Hepatitis A and E management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatitis A" AND "hepatitis E" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Searching PubMed
"hepatitis E" AND ribavirin AND chronic
I now have comprehensive data from multiple authoritative sources. Here is the full structured answer:
Hepatitis A and Hepatitis E - Management
HEPATITIS A (HAV)
The Pathogen & Epidemiology
HAV is a non-enveloped, positive-sense RNA virus of the family Picornaviridae, genus Hepatovirus. It is a 27-nm icosahedral particle with a ~7.5 kb genome. Three human genotypes exist (I, II, III), with genotype I predominating globally. Transmission is via the fecal-oral route - through direct person-to-person contact or ingestion of fecally contaminated food or water.
High-risk groups:
- Travelers to developing countries
- Men who have sex with men
- Injection drug users
- Homeless persons
- Children in day-care centers (and their parents)
- Patients receiving clotting factor concentrates (hemophilia)
- Persons in institutional settings
Incubation period: 15-50 days (mean ~28-30 days)
Clinical Features
- Often mild and anicteric, especially in children
- Symptomatic icteric disease becomes more common with older age at infection
- Prodrome: fatigue, anorexia, nausea, right upper quadrant discomfort, fever
- Icteric phase: jaundice, dark urine, pale stools, pruritus
- Elevated ALT/AST (peaks early in acute phase), conjugated hyperbilirubinemia
- In 5-10% of cases, a secondary enzyme rise ("relapse") occurs
- Self-limited in nearly all cases - never progresses to chronic hepatitis
- Rare complication: fulminant hepatic failure (acute liver failure - ALF)
- Prolonged cholestatic course can occasionally occur
Serologic Course
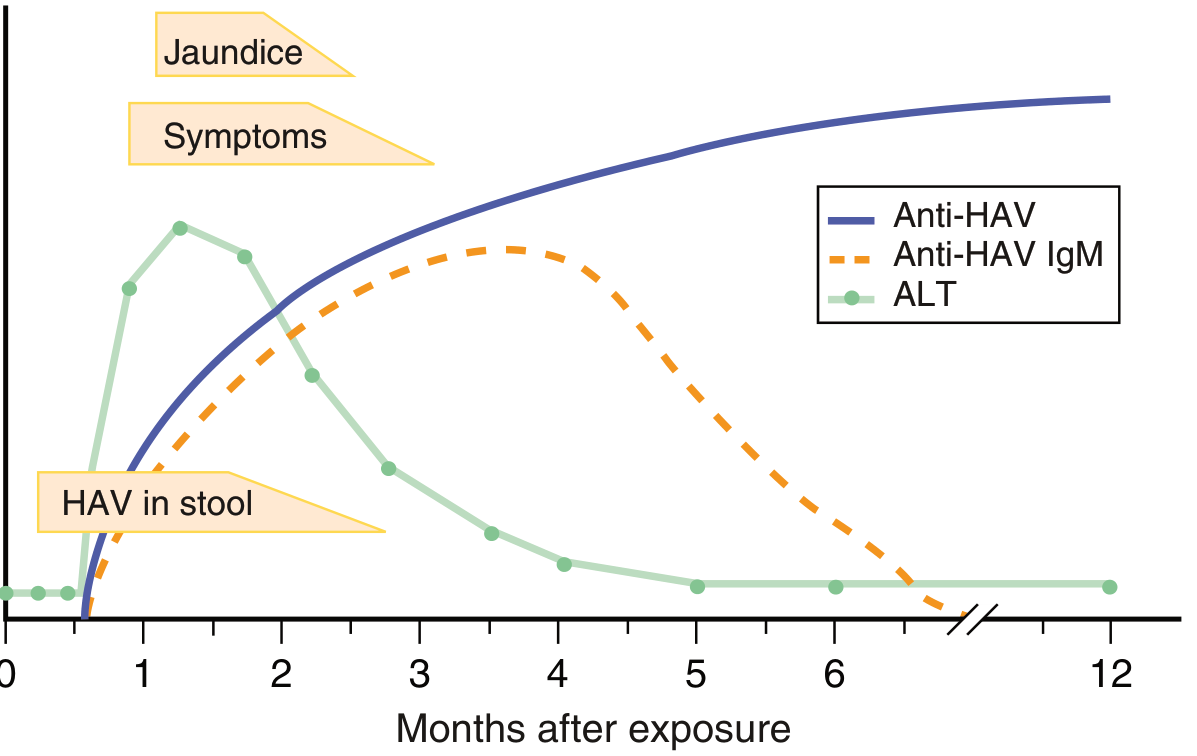
| Marker | Significance | Duration |
|---|---|---|
| HAV RNA (stool/serum) | Earliest marker; infectious period | 3-10 days before illness, ~1-2 weeks after onset |
| Anti-HAV IgM | Diagnostic of acute infection | Peaks ~2nd month; clears at 4-12 months |
| Anti-HAV IgG | Past exposure / immunity | Lifelong |
Diagnosis
- Anti-HAV IgM by enzyme immunoassay is the standard diagnostic test
- HAV RNA (PCR) can be detected in stool/body fluids but is not routinely required
- "Total anti-HAV" assays (IgM + IgG combined) indicate exposure/immunity but cannot distinguish acute from past infection
- Serology should only be ordered in symptomatic individuals to avoid false positives
Treatment
No specific antiviral therapy is required or available. Management is entirely supportive:
| Situation | Management |
|---|---|
| Uncomplicated acute HAV | Supportive care: rest, hydration, avoid hepatotoxic drugs/alcohol |
| Hospitalization indications | Factor V < 40%, any encephalopathy, persistent worsening jaundice, ascites, rapid liver shrinkage |
| Fulminant hepatic failure (ALF) | ICU care, management of cerebral edema; liver transplantation is the only definitive option |
- Prothrombin time prolongation and bilirubin/lactate levels are the key prognostic markers
- Serum aminotransferase levels and viral load do NOT carry prognostic value
- Prognosis is generally excellent; death is exceedingly rare, confined to fulminant cases
Prevention
Active immunization (HAV vaccine):
- Inactivated virus vaccine (purified from cell culture)
- Standard schedule: 2 doses, 6-18 months apart
- Accelerated schedule: Days 0, 7, and 21 (for last-minute travelers to endemic areas)
- Seroconversion: virtually 100% in healthy individuals; lower in immunocompromised
- Protective antibodies persist for at least 27 years after childhood/young adult vaccination
- A combination HAV + HBV vaccine is available
- Part of routine childhood immunization in many countries
Recommended vaccination groups:
- Non-immune travelers to endemic countries
- Healthcare workers
- MSM
- Close contacts of HAV cases
- Patients with chronic liver disease (CLD)
Passive immunization (Immunoglobulin - Ig):
- ~98% effective for post-exposure prophylaxis
- Used together with HAV vaccine in the post-exposure setting
- HAV vaccine preferred as it also prevents secondary cases
Post-exposure prophylaxis: Both HAV vaccine and Ig are ~98% effective; vaccination is preferred when no contraindications exist.
HEPATITIS E (HEV)
The Pathogen & Epidemiology
HEV is a non-enveloped, positive-sense RNA virus. 4 major genotypes with distinct epidemiological patterns:
| Genotype | Distribution | Features |
|---|---|---|
| GT1 | Developing countries (India, Asia, Africa) | Causes large waterborne community outbreaks; most common in India |
| GT2 | Mexico, West Africa | Community outbreaks |
| GT3 | Developed countries (Europe, USA) | Sporadic, zoonotic (pigs, boar, deer); no outbreaks; older patients with comorbidities |
| GT4 | China, Japan | Zoonotic; similar to GT3 |
- ~20 million infections and 3.3 million symptomatic cases per year worldwide
- ~44,000 deaths per year (2015 estimate)
- Over 60% of cases and deaths in East and South Asia
Routes of transmission:
- Fecal-oral (contaminated water) - primary route for GT1/2
- Zoonotic/foodborne (undercooked pork, boar, deer meat) - GT3/4
- Blood transfusion
- Vertical (mother to fetus)
Incubation period: 3-8 weeks (mean 40 days)
Clinical Features
Acute hepatitis E (GT1/2 - typical):
- Resembles acute hepatitis A clinically
- Prodrome: flu-like symptoms, fever, chills, abdominal pain, anorexia, nausea, vomiting, arthralgia, transient rash
- Icteric phase (1-7 days later): jaundice, dark urine, clay-colored stools, pruritus (lasting weeks)
- Labs: elevated ALT, AST, GGTP, conjugated hyperbilirubinemia, mild leukopenia, relative lymphocytosis
- Case-fatality rate: 0.5-4% in hospital-based data; 0.07-0.6% in population surveys
- Usually self-limited; may have a prolonged cholestatic variant with spontaneous resolution
Special populations:
| Group | Risk |
|---|---|
| Pregnant women (2nd-3rd trimester) | Mortality 5-25%; high rates of ALF (~22%), abortion, stillbirths, neonatal deaths |
| Immunosuppressed / organ transplant recipients | Risk of chronic HEV infection (GT3/4) |
| Chronic liver disease | More severe acute-on-chronic liver failure |
| GT3 patients | Older, more comorbidities; milder liver disease but neurologic manifestations more common |
Extrahepatic manifestations (mostly GT3):
- Neurological: Guillain-Barre syndrome, neuralgic amyotrophy, encephalitis
- Renal, hematologic, autoimmune manifestations
- Acute pancreatitis
Diagnosis
| Test | Indication | Notes |
|---|---|---|
| Anti-HEV IgM | Acute infection (primary diagnostic test) | Appears early, lasts 4-5 months; detectable in 80-100% during outbreaks |
| Anti-HEV IgG | Convalescent/past exposure | Appears days after IgM; persists years but may wane |
| HEV RNA (RT-PCR) | Confirmatory; chronic infection; immunosuppressed patients | Essential in endemic areas with low PPV for serology; required to diagnose and monitor chronic HEV |
| HEV antigen (EIA) | Early acute phase | Newer test; may detect virus longer than previously thought |
- In endemic areas: IgM anti-HEV is sufficient for clinical diagnosis
- In non-endemic areas (low pre-test probability): HEV RNA confirmation recommended
- Immunodeficient patients may lack antibody response - HEV RNA is essential
Treatment
Acute Hepatitis E
Supportive care only - no antiviral therapy has a proven role in acute HEV.
| Situation | Management |
|---|---|
| Uncomplicated acute HEV | Supportive care |
| Acute/acute-on-chronic liver failure | ICU admission, cerebral edema management, consider liver transplantation (LT) |
| Pregnant women with ALF | Supportive care; termination of pregnancy has NOT been shown to improve outcomes; treat postpartum hemorrhage with fresh frozen plasma (FFP) |
Chronic Hepatitis E (mainly in immunosuppressed GT3/4)
Chronic HEV (viremia > 3 months) occurs almost exclusively in immunosuppressed individuals (organ transplant recipients, HIV patients, hematologic malignancy patients on chemotherapy).
Step-wise approach:
- Step 1 - Reduce immunosuppression: Reduction or withdrawal of immunosuppressive drugs leads to spontaneous clearance of HEV in approximately one-third of transplant patients
- Step 2 - Ribavirin: If immunosuppression cannot be adequately reduced, or if reduction fails:
- Ribavirin ~600 mg/day for 3 months
- High rates of sustained virologic response (SVR) - defined as undetectable HEV RNA 3-6 months after treatment cessation
- No controlled RCTs available; evidence from retrospective case series
- Some patients show HEV genome mutations conferring ribavirin resistance at treatment failure
- Step 3 - Pegylated interferon-alpha (PEG-IFN-α): Used in select patients (e.g., those who fail ribavirin or in liver transplant recipients when ribavirin is not appropriate); evidence is limited to case reports/series
A 2025 review (PMID: 40693961) highlights the management of HEV in organ transplant recipients as an evolving area, reinforcing the ribavirin-first approach for chronic HEV post-transplant.
Prevention of Hepatitis E
| Measure | Details |
|---|---|
| Safe water/sanitation | Primary public health intervention for GT1/2 outbreaks |
| Food hygiene | Thoroughly cook pork, game meat; avoid raw/undercooked animal products (GT3/4) |
| HAV/water precautions for travelers | Standard food and water hygiene in endemic areas |
| HEV vaccine (HEV 239 / Hecolin) | Licensed in China only; 3-dose schedule; ~100% efficacy in trials; recommended for travelers, pregnant women, and those with CLD in endemic areas. Not yet licensed globally. |
| Blood product screening | Relevant in transplant/immunocompromised settings to prevent GT3 transfusion-transmitted HEV |
Key Comparison: HAV vs. HEV
| Feature | Hepatitis A | Hepatitis E |
|---|---|---|
| Virus family | Picornaviridae | Hepeviridae |
| Genome | +ssRNA | +ssRNA |
| Transmission | Fecal-oral (person-to-person, food, water) | Fecal-oral (water GT1/2); zoonotic (GT3/4) |
| Incubation | 15-50 days (avg. 25-30) | 3-8 weeks (avg. 40 days) |
| Chronicity | Never | Only in immunosuppressed (GT3/4) |
| Pregnancy risk | Mild | Severe - 5-25% mortality (GT1) |
| Fulminant hepatitis | Rare | Rare except in pregnancy |
| Specific treatment | None | Ribavirin (chronic only) |
| Vaccine | Yes - inactivated; globally available | Yes - China only (Hecolin) |
| Diagnosis | Anti-HAV IgM | Anti-HEV IgM / HEV RNA |
| Prognosis | Excellent; CFR <0.1% | Generally good; higher in pregnancy/immunosuppressed |
Sources: Goldman-Cecil Medicine, Sleisenger & Fordtran's GI and Liver Disease, Henry's Clinical Diagnosis and Management by Laboratory Methods, Park's Textbook of Preventive and Social Medicine, Creasy & Resnik's Maternal-Fetal Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.