Paracetamol
Reading File
Finding Sources
Finding Sources
Searching PubMed
paracetamol acetaminophen pharmacology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Here is a full, well-organised summary of paracetamol from the textbooks.
Paracetamol (Acetaminophen)
Brand names: Tylenol, Ofirmev (IV formulation)
Class: Non-opioid analgesic / antipyretic
Metabolite of: Phenacetin
Mechanism of Action
Paracetamol works primarily within the CNS by inhibiting prostaglandin synthesis. Unlike NSAIDs, it has minimal peripheral anti-inflammatory activity. It also inhibits nitric oxide synthesis in murine spinal cord models. The CNS-central action accounts for its analgesic and antipyretic effects without the gastric or platelet-related side effects of NSAIDs.
Dosage
| Category | Adults | Children |
|---|---|---|
| Therapeutic dose | 500-1000 mg/dose (max 4 g/day) | 10-15 mg/kg/dose (max 60 mg/kg/day) |
| Toxic dose | ≥150 mg/kg (single ingestion) | ≥150-200 mg/kg |
| Lethal dose | >350 mg/kg | >250-350 mg/kg |
- The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 543
Pharmacokinetics
- Rapidly absorbed from the GI tract; peak plasma concentration in 30-60 minutes
- Plasma half-life ~2 hours under normal therapeutic conditions
Metabolism Pathway
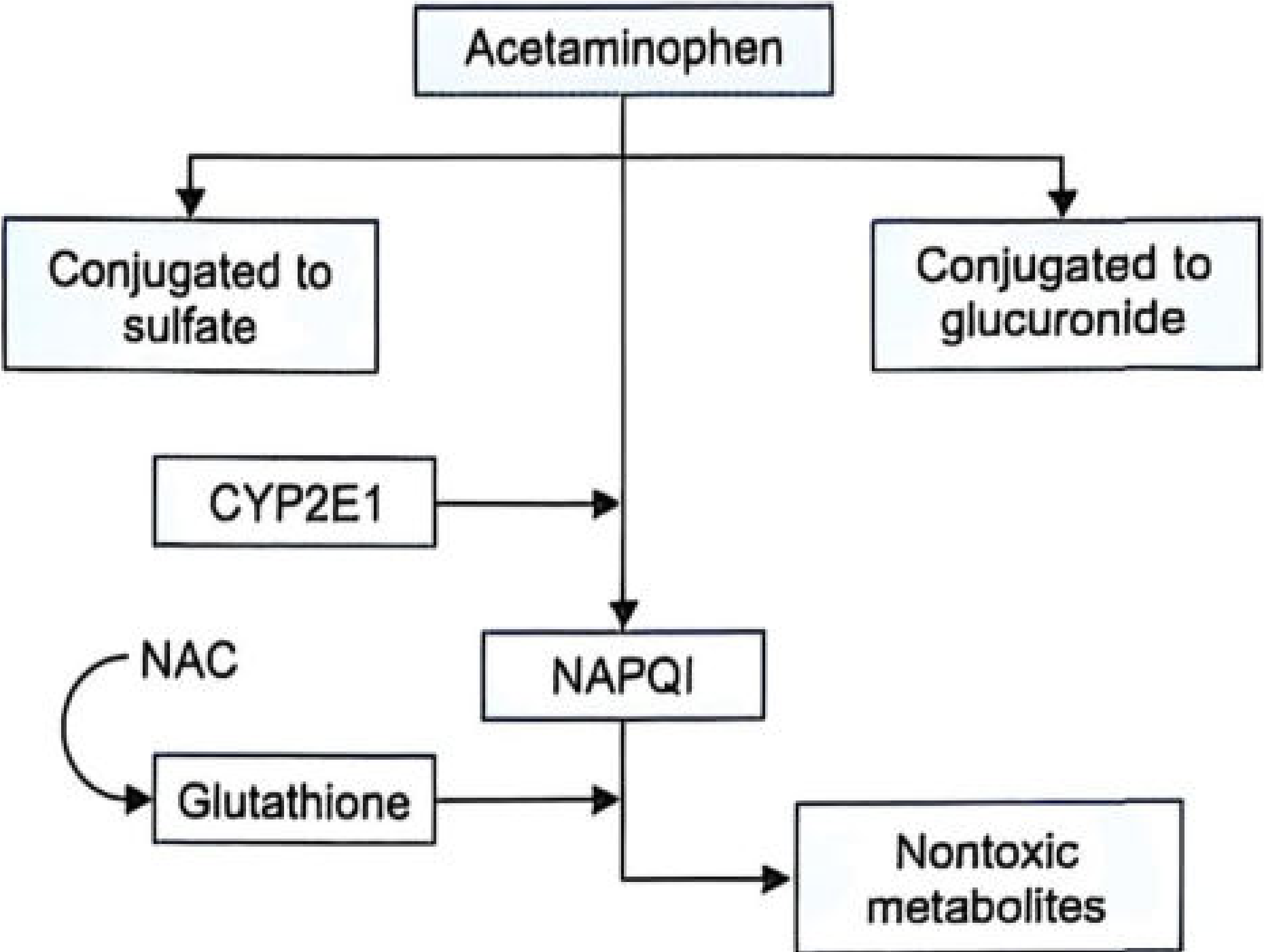
Fig. 31.1: Metabolism pathway of paracetamol - The Essentials of Forensic Medicine and Toxicology, 36th ed.
- ~90% - Conjugated with glucuronic acid and sulfuric acid → non-toxic metabolites (safe excretion)
- ~10% - Metabolized via CYP2E1 → NAPQI (N-acetyl-p-benzoquinone imine), a highly reactive toxic metabolite
Under normal conditions: NAPQI is neutralized by glutathione → cysteine and mercapturic acid conjugates (safely excreted)
In overdose: Hepatic glutathione reserves are exhausted → NAPQI accumulates → covalent binding to liver cell proteins, especially in the centrilobular region → oxidative stress and hepatocyte necrosis
Clinical Features of Paracetamol Poisoning
Stages
| Stage | Timeframe | Clinical Features |
|---|---|---|
| Stage I | 0-24 hours | Nausea, vomiting, anorexia, malaise, pallor, diaphoresis. Often asymptomatic; LFTs usually normal. Deceptively mild - can give false sense of security. |
| Stage II | 24-72 hours | Right upper quadrant pain, elevated LFTs (ALT, AST), bilirubin rises. Patient relatively pain-free despite ongoing liver damage. Anorexia, epigastric pain, malaise. |
| Stage III | 72-96 hours (peak hepatotoxicity) | Fulminant hepatic failure, coagulopathy, encephalopathy. Acute kidney injury, metabolic acidosis, hypoglycaemia, gastrointestinal haemorrhage, cerebral oedema, cardiomyopathy. |
| Stage IV | 4 days - 2 weeks | Recovery phase: if patient survives Stage III, complete resolution of liver injury typically occurs. |
Key point: In overdose, paracetamol does NOT affect acid-base balance, does NOT stimulate respiration, and does NOT have cardiovascular effects in the early stages - unlike aspirin poisoning.
Fatal dose: Ingestion of ~20 tablets of 500 mg (10 g) is usually fatal within 3-5 days.
Management of Paracetamol Overdose
-
Admission - All suspected overdose patients must be admitted, even if clinically well. A patient appearing well at 12 hours may die of acute hepatic failure up to 5 days later.
-
Gastric lavage - If admitted within 4 hours of ingestion.
-
Activated charcoal - Within 1-2 hours post-ingestion to limit absorption. Note: may reduce effectiveness of oral NAC if given together.
-
N-Acetylcysteine (NAC) - The antidote; most effective within 8-10 hours of overdose (effective up to 16-24 hours):
- Oral NAC: Loading dose 140 mg/kg, then 70 mg/kg every 4 hours. Duration 24-72 hours (6-18 doses). Dilute to ~5% solution.
- IV NAC (FDA-approved protocol): 150 mg/kg over 1 hour → 50 mg/kg over 4 hours → 100 mg/kg over 16 hours (21-hour regimen total). Recommended if vomiting prevents oral administration.
-
Methionine - Oral glutathione precursor: 2.5 g every 4 hours for 4 doses (10 g total over 12 hours). Useful if NAC unavailable.
-
Supportive care for hepatic necrosis complications: IV dextrose (hypoglycaemia), IV bicarbonate (metabolic acidosis), Vitamin K1, whole blood/plasma (coagulopathy). Fluid restriction to <2.5 L/day (paracetamol causes fluid retention).
-
Haemodialysis - For acute renal failure, or severe overdose with metabolic complications.
-
Liver transplantation - Indications: severe metabolic acidosis, prothrombin time >100 seconds, or serum creatinine >300 µmol/L (King's College Criteria).
Rumack-Matthew Nomogram - Essential tool for guiding treatment decisions based on serum paracetamol level and time since ingestion.
Postmortem Findings
- Remains of paracetamol tablets in stomach
- Centrilobular hepatic necrosis
- Acute tubular necrosis of kidneys
- Skin rashes, jaundice
- Petechial haemorrhages, GI bleeding
- Myocardial damage, cerebral oedema
Drug Interactions / Risk Factors for Increased Hepatotoxicity
- Isoniazid, rifampicin, barbiturates (enzyme inducers increase CYP2E1 activity → more NAPQI)
- Chronic alcohol use
- AIDS / immunocompromised states
- Long-term therapeutic use can cause toxic hepatitis in these high-risk groups
Medicolegal Notes
- Poisoning is usually accidental (overdosage, indiscriminate use as analgesic/antipyretic)
- More common in children
- Suicidal ingestion is notable because patients who attempt suicide with paracetamol often regret the choice due to the prolonged and painful course before death
- Common in USA and UK; relatively less common in India
Sources: The Essentials of Forensic Medicine and Toxicology 36th ed. (2026), p. 541-543 | Parikh's Textbook of Medical Jurisprudence Forensic Medicine and Toxicology, p. 714-715 | P C Dikshit Textbook of Forensic Medicine and Toxicology | Bailey and Love's Short Practice of Surgery 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.