CVS complete examination and history for MD medicine student in details with standard book
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from Harrison's 22nd edition and Goldman-Cecil Medicine. Let me compose the full, detailed CVS history and examination guide.
Cardiovascular System (CVS) - Complete History & Examination
For MD Medicine Students
Primary Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025); Goldman-Cecil Medicine, International Edition; Braunwald's Heart Disease; Fuster & Hurst's The Heart, 15th Ed.
PART I: CVS HISTORY TAKING
1. Introduction & Patient Identification
- Name, age, sex, occupation, domicile
- Referred by / presenting complaints (in patient's own words)
- Duration of each complaint
2. Chief Complaints - The "Cardinal Symptoms" of Heart Disease
The 7 cardinal symptoms of cardiac disease to ask about:
| Symptom | Key Cardiac Causes |
|---|---|
| Chest pain / discomfort | Angina, ACS, pericarditis, aortic dissection |
| Dyspnea | Heart failure (LV), pulmonary oedema, cardiac tamponade |
| Palpitations | Arrhythmias, AF, SVT, VT |
| Syncope / presyncope | AS, HOCM, complete heart block, VT |
| Oedema (leg / dependent) | RV failure, biventricular failure, constrictive pericarditis |
| Fatigue / easy fatigability | Low cardiac output, heart failure |
| Cough / haemoptysis | MS, LV failure (pulmonary oedema), PE |
3. History of Presenting Complaints (SOCRATES for each symptom)
A. CHEST PAIN
- Site: Central, retrosternal, left chest, epigastric
- Onset: Sudden vs. gradual; at rest vs. exertion
- Character:
- Squeezing/crushing/pressure-like = ischaemic (angina/ACS)
- Sharp, pleuritic, worse lying flat, relieved sitting forward = pericarditis
- Tearing/ripping, radiating to back = aortic dissection
- Burning, epigastric = GERD (differential)
- Radiation: To left arm, jaw, neck, back (aortic dissection)
- Associated symptoms: Sweating, nausea, vomiting, dyspnea, syncope
- Time: Duration (minutes = angina; >20 min = ACS; constant = pericarditis)
- Exacerbating/Relieving: Exertion, emotion, cold, heavy meals; relief with nitrates (angina), sitting forward (pericarditis)
- Severity: 1-10 scale
Grading of Angina - Canadian Cardiovascular Society (CCS):
| Class | Definition |
|---|---|
| I | Angina only with strenuous exertion |
| II | Slight limitation - angina on walking >2 blocks or climbing >1 flight |
| III | Marked limitation - angina on walking <2 blocks or climbing <1 flight |
| IV | Inability to do any activity without discomfort; angina at rest |
(Goldman-Cecil Medicine, Table 293, p. 391)
B. DYSPNEA
- Type: Exertional dyspnea (ED), orthopnea, paroxysmal nocturnal dyspnea (PND), dyspnea at rest
- NYHA Functional Classification for exertional dyspnea:
- Class I: No symptoms with ordinary activity
- Class II: Slight limitation; symptoms with moderate exertion
- Class III: Marked limitation; symptoms with minimal exertion, comfortable at rest
- Class IV: Symptoms at rest or with any activity
- Orthopnea: Number of pillows used (2-pillow, 3-pillow orthopnea); due to redistribution of fluid from legs to pulmonary circulation when lying flat
- PND: Awakens patient from sleep after 1-2 hours; relieved by sitting up or standing; caused by pulmonary oedema
- Cardiac vs. pulmonary dyspnea: Ask about wheeze, productive cough, history of smoking, occupational exposure
C. PALPITATIONS
- Character: Fast, slow, irregular, "fluttering," "thudding"
- Onset: Sudden/gradual, at rest/exertion
- Associated: Presyncope, chest pain, dyspnea
- Precipitating: Coffee, alcohol, thyroid disease, anxiety
- Duration and termination: Spontaneous, Valsalva manoeuvre
- Ask about: Prior ECG, ablation, medications
D. SYNCOPE
- Pre-syncope vs. true loss of consciousness
- Postural (orthostatic hypotension), exertional (AS, HOCM - high risk!), situational (micturition, cough, defaecation - vasovagal)
- Warning (prodrome): Lightheadedness, sweating = vasovagal vs. no warning = Stokes-Adams (complete heart block, VT)
- Recovery: Rapid = vasovagal; prolonged confusion = seizure
- Tongue bite, incontinence = suggest seizure
E. OEDEMA
- Location: Dependent (bilateral ankle/leg = cardiac), unilateral = DVT/venous insufficiency
- Duration, progression
- Worse at end of day, improved after recumbency (cardiac)
- Ask about ascites, facial puffiness (nephrotic syndrome differential)
- Associated: SOB, abdominal distension (ascites with RHF)
F. COUGH & HAEMOPTYSIS
- Dry nocturnal cough = LV failure, ACE inhibitor side effect
- Frothy pink sputum = acute pulmonary oedema
- Haemoptysis = mitral stenosis, PE, Eisenmenger syndrome
4. Past Medical History (PMH)
- Previous cardiac events: MI, heart failure, cardiac surgery, PCI/CABG, pacemaker/ICD
- Hypertension (duration, control, medications)
- Diabetes mellitus
- Hyperlipidaemia
- Rheumatic fever (important for valvular disease, especially MS)
- Congenital heart disease
- Stroke/TIA
- Peripheral vascular disease
- Renal disease
- Thyroid disease
- Previous ECG/Echo/angiogram findings
5. Drug History
- Current cardiac medications: antihypertensives, anticoagulants, antiplatelets, statins, diuretics, nitrates, digoxin, antiarrhythmics
- Cardiotoxic drugs: Doxorubicin, trastuzumab, clozapine
- Drugs causing QT prolongation: antipsychotics, macrolides, fluoroquinolones
- NSAIDs (worsen heart failure, increase BP)
- OCP (increases thrombotic risk)
- Over-the-counter/herbal medications
- Allergies: Drug name, type of reaction
6. Family History
- First-degree relatives with:
- Premature coronary artery disease (men <55 yrs, women <65 yrs)
- Sudden cardiac death (especially at young age - suggests HOCM, channelopathies: LQTS, Brugada)
- Hypertension, diabetes, hyperlipidaemia
- Cardiomyopathy (familial dilated, HOCM)
- Marfan syndrome, connective tissue disorders
- Congenital heart disease
7. Social History
- Smoking: Pack-years, current or ex-smoker, passive exposure
- Alcohol: Units per week (alcoholic cardiomyopathy, AF trigger, hypertension)
- Recreational drugs: Cocaine (coronary spasm, MI, dissection), amphetamines, anabolic steroids
- Diet: Saturated fat, salt intake
- Exercise: Level of physical activity (important for functional assessment)
- Occupation: Physical demands, occupational toxin exposure, stress
- Travel history: Endemic areas (Chagas disease, infective endocarditis risk)
- Socioeconomic: Affects access to care, medication compliance
8. Systems Review (relevant to CVS)
- Respiratory: Wheeze, chronic cough, sputum
- GI: Nausea, vomiting (inferior MI), abdominal pain (mesenteric ischaemia, hepatomegaly)
- Renal: Oliguria, haematuria (endocarditis), nocturia (HF)
- Neurological: TIA, stroke, visual disturbances (emboli)
- Musculoskeletal: Joint pains (rheumatic fever, reactive arthritis)
- Endocrine: Sweating, heat intolerance, weight change (thyroid), polyuria/polydipsia (diabetes)
PART II: CVS PHYSICAL EXAMINATION
STEP 1: GENERAL EXAMINATION (Begins before laying hands on the patient)
From Harrison's 22E, p. 1903: "The examination begins with an assessment of the general appearance of the patient, with notation of age, posture, demeanor, and overall health status."
A. General Appearance
- Comfortable at rest vs. in distress, breathless, diaphoretic
- State of nutrition: Cachectic (cardiac cachexia in advanced HF), obese (metabolic syndrome)
- Position: Sitting upright/leaning forward (pericarditis), unable to lie flat (orthopnea)
- Cheyne-Stokes respiration (advanced heart failure, low cardiac output)
- Pallor, cyanosis (central vs. peripheral), jaundice
B. Skin & Nails
- Central cyanosis: Tongue + mucous membranes; significant right-to-left shunt (congenital HD, Eisenmenger)
- Peripheral cyanosis (acrocyanosis): Fingers/toes only; low flow states - HF, shock, peripheral vascular disease
- Differential cyanosis: Lower limbs only (PDA + pulmonary hypertension, right-to-left shunt at great vessel level)
- Clubbing: Chronic cyanotic congenital HD (ToF, TGA), infective endocarditis, lung disease
- Splinter haemorrhages: Infective endocarditis (also trauma)
- Osler's nodes: Painful red nodules on finger pads - infective endocarditis
- Janeway lesions: Painless haemorrhagic macules on palms/soles - infective endocarditis
- Koilonychia: Spoon-shaped nails (iron deficiency, high output failure)
- Xanthelasma, xanthomas: Hyperlipidaemia; tendon xanthomas = familial hypercholesterolaemia
- Arcus cornealis (arcus senilis): <45 yrs suggests dyslipidaemia
- Malar flush: Mitral stenosis (MS facies), scleroderma
- Petechiae: Infective endocarditis
C. Facies
- Malar flush (MS)
- Exophthalmos + lid retraction: Hyperthyroidism
- Expressionless face + ptosis: Myotonic dystrophy (associated with AV block, arrhythmia)
- Down syndrome facies, Turner's syndrome, Marfan habitus
D. Skeletal/Dysmorphic Features
| Feature | Syndrome | Cardiac Association |
|---|---|---|
| Tall, high-arched palate, arachnodactyly, lens dislocation | Marfan syndrome | Aortic root dilatation, AR, MVP |
| Webbed neck, short stature, cubitus valgus | Turner syndrome | CoA, bicuspid AorticV, AS |
| Widely spaced eyes, low-set ears, mental retardation | Down syndrome | ASD, VSD, AVSD |
| Thumb/radial hypoplasia | Holt-Oram | ASD, VSD |
| Pterygium colli, hypertelorism | Noonan syndrome | Pulmonary stenosis, HCM |
STEP 2: VITAL SIGNS
A. Heart Rate
- Normal: 60-100 bpm
- Method: Radial pulse for 60 seconds
- Rate: Bradycardia (<60) or tachycardia (>100)
- Character and rhythm
B. Blood Pressure
- Measure both arms: >10 mmHg difference = subclavian artery stenosis, aortic dissection, or coarctation
- Measure both arms AND at least one leg when coarctation of aorta suspected (BP higher in arms than legs in CoA)
- Pulsus paradoxus: >10 mmHg fall in SBP during inspiration = cardiac tamponade, severe asthma, constrictive pericarditis
- Hypertensive urgency/emergency assessment
- Wide pulse pressure: Aortic regurgitation, hyperthyroidism, severe anaemia, AV fistula
- Narrow pulse pressure: Aortic stenosis, cardiac tamponade, constrictive pericarditis, severe LV dysfunction
C. Respiratory Rate
- Tachypnoea (>20/min): Heart failure, pulmonary oedema
D. Temperature
- Fever: Infective endocarditis, pericarditis, myocarditis, acute rheumatic fever
E. Peripheral O2 Saturation (SpO2)
- <94% warrants further investigation
STEP 3: THE HANDS, FACE, NECK (Peripheral Examination)
A. Hands
- Clubbing (grade I-IV)
- Splinter haemorrhages, Osler's nodes, Janeway lesions
- Peripheral cyanosis, capillary refill time
- Tremor (thyrotoxicosis)
- Temperature: Cold peripheries = low cardiac output
B. Eyes
(Goldman-Cecil, p. 392): "Examination of the fundi may show diabetic or hypertensive retinopathy or Roth spots typical of infectious endocarditis."
- Xanthelasma (hyperlipidaemia)
- Corneal arcus
- Kayser-Fleischer rings (Wilson's disease - cardiomyopathy)
- Roth spots (infective endocarditis)
- Retinal artery occlusion (embolism from LA thrombus or myxoma)
- Subconjunctival haemorrhage
- Exophthalmos (hyperthyroidism)
C. Mouth
- Dentition and oral hygiene (source of bacteraemia - endocarditis risk)
- High-arched palate (Marfan syndrome)
- Bifid uvula (Loeys-Dietz syndrome)
- Orange tonsils (Tangier disease)
- Telangiectasias on tongue/lips (Osler-Weber-Rendu syndrome - source of R-to-L shunt if pulmonary AVMs)
- Cyanotic tongue (central cyanosis)
STEP 4: CAROTID PULSE
- Method: Palpate one side at a time, gentle pressure, below the angle of the jaw
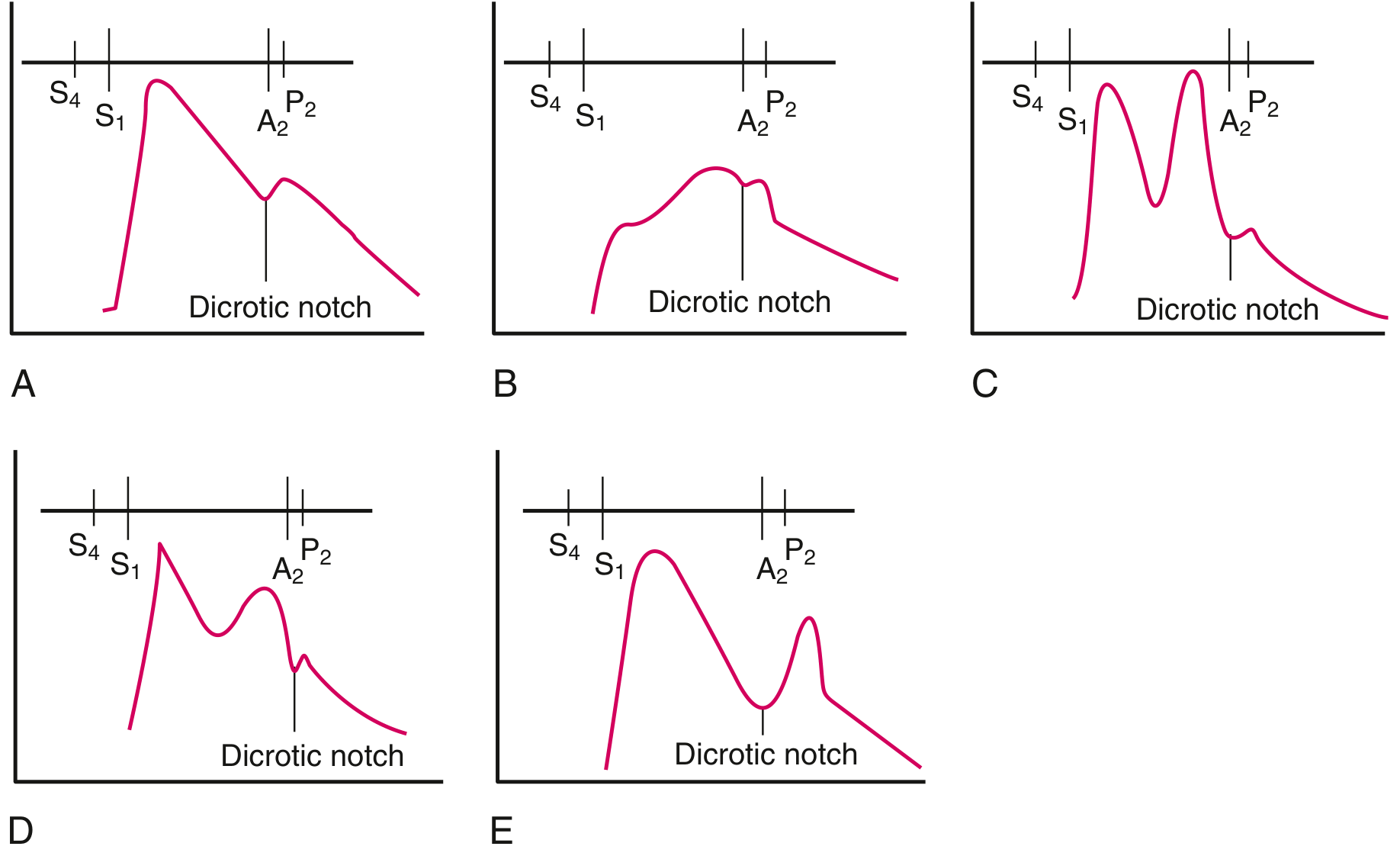
- Character of the carotid pulse:
| Pulse Character | Description | Clinical Association |
|---|---|---|
| Normal (normal) | Smooth, single systolic peak | Normal |
| Anacrotic (slow-rising, parvus et tardus) | Slow upstroke, delayed peak near S2 | Aortic stenosis (severe) |
| Bisferiens | Two systolic peaks (percussion + tidal wave) | Aortic regurgitation (significant), HOCM |
| Hyperkinetic (bounding, Corrigan's/water-hammer) | Rapid upstroke, collapsing quality | AR, hyperthyroidism, anaemia, AV fistula |
| Dicrotic | Accentuated dicrotic wave felt as double pulse | Severe HF, sepsis, cardiac tamponade |
| Pulsus alternans | Alternating strong and weak beats | Severe LV systolic dysfunction |
| Pulsus paradoxus | Marked decrease on inspiration | Tamponade, severe asthma |
STEP 5: JUGULAR VENOUS PRESSURE (JVP)
Harrison's 22E, p. 1904: "The JVP is the single most important bedside measurement from which to estimate the volume status."
A. How to Assess JVP
- Position patient at 30-45° (use 45° initially; adjust to visualise the meniscus)
- Turn head slightly to the left to examine the right internal jugular vein (preferred - directly in line with SVC and RA)
- Identify the venous pulsation just lateral to the sternocleidomastoid muscle
- Measure the vertical height of the venous pulsation above the sternal angle of Louis
- Normal = <4.5 cm above the sternal angle at 45°
- The sternal angle is approximately 5 cm above the mid-right atrium, so total CVP (cmH2O) = height above sternal angle + 5 cm
- If JVP is elevated, sit the patient fully upright with legs dangling to better assess the upper limit
- If not visible at 30-45°, check at 60° or even 90° (sitting)
IJV vs. EJV vs. Carotid distinctions:
| Feature | JVP (Venous) | Carotid (Arterial) |
|---|---|---|
| Pulsation character | Biphasic (2 peaks), soft, diffuse | Monophasic, forceful, discrete |
| Obliteration with pressure | Easily obliterated proximally | NOT obliterated |
| Posture effect | Falls with sitting up | No change |
| Inspiration effect | Falls (normal) | No change |
| Abdominojugular test | Rises | No change |
B. JVP Waveform Components
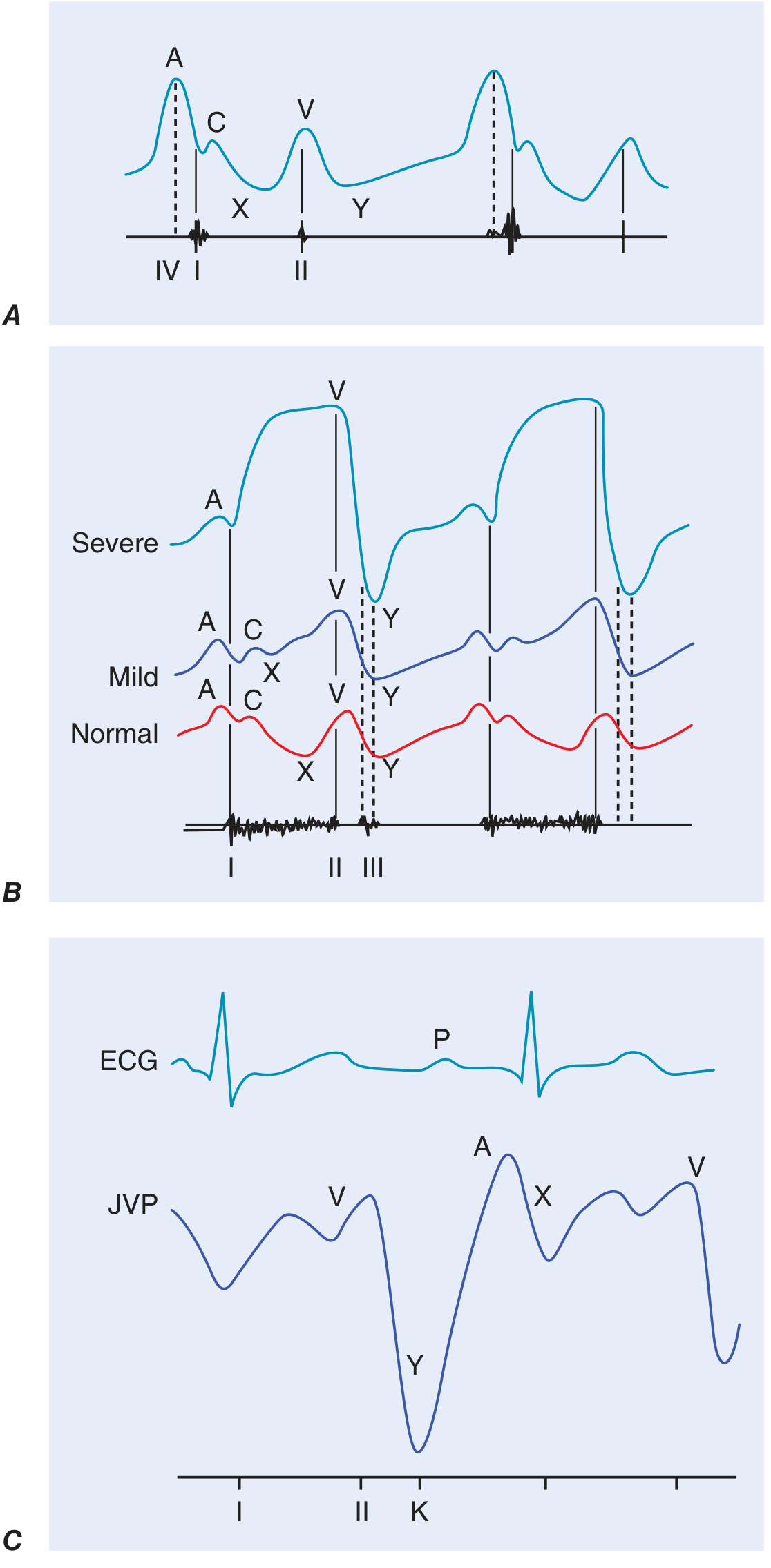
| Component | Mechanism | Timing relative to cardiac cycle |
|---|---|---|
| a wave | Right atrial presystolic contraction | Just after P wave on ECG, before S1 |
| c wave | Tricuspid valve pushed into RA during early RV systole / carotid artefact | Interrupts x descent |
| x descent | RA relaxation + downward displacement of TV | Systolic descent |
| v wave | Atrial filling against closed tricuspid valve (atrial diastole) | During ventricular systole, peaks near S2 |
| y descent | Tricuspid valve opening, ventricular filling begins | After peak of v wave |
C. Abnormalities of JVP Waveform
| Abnormality | Waveform Change | Clinical Cause |
|---|---|---|
| Elevated JVP | >4.5 cm above sternal angle | RHF, fluid overload, tamponade, constrictive pericarditis, SVC obstruction |
| Giant/cannon a waves | Exaggerated a wave | AV dissociation (VT vs. SVT), complete heart block, TR, RV failure |
| Absent a wave | No a wave | Atrial fibrillation |
| Large v waves | Prominent v wave, ventriculrised waveform | Tricuspid regurgitation (severe) |
| Blunted/absent y descent | Slow y descent | Tricuspid stenosis, cardiac tamponade |
| Prominent y descent | Sharp y descent | Constrictive pericarditis, severe RHF |
| Kussmaul's sign | JVP rises (or fails to fall) with inspiration | Constrictive pericarditis, RV infarct, restrictive cardiomyopathy, massive PE |
D. Abdominojugular Reflux (Hepatojugular Reflux)
- Apply firm pressure over right upper quadrant (upper abdomen) for >15 seconds
- Positive = sustained rise in JVP >3 cm
- Indicates elevated pulmonary capillary wedge pressure >15 mmHg
- Assess at 10 seconds (allow abdominal muscle tensing to subside)
- Caution patient not to Valsalva during test
STEP 6: PRECORDIAL EXAMINATION
Patient positioned: Supine at 45°, then left lateral decubitus for apex/low-frequency sounds
A. INSPECTION
- Chest shape: Barrel chest, pectus excavatum (compresses heart, can produce systolic murmur), pectus carinatum, kyphoscoliosis (cor pulmonale), asymmetry
- Scars:
- Midline sternotomy = CABG, valve surgery, congenital HD surgery
- Left submammary/lateral thoracotomy = mitral valvotomy (old closed commissurotomy), BT shunt
- Right infraclavicular scar = pacemaker/ICD implant
- Visible pulsations:
- Apex beat (visible in ~50% of normals)
- Visible left parasternal heave = RV hypertrophy
- Epigastric pulsation = aortic aneurysm, right ventricular enlargement
- Pulsatile neck veins (see JVP section)
- Dilated veins on chest wall: SVC obstruction, caval obstruction
B. PALPATION
Palpate in sequence: Apex beat → Left parasternal region → Aortic area → Pulmonary area → Epigastric area → Back (for aortic coarctation collateral pulsations)
1. Apex Beat
- Location: Normally in the 5th intercostal space, midclavicular line (MCL)
- Character:
Type Description Association Normal Tapping, localised, <2.5 cm Normal Heaving (sustained, forceful) Hyperdynamic, displaced, lifts finger LVH (pressure overload: AS, hypertension) Hyperdynamic (thrusting, volume-loaded) Vigorous, displaced laterally Volume overload: AR, MR, VSD Tapping Palpable S1, sharp Mitral stenosis (loud S1 palpable) Diffuse/dyskinetic Broad, unsustained, multiple areas LV aneurysm, dilated cardiomyopathy Double impulse Two distinct pulsations HOCM (systolic + atrial), LV aneurysm Absent Not palpable Obesity, emphysema, pericardial effusion, dextrocardia - Displacement: Lateral (LV dilatation/LVH), downward, mediastinal shift
2. Parasternal Heave (Right Ventricular Impulse)
- Place heel of hand over left parasternal area (2nd-4th ICS)
- Sustained heave lifting the hand = right ventricular hypertrophy/overload (pulmonary hypertension, pulmonary stenosis, severe MS, large ASD)
3. Thrills
- A palpable murmur (grade 4+ murmur): Systolic thrill = AS, VSD, PS; Diastolic thrill = MS (rare), AR
- Location as per murmur site
4. Palpable Heart Sounds
- Palpable S1 (tapping apex) = MS
- Palpable P2 in pulmonary area = pulmonary hypertension
5. Percussion
- Limited use in cardiac exam
- May help delineate cardiac borders
- Shifting of cardiac border to the right (dextrocardia - confirmed by apex beat)
- Dull left costophrenic angle (pleural effusion in heart failure)
C. AUSCULTATION
Stethoscope use:
- Diaphragm (high-frequency): S1, S2, AR, MR, pericardial rub, ejection clicks
- Bell (low-frequency, light pressure): S3, S4, MS (mitral diastolic murmur)
Auscultatory areas (listen over all 5 areas):
- Aortic area: 2nd right intercostal space, right sternal border (2RICS)
- Pulmonary area: 2nd left intercostal space, left sternal border (2LICS)
- Erb's point (left 3rd ICS): AR often best heard here in leaning-forward position
- Tricuspid area: Lower left sternal border (4-5th ICS, LLSB)
- Mitral area (Apex): 5th ICS, MCL - left lateral decubitus position for low-frequency sounds
Heart Sounds
S1 (First Heart Sound)
- Closure of mitral (M1) and tricuspid (T1) valves at onset of systole; M1 precedes T1
- Heard best at the apex
- Loud S1: MS (restricted leaflet excursion, mobile but not closing fully until high LA pressure), hyperdynamic states (fever, anaemia, thyrotoxicosis), short PR interval
- Soft S1: LV dysfunction, calcified/immobile MV, prolonged PR interval (1° AV block), MR
- Variable S1: AF, complete AV dissociation
S2 (Second Heart Sound)
- Closure of aortic (A2) and pulmonary (P2) valves; A2 precedes P2
- Heard best at base (2nd ICS)
- Splitting of S2:
Type Behaviour Cause Physiological splitting Widens on inspiration, closes on expiration Normal Wide splitting Wide but moves with respiration RBBB, pulmonary stenosis, ASD Fixed splitting Wide, does NOT change with respiration ASD (classic) Paradoxical (reversed) splitting Narrows on inspiration LBBB, severe AS, HOCM Absent P2 P2 not audible Severe PS, pulmonary atresia Loud P2 Accentuated, may be palpable Pulmonary hypertension Loud A2 Systemic hypertension
Added Heart Sounds (S3 and S4)
| Sound | Quality | Timing | Mechanism | Clinical Significance |
|---|---|---|---|---|
| S3 (Third HS) | Low-pitched "gallop" (Kentucky: lub-dub-TA) | Early diastole, after S2 | Rapid ventricular filling causing wall vibration | Pathological in adults >40: LV failure, volume overload (MR, AR, VSD); physiological in young/pregnancy |
| S4 (Fourth HS) | Low-pitched presystolic gallop (Tennessee: TA-lub-dub) | Late diastole, before S1 | Atrial kick into a stiff/hypertrophied ventricle | LVH (HTN, AS, HOCM), acute MI, restrictive cardiomyopathy; never normal |
Summation Gallop: S3 + S4 merge in tachycardia (sounds like a galloping horse)
Opening Snap (OS): Early diastolic high-pitched sound - mitral stenosis (mobile anterior leaflet). OS-S2 interval narrows as MS becomes more severe (closer to S2 = higher LA pressure = more severe MS)
Ejection Clicks: High-pitched early systolic sounds
- Aortic ejection click: 2RICS, does NOT vary with respiration - aortic stenosis, bicuspid aortic valve, aortic root dilatation
- Pulmonary ejection click: 2LICS, disappears on inspiration - pulmonary valve stenosis
Mid-systolic Click(s): Mitral valve prolapse (MVP); best at apex; moves earlier with standing/Valsalva (decreases preload)
Pericardial Friction Rub: Scratchy, to-and-fro sound (may have 3 components: atrial systole, ventricular systole, ventricular diastole); best heard with patient leaning forward, in full expiration; increases with pressure from diaphragm; pathognomonic of pericarditis
Heart Murmurs
Grading (Levine scale):
| Grade | Description |
|---|---|
| 1/6 | Barely audible, only with concentration in a quiet room |
| 2/6 | Faint but easily heard |
| 3/6 | Moderately loud, no thrill |
| 4/6 | Loud with palpable thrill |
| 5/6 | Very loud, audible with stethoscope edge only touching chest |
| 6/6 | Audible without stethoscope |
Systolic Murmurs:
| Murmur | Character | Location | Radiation | Key Features |
|---|---|---|---|---|
| Aortic Stenosis | Ejection (crescendo-decrescendo), harsh | 2RICS | To carotids | Soft A2, slow-rising pulse (parvus et tardus), sustained apex, S4, ejection click |
| Pulmonary Stenosis | Ejection, systolic | 2LICS | Left shoulder | Ejection click (disappears on inspiration), wide split S2, RV heave |
| HOCM | Ejection/mixed (obs + MR component) | LLSB to apex | Variable | Louder with Valsalva/standing; softer with squatting/leg raise; bisferiens pulse |
| Mitral Regurgitation | Holosystolic, plateau, blowing | Apex | Left axilla/back | Soft S1, S3, displaced apex, +/- signs of LV enlargement |
| Tricuspid Regurgitation | Holosystolic | LLSB | Increases with inspiration (Carvallo's sign), prominent v waves in JVP, pulsatile hepatomegaly | |
| VSD | Holosystolic, harsh | Mid-LLSB | Thrill at LLSB, louder with small defects ("maladie de Roger") | |
| MVP | Late systolic murmur | Apex | Axilla | Preceded by mid-systolic click; click and murmur move earlier with Valsalva/standing |
Diastolic Murmurs (always significant - always indicate structural disease):
| Murmur | Character | Location | Key Features |
|---|---|---|---|
| Aortic Regurgitation | Early diastolic, high-pitched, blowing | 3rd LICS (Erb's) | Heard leaning forward, full expiration; collapsing pulse; wide PP; Austin Flint murmur (diastolic rumble at apex) |
| Pulmonary Regurgitation | Early diastolic, high-pitched | 2-3rd LICS | Graham-Steell murmur: pulmonary hypertension |
| Mitral Stenosis | Mid-diastolic, low-pitched rumble | Apex (left lateral decubitus) | Opening snap + diastolic rumble with pre-systolic accentuation (if sinus rhythm); loud S1; tapping apex; RV heave; AF in advanced MS |
| Tricuspid Stenosis | Mid-diastolic | LLSB | Increases with inspiration; prominent a wave in JVP |
Continuous Murmurs: Heard throughout systole and diastole, peak around S2
- PDA: "Machinery murmur" - left infraclavicular area
- Ruptured sinus of Valsalva aneurysm
- AV fistula
- Coarctation of aorta (also intercostal/back)
Dynamic Auscultation - Response to Manoeuvres:
| Manoeuvre | Effect | HOCM | AS | MR | MVP |
|---|---|---|---|---|---|
| Valsalva (strain phase) | Decreases preload | LOUDER | Softer | Softer | Click earlier, louder |
| Standing quickly | Decreases preload | LOUDER | Softer | Softer | Click earlier |
| Squatting | Increases preload + afterload | SOFTER | Louder | Louder | Click later, softer |
| Passive leg raise | Increases preload | SOFTER | Louder | Louder | Click later |
| Hand grip (isometric) | Increases afterload | SOFTER | Softer | LOUDER | Softer |
| Amyl nitrite | Decreases afterload/preload | LOUDER | Louder | Softer | Click earlier |
STEP 7: LUNG EXAMINATION (Cardiovascular Assessment)
- Bibasal crepitations (fine): Pulmonary oedema / LV failure
- Wheeze: Cardiac asthma (bronchoconstriction from interstitial oedema)
- Dullness at lung bases: Pleural effusion (LV failure - typically bilateral; unilateral right > left)
- Reduced air entry: Pleural effusion
STEP 8: ABDOMINAL EXAMINATION
(Goldman-Cecil, p. 393): "The most common cause of hepatomegaly in patients with heart disease is hepatic engorgement from elevated right-sided pressures associated with right ventricular failure."
- Hepatomegaly: Tender, smooth liver edge = congestive hepatopathy (RHF)
- Pulsatile hepatomegaly: Tricuspid regurgitation (systolic expansion)
- Hepatojugular reflux: Press on RUQ; JVP rises = elevated PCWP, RHF
- Ascites: Congestive cardiac failure (right-sided), constrictive pericarditis
- Splenomegaly: Infective endocarditis (septic emboli), LV failure (portal hypertension)
- Aortic pulsation: Abdominal aortic aneurysm (pulsatile, expansile mass in midline)
- Arterial bruits: Renal artery bruits (renovascular hypertension), iliac bruit
STEP 9: PERIPHERAL VASCULAR EXAMINATION
- Peripheral pulses: Radial, brachial, carotid, femoral, popliteal, posterior tibial, dorsalis pedis - note presence, character, symmetry
- Radio-femoral delay: Coarctation of the aorta (femoral pulse delayed relative to radial)
- Radio-radial inequality: Subclavian artery stenosis, aortic dissection
- Absent peripheral pulses: PVD, embolism
- Ankle-Brachial Index (ABI): <0.9 = peripheral arterial disease
- Varicosities, venous insufficiency, DVT signs
- Peripheral oedema: Pitting/non-pitting; bilateral (cardiac, hypoalbuminaemic) vs. unilateral (DVT, lymphoedema)
- Note: Pitting oedema also caused by dihydropyridine calcium channel blockers
- Homans' sign (dorsiflexion calf pain) - neither sensitive nor specific for DVT
STEP 10: COMPLETING THE EXAMINATION
- Thank and cover the patient
- State: "To complete my examination I would also like to:
- Measure blood pressure in both arms (and legs if coarctation suspected)
- Perform fundoscopy (hypertensive/diabetic retinopathy, Roth spots)
- Check urine dipstick (haematuria in endocarditis, proteinuria in renal disease)
- Review 12-lead ECG, chest X-ray, echocardiogram
- Perform pulse oximetry
- Examine the back (kyphoscoliosis, sacral oedema in bedridden patients)
- Sacral oedema: Always check in bedridden/immobile patients"
PART III: SUMMARY TABLES
NYHA vs. CCS vs. Specific Activity Scale
| Class | NYHA | CCS Angina |
|---|---|---|
| I | No symptoms with ordinary activity | Angina only with strenuous exertion |
| II | Slight limitation; symptoms with moderate exertion | Angina walking >2 blocks or >1 flight of stairs |
| III | Marked limitation; symptoms with minimal exertion | Angina walking <2 blocks or <1 flight |
| IV | Symptoms at rest | Angina at rest |
(Goldman-Cecil Medicine, Table 29-3)
Signs That Indicate Specific Conditions
| Clinical Finding | Condition |
|---|---|
| Tapping apex + opening snap + mid-diastolic rumble | Mitral Stenosis |
| Displaced heaving apex + early diastolic murmur (Erb's) + collapsing pulse | Aortic Regurgitation |
| Slow-rising pulse + ejection systolic murmur (carotids) + S4 | Aortic Stenosis |
| Holosystolic murmur (apex, axilla) + S3 + displaced apex | Mitral Regurgitation |
| Murmur louder with Valsalva + bisferiens pulse + S4 | HOCM |
| Elevated JVP + pulsatile hepatomegaly + holosystolic murmur (LLSB, Carvallo's) | Tricuspid Regurgitation |
| Elevated JVP + Kussmaul's sign + rapid y descent + pericardial knock | Constrictive Pericarditis |
| Pulsus paradoxus + elevated JVP + muffled heart sounds + hypotension | Cardiac Tamponade (Beck's Triad) |
| Fever + new murmur + splinter haemorrhages + Osler's nodes | Infective Endocarditis |
Sources
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw Hill - Chapter 246: Physical Examination of the Cardiovascular System, pp. 1902-1909
- Goldman-Cecil Medicine, International Edition - Chapter 39: Physical Examination for Detection of Signs of Cardiovascular Disease, pp. 391-393
- Fuster and Hurst's The Heart, 15th Edition - Clinical Cardiovascular Examination
- Braunwald's Heart Disease, 2-Volume Set, A Textbook of Cardiovascular Medicine
Create a study guide PDF on CVS examination findings and their meanings
Reading File
Running Command
ls -la /home/daytona/workspace/ && mkdir -p /home/daytona/workspace/cvs-study-guide
This is a shared conversation. Sign in to Orris to start your own chat.