Gauchers treatment
Reading File
Finding Sources
Searching PubMed
"Gaucher disease" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Gaucher's disease treatment:
Gaucher Disease - Treatment
Background
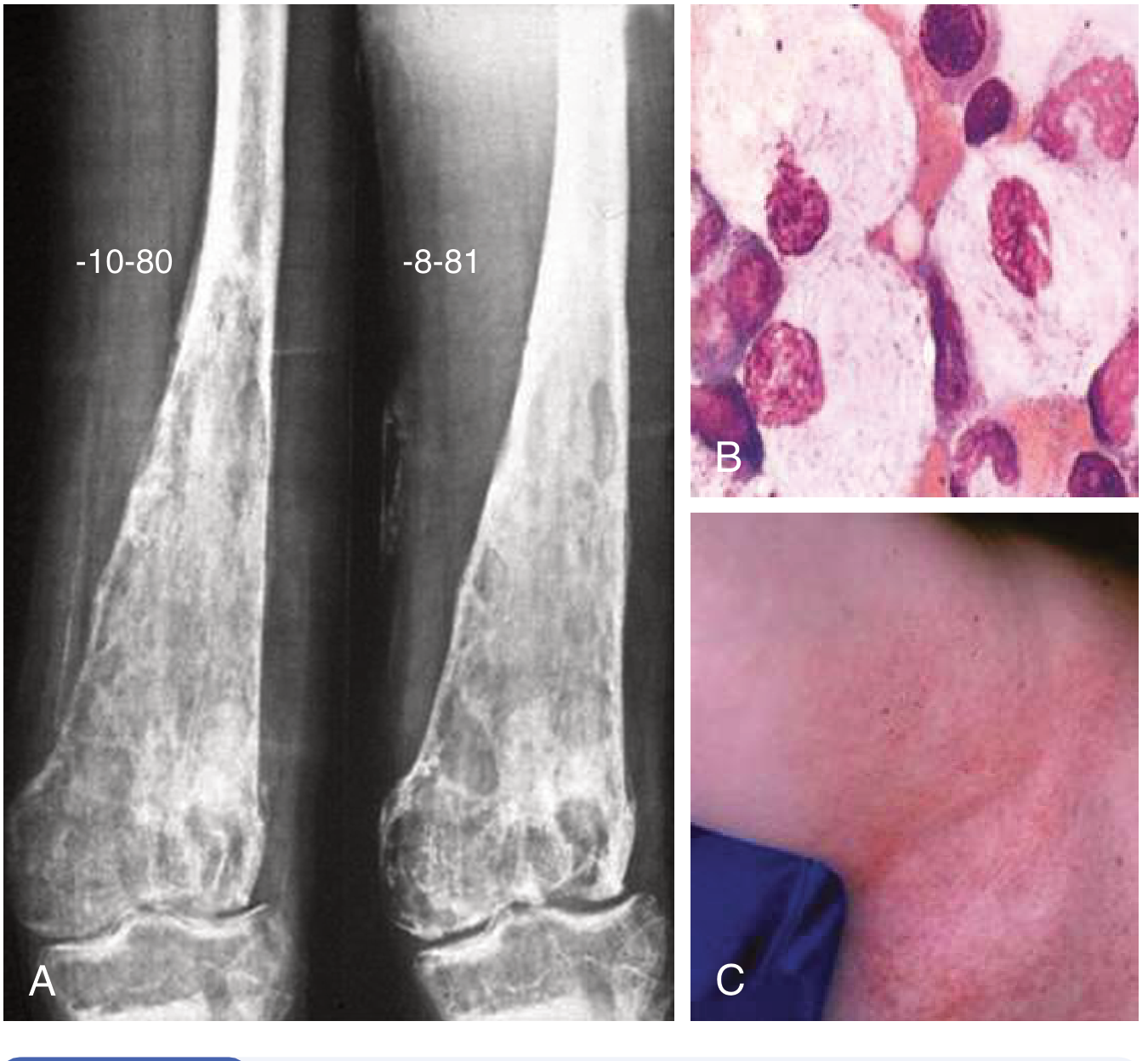
Gaucher disease is an autosomal recessive lysosomal storage disorder caused by deficiency of glucocerebrosidase (encoded by GBA1 on chromosome 1q21). Macrophages accumulate glucocerebroside, forming characteristic "Gaucher cells" with a wrinkled-paper appearance.
Three types:
- Type 1 - Non-neuronopathic (most common, especially in Ashkenazi Jews)
- Type 2 - Acute neuronopathic; rapidly fatal in early childhood
- Type 3 - Subacute neuronopathic; variable neurologic involvement
Asymptomatic and mildly symptomatic adults do not always require treatment.
1. Enzyme Replacement Therapy (ERT) - First-Line
ERT supplies the missing enzyme directly and is the mainstay for Types 1 and 3.
| Agent | Route | Notes |
|---|---|---|
| Imiglucerase (Cerezyme) | IV every 2 weeks | Most widely used; plant-derived recombinant |
| Velaglucerase alfa (VPRIV) | IV every 2 weeks | Human cell line-derived |
| Taliglucerase alfa (Elelyso) | IV every 2 weeks | Carrot cell-derived |
Dose: 15-60 IU/kg every other week, titrated to response.
Expected response (within 12-36 months):
- Reversal of anemia and thrombocytopenia
- Reduction in hepatosplenomegaly
- Improvement in bone disease
Limitation: ERT does NOT cross the blood-brain barrier - it does not halt neurologic progression in Types 2 or 3, though it can alleviate visceral manifestations. Treatment is ongoing, lifelong, and very expensive.
2. Substrate Reduction Therapy (SRT) - Oral Alternative
SRT reduces glucosylceramide synthesis to match its impaired rate of degradation.
| Agent | Mechanism | Notes |
|---|---|---|
| Eliglustat (Cerdelga) | Potent, specific inhibitor of glucosylceramide synthase (ceramide analogue) | Oral; adults with Type 1 only; CYP2D6 genotyping required before use; not for ultra-rapid metabolizers |
| Miglustat (Zavesca) | Inhibitor of glucosylceramide synthase | Oral; used when ERT is not an option; also used in Type 1; GI side effects common |
Eliglustat significantly improves spleen/liver volumes, hemoglobin, and platelet counts, and is increasingly used as an oral alternative to ERT in adults who prefer it. CYP2D6 status must be evaluated before prescribing - ultra-rapid CYP2D6 metabolizers are not eligible.
3. Supportive Therapies
| Problem | Management |
|---|---|
| Osteoporosis | Bisphosphonates |
| Bone fractures | Orthopedic surgery |
| Bone crises | Analgesics, hydration, palliation |
| Severe cytopenia/organomegaly (limited-resource settings) | Hematopoietic stem cell transplantation (improves systemic but NOT neurologic manifestations) |
| Splenectomy | Now rarely indicated |
4. Emerging and Investigational Therapies
- Brain-penetrant ERT - in development for neuronopathic forms
- Brain-penetrant SRT - targeting CNS involvement
- Chemical chaperones - pharmacological chaperone therapy (e.g., ambroxol at high doses is under investigation for Types 2 and 3 - a 2024 systematic review (PMID 39116528) examined this)
- Gene therapy - active area of research
5. Treatment by Type
| Type | Visceral Tx | CNS Tx |
|---|---|---|
| Type 1 | ERT or SRT (eliglustat/miglustat) | N/A (no CNS involvement) |
| Type 2 | ERT (visceral only) | No effective therapy; fatal in early childhood |
| Type 3 | ERT (visceral only) | ERT does not halt neurologic decline; supportive care |
Monitoring / Treatment Targets
Track response with:
- Hemoglobin level
- Platelet count
- Spleen and liver volumes (MRI)
- Skeletal imaging (MRI for avascular necrosis, bone marrow)
- Biomarker: lyso-Gb1 (glucosylsphingosine) - increasingly used as a disease activity marker
Note on GBA1 and Parkinsonism: Both Gaucher patients and heterozygous GBA1 carriers have a 5-10x increased risk of Parkinson disease/Lewy body disorders. Current therapies do not prevent this. This is the most common known genetic risk factor for parkinsonism. Monitoring for parkinsonian features is warranted.
- Goldman-Cecil Medicine, Chapter 192 (p. 2303-2304)
- Dermatology 5e, Chapter on Lysosomal Storage Disorders (p. 1248)
- Lippincott Illustrated Reviews: Biochemistry, 8th ed.
Neck of femur
Asking for Preferences
A detailed 10 marker for neck of femur fracture
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed information from Campbell's Operative Orthopaedics 2026 and Gray's Anatomy. I have everything needed for a thorough 10-marker answer.
Fracture of the Neck of Femur
1. Definition and Epidemiology
Fracture of the neck of femur (NOF) is a break through the intracapsular portion of the proximal femur, between the femoral head and the intertrochanteric line. It occurs predominantly in the elderly from low-energy falls and is an increasingly significant public health problem (estimated 458,000 to 1,037,000 hip fractures/year in the US by 2050). In young patients, it results from high-energy mechanisms (e.g., road traffic accidents) with frequent associated injuries. It is significantly more common in postmenopausal women due to osteoporosis.
2. Anatomy and Blood Supply (Why NOF is Clinically Unique)
The femoral neck is entirely intracapsular, which gives this fracture its distinct complications. Blood supply to the femoral head comes from three sources:
- Retinacular vessels (most important) - branches of the medial and lateral femoral circumflex arteries running deep to the synovium; the superior retinacular artery is the dominant supply
- Medullary vessels within the femoral neck (attenuated with age due to fatty marrow replacement)
- Artery of the ligamentum teres (the obturator artery branch; becomes progressively non-functional with age and atherosclerosis)
In elderly patients, the medullary and ligamentum teres supplies are effectively absent, leaving the retinacular vessels as the sole supply. A displaced NOF fracture tears these retinacular vessels, cutting off all blood to the femoral head - this is why avascular necrosis (AVN) is the hallmark complication.
"If the patient had an intertrochanteric fracture instead, the vessels of the retinacula fibers would not have been damaged and a different approach to surgical fixation could be undertaken without the need for a hemiarthroplasty." - Gray's Anatomy for Students
3. Classification
A. By Anatomical Location
- Subcapital - just below the femoral head (most common; highest AVN risk)
- Transcervical - through the mid-neck
- Basicervical - at the base of the neck near the trochanters (extracapsular in some; lowest AVN risk)
B. Garden Classification (Displacement-based; Most Widely Used)
| Grade | Description | Key Feature |
|---|---|---|
| Garden I | Incomplete/impacted (valgus) | Trabeculae angled upward |
| Garden II | Complete, non-displaced | Trabeculae aligned |
| Garden III | Complete, partially displaced | Trabeculae misaligned; neck/head still in contact |
| Garden IV | Complete, fully displaced | Trabeculae realigned with acetabulum; no neck-head contact |
- Garden I + II = non-displaced (lower AVN risk; ~15%)
- Garden III + IV = displaced (higher AVN risk; ~30-35%)
- Note: Garden I/II fractures with ≥20° sagittal plane (posterior) tilt should be managed as displaced fractures
C. Pauwels Classification (Biomechanical; based on fracture line angle with horizontal)
| Type | Angle | Predominant Force | Stability |
|---|---|---|---|
| Type I | <30° | Compression | Most stable |
| Type II | 30-50° | Compression + shear | Intermediate |
| Type III | >50° | Shear dominant | Most unstable; highest nonunion risk |
Increasing verticality = more shear at fracture site = higher fixation failure risk.
4. Clinical Features
- History: Fall in elderly; high-energy trauma in young
- Pain in the groin/hip radiating to the knee
- Shortened limb (psoas pulls femur proximally)
- Externally rotated limb (psoas action without femoral head fulcrum causes external rotation)
- Inability to bear weight
- Impacted (Garden I) fractures may allow limited weight bearing - do not miss these
Mechanism of external rotation: When the femoral neck is fractured, the psoas major (which inserts on the lesser trochanter and acts to externally rotate/flex the hip) loses its normal femoral head fulcrum - its overriding action pulls the femur proximally and into external rotation, exacerbated by adductor spasm.
5. Investigations
- X-ray AP pelvis + cross-table lateral - first-line; traction internal rotation view helps
- MRI - gold standard for occult fractures not visible on plain X-ray
- CT scan - shows degree of comminution; often available from trauma workup
- Pre-operative: FBC, renal function, ECG, coagulation, group and save
- Assess for coexisting medical comorbidities (elderly patients)
6. Treatment - Overview
"A satisfactory reduction is paramount in minimizing complications including nonunion and osteonecrosis." - Campbell's Operative Orthopaedics, 2026
The treatment decision is based on:
- Fracture displacement (Garden grade)
- Patient's physiological age (not just chronological)
- Ambulatory status and cognitive function
| Patient | Fracture | Treatment |
|---|---|---|
| Any | Asymptomatic (stress), no displacement | Conservative (protected weight bearing) |
| Young (<65) | Nondisplaced (Garden I/II) | Internal fixation (cannulated screws) |
| Young (<65) | Displaced (Garden III/IV) | Anatomic reduction + internal fixation |
| Elderly (>65) | Nondisplaced (Garden I/II) | Fixation or arthroplasty (moderate evidence) |
| Elderly (>65) | Displaced (Garden III/IV) | Arthroplasty (Strong AAOS recommendation) |
7. Internal Fixation Techniques
Used for non-displaced fractures and young patients with displaced fractures.
Cannulated screw fixation:
- Three partially threaded cannulated screws (6.5, 7.0, or 7.3 mm) in an inverted triangle configuration
- A 4th screw (diamond configuration) for significant posterior comminution
- Garden alignment index used to assess reduction: AP angle 160-180°; lateral deviation <20°
- Inferior screw placed along the calcar for rotational stability
Dynamic Hip Screw (DHS) / Screw-side plate device:
- Preferred for basicervical and high Pauwels angle (Type III) fractures
- Combines DHS with a derotational screw for unstable patterns
Femoral Neck System (FNS) / Fixed-angle plates:
- Newer devices for high Pauwels type III fractures
- Allow some controlled shortening while maintaining alignment
8. Arthroplasty
For displaced NOF fractures in elderly patients.
Hemiarthroplasty
- Femoral head is removed, neck trimmed, and a metal prosthesis is inserted into the medullary cavity
- The prosthesis head articulates with the native acetabulum
- Indication: displaced fracture, moderate activity level, pre-existing acetabular disease absent
Total Hip Arthroplasty (THA)
- Replaces both femoral head and acetabulum
- Preferred in physiologically active, cognitively intact patients with pre-existing hip arthritis
- AAOS guideline: THA beneficial over hemiarthroplasty in patients with pre-existing symptomatic hip osteoarthritis (Strong recommendation)
Unipolar vs. Bipolar Hemiarthroplasty
- Similar outcomes overall; bipolar may slightly lower revision rates (Moderate evidence)
9. Complications
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) | Most feared; 15-35% displaced, 14% nondisplaced; higher with Garden III/IV; the femoral head undergoes collapse |
| Nonunion | 9-16% in young patients; higher with Pauwels III; requires valgus osteotomy or conversion to arthroplasty |
| Failure of fixation | Due to inadequate reduction, poor implant position, or nonunion |
| Femoral neck shortening | Associated with pain and decreased mobility; abductor lever arm shortening |
| Deep vein thrombosis / PE | Major perioperative risk; thromboprophylaxis mandatory |
| Infection | Deep joint infection; especially after arthroplasty |
| Implant prominence/removal | 23-24% reoperation rate for prominent hardware in younger patients |
| Dislocation | After arthroplasty |
| Pressure sores, pneumonia, UTI | From prolonged immobility if surgery delayed |
In a meta-analysis of 18 studies in patients aged 15-50, the overall incidence of osteonecrosis was 23% and nonunion 9%. - Campbell's 2026
10. Prognosis and Special Considerations
- 1-year mortality after hip fracture in the elderly is approximately 25-30% - largely from cardiopulmonary and thromboembolic complications
- Early surgery (within 24-48 hours) reduces mortality and morbidity; however, medically optimizing the patient first is important
- Osteoporosis management post-fracture: bisphosphonates, calcium/Vitamin D supplementation, fall prevention
- Young patients with femoral neck fractures carry a higher surgical challenge - anatomic reduction is critical; AVN rate 23%, nonunion 9%
- Stress fractures of the femoral neck (e.g., in military recruits, athletes) require high suspicion; may be missed on plain X-ray; MRI essential
- Timing of capsular decompression (capsulotomy) is debated as a method to reduce AVN by relieving intracapsular tamponade; remains controversial
Sources: Campbell's Operative Orthopaedics, 15th Ed 2026; Gray's Anatomy for Students; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.