breast cancer detection
- Excellent at detecting microcalcifications (down to ~100 µm)
- Detects non-palpable, asymptomatic cancers
- Reduces breast cancer mortality by detecting disease at earlier stage
2. Ultrasonography (Breast Ultrasound)
Principle
High-frequency sound waves are used to image breast tissue in real time, without ionising radiation. It is operator-dependent and primarily a diagnostic rather than screening tool.
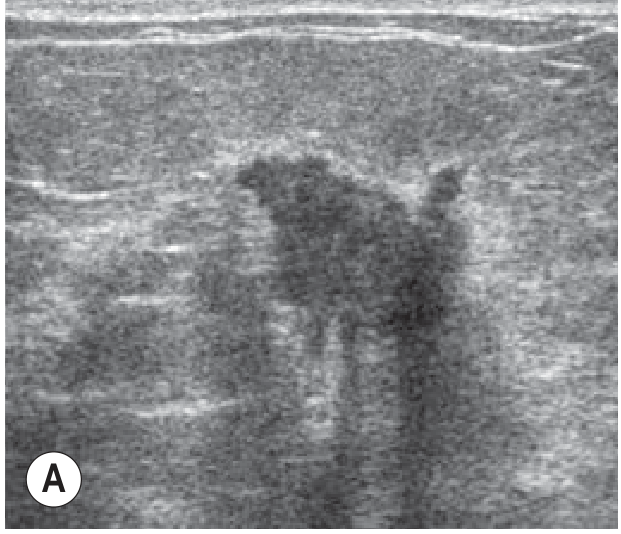
Key Ultrasonographic Features for Characterising Lesions
| Feature | Suspicious (Malignant) | Benign |
|---|---|---|
| Shape | Irregular | Oval/round |
| Margin | Ill-defined, microlobulated, spiculated | Circumscribed |
| Orientation | Taller than wide (not parallel) | Parallel to skin |
| Echogenicity | Hypoechoic | Hyperechoic/anechoic |
| Attenuation | Posterior shadowing | Posterior enhancement (cysts) |
| Vascularity (Doppler) | Irregular, centrally penetrating vessels | Vessels displaced peripherally |
| Elastography | Increased stiffness, area larger than grey-scale lesion | Normal stiffness |
Strengths
- Differentiates cystic from solid masses — critical for triaging benign cysts vs. solid lesions requiring biopsy
- Characterises palpable lesions not seen on mammography
- Better predictor of tumour size than mammography
- Can detect intraductal extension and multifocal disease not visible on mammogram
- Guides ultrasound-directed core needle biopsy
- Axillary lymph node staging — identifies abnormal nodes preoperatively; biopsy can confirm nodal involvement in ~40% of node-positive patients, enabling targeted axillary clearance
- No ionising radiation — safe in younger women and during pregnancy
- Useful in dense breasts where mammography sensitivity is reduced
Limitations
- Not recommended as sole screening tool — low reproducibility between operators, time-consuming, high false-positive rate
- Microcalcifications less reliably detected than with mammography
- Lobular carcinoma can be difficult to demonstrate — may show only subtle echotexture changes or appear normal
- No proven mortality reduction from ultrasound screening alone
3. Head-to-Head Comparison
| Parameter | Mammography | Ultrasonography |
|---|---|---|
| Primary role | Screening + diagnosis | Diagnosis + staging |
| Gold standard | Yes (screening) | No |
| Radiation | Yes (~3 mGy/exam) | No |
| Dense breasts | Sensitivity <50% | Better performance |
| Microcalcifications | Excellent | Poor |
| Cyst vs. solid | Cannot reliably differentiate | Definitive |
| Tumour size accuracy | Underestimates in dense tissue | More accurate |
| Axillary staging | Limited | Direct visualisation + biopsy |
| Operator dependence | Low | High |
| Guidance for biopsy | Stereotactic | Real-time ultrasound |
| Screening use | Routine from age 40 | Supplemental only |
| Lobular carcinoma | Better | Can be normal |
4. Combined Use and Clinical Scenarios
When ultrasound adds value to mammography:
- Dense breast tissue (BI-RADS C/D) — adds ~5 additional cancers detected per 1,000 exams when combined with mammography
- Palpable mass with no mammographic correlate
- Young women (pre-menopausal) with denser breasts
- Characterising a mass as cystic vs. solid
- Guiding percutaneous biopsy
When mammography is preferred:
- Microcalcification assessment (DCIS detection)
- Screening of asymptomatic average-risk women ≥40 years
- Post-treatment surveillance
The ACRIN 6666 trial found that adding ultrasound to mammography in high-risk women detected an additional 4.2 cancers per 1,000 women, but at the cost of >10% recall rate and increased biopsy rate — without demonstrated mortality reduction from US alone.
5. Advanced Techniques
Digital Breast Tomosynthesis (DBT / 3D Mammography)
Acquires multiple low-dose projections at different angles, producing thin slices through the breast. Addresses the main limitation of 2D mammography — tissue superimposition — improving both sensitivity and specificity, with mean glandular dose of ~2.3 mGy per view (only slightly higher than 2D). Increasingly replacing conventional 2D mammography.
Automated Whole-Breast Ultrasound (ABUS)
Overcomes operator variability of freehand US but not yet widely adopted.
Summary
Mammography is the established gold standard for breast cancer screening, particularly for detecting microcalcifications and non-palpable lesions. Its main weakness is reduced sensitivity in dense breast tissue. Ultrasound is the essential complementary tool — superior for characterising masses, staging the axilla, guiding biopsies, and imaging younger women with dense breasts. Neither modality replaces the other; optimal breast diagnosis integrates both within triple assessment, supplemented by MRI in high-risk patients.
Sources:
- Grainger & Allison's Diagnostic Radiology (Ch. 63 — Breast Imaging)
- Sabiston Textbook of Surgery, 21e (Ch. 68 — Diseases of the Breast)
- Mulholland & Greenfield's Surgery, 7e (Ch. 74 — Breast Disease)
- Current Surgical Therapy, 14e (Whole-Breast Ultrasound)
This is a shared conversation. Sign in to Orris to start your own chat.