Portal hypertension-Nelson
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Portal hypertension -Nelson
Reading File
Reading File
Finding Sources
Searching PubMed
"portal hypertension" AND "children"
Running Command
python3 -c " import pdfplumber pdf_path = '/home/daytona/workspace/attachments/…
Reading File
Running Command
python3 << 'EOF' from pypdf import PdfReader pdf_path = '/home/daytona/workspac…
Finding Sources
Running Command
python3 << 'EOF' from pypdf import PdfReader pdf_path = '/home/daytona/workspac…
Running Command
python3 << 'EOF' from pypdf import PdfReader pdf_path = '/home/daytona/workspac…
Searching Images
portal hypertension varices children pediatric esophageal splenomegaly
I now have the complete content of Chapter 415 from Nelson 2024. Here is a comprehensive, well-organized summary:
Portal Hypertension and Varices
Nelson Textbook of Pediatrics, 2024 — Chapter 415
(Amy G. Feldman & Frederick J. Suchy)
Definition
Portal hypertension is defined as elevation of portal pressure >10–12 mm Hg or a hepatic venous pressure gradient >4 mm Hg. It is a major cause of morbidity and mortality in children with liver disease, leading to varices, splenomegaly, ascites, and GI bleeding.
Etiology
Portal hypertension results from obstruction anywhere along the portal venous system — classified as prehepatic, intrahepatic, or posthepatic.
Table 415.1 — Causes of Portal Hypertension
| Category | Causes |
|---|---|
| Extrahepatic (Prehepatic) | Portal vein agenesis/atresia/stenosis; Portal vein thrombosis or cavernous transformation; Splenic vein thrombosis; AV fistula (↑ portal flow) |
| Intrahepatic — Hepatocellular | Cirrhosis (most common); Viral hepatitis; Congenital hepatic fibrosis; Wilson disease; α1-antitrypsin deficiency; Glycogen storage disease type IV; Methotrexate/PN hepatotoxicity |
| Intrahepatic — Biliary | Biliary atresia; Cystic fibrosis; Choledochal cyst; Sclerosing cholangitis; Bile duct paucity |
| Intrahepatic — Idiopathic | Idiopathic portal hypertension; Noncirrhotic portal fibrosis |
| Postsinusoidal (Posthepatic) | Budd-Chiari syndrome; Sinusoidal obstruction syndrome (venoocclusive disease) |
Key points:
- Portal vein thrombosis is the most common cause of extrahepatic portal hypertension. In neonates, causes include omphalitis, umbilical vein catheterization, dehydration, and sepsis. In older children: intraabdominal infection, IBD, celiac disease, PSC, and hypercoagulable states (Factor V Leiden, protein C/S deficiency).
- Cirrhosis is the most common cause of intrahepatic portal hypertension (biliary atresia, autoimmune hepatitis, Wilson disease, α1-AT deficiency, etc.).
- Budd-Chiari syndrome: obstruction of hepatic veins (efferent veins → IVC entry). Causes include inherited/acquired hypercoagulable states (antithrombin III deficiency, protein C/S deficiency, factor V Leiden, PNH, antiphospholipid syndrome), Behçet syndrome, IBD, sarcoidosis, IVC webs.
- Sinusoidal obstruction syndrome (venoocclusive disease): most common hepatic vein obstruction in children; classically post-BMT after total body irradiation ± cytotoxic drugs; also with azathioprine, 6-MP, thioguanine, pyrrolizidine alkaloids.
Pathophysiology
The primary hemodynamic abnormality is increased resistance to portal blood flow — whether intrahepatic (cirrhosis) or from portal vein obstruction.
Key mechanisms:
- Portosystemic collaterals develop but fail to fully decompress the portal system because portal flow increases simultaneously
- A hyperdynamic circulation develops: tachycardia, ↑ cardiac output, ↓ systemic vascular resistance, splanchnic vasodilation
- Hepatocellular dysfunction and portosystemic shunting → humoral vasodilators → ↑ plasma volume
- Collateral vessels preferentially form at junctions of absorptive and stratified epithelium (esophagus, anorectal region) → prone to rupture
- Congestive (portal hypertensive) gastropathy: abnormal submucosal AV communications in gastric wall → vascular ectasia → bleeding risk
Clinical Manifestations
| Feature | Details |
|---|---|
| GI Bleeding | Most common presentation (2/3 of children): hematemesis or melena from esophageal varix rupture. Less common: portal gastropathy, gastric antral ectasia, anorectal varices |
| Splenomegaly | Second most common finding; may be the first sign noticed on exam. Most asymptomatic. Beware: >50% of portal vein obstruction patients don't bleed until after age 6 |
| Ascites | Presenting sign in 7–21%; can develop with cirrhosis or new portal vein obstruction |
| Other | Growth impairment; minimal hepatic encephalopathy; impaired quality of life; portal hypertensive biliopathy (bile duct compression by cavernous transformation of portal vein) |
Risk of bleeding:
- Children with cirrhosis: 22% risk of first bleed; rises to 38% in those with known varices over 5 years
- Children with biliary atresia: 15–25% have bleeding on long-term follow-up
- NSAIDs and aspirin can precipitate hemorrhage (damage congested gastric mucosa, impair platelet function)
- Coughing during illness can also ↑ intravariceal pressure
Pulmonary Complications
- Hepatopulmonary syndrome (HPS): arterial oxygenation defect from intrapulmonary microvascular dilation (endothelin-1, NO). Occurs in ≥10% with portal HTN. Presents: dyspnea, cyanosis, clubbing, spider nevi.
- Portopulmonary hypertension (PP-HTN): PAP >25 mmHg at rest or LVEDP <15 mmHg. Presents with exertional dyspnea; histology shows pulmonary arteriopathy with laminar intimal fibrosis.
Diagnosis
| Investigation | Findings/Purpose |
|---|---|
| Doppler ultrasonography | First-line. Demonstrates portal vein patency, direction of flow. Hepatofugal flow (reversal) → associated with variceal bleeding. Detects esophageal varices, cavernous transformation |
| CT / MR angiography | Further anatomical definition; similar information to US but used less often |
| Selective arteriography | Precise mapping of extrahepatic vascular anatomy; useful before surgical decompression planning |
| Endoscopy | Most reliable for detecting esophageal varices and identifying bleeding source. Red spots on varices = strong predictor of imminent hemorrhage. Note: up to 1/3 of bleeding children have a non-variceal source (portal gastropathy, GU ulcers) |
| Bubble echocardiography | For HPS: delayed left-heart appearance of microbubbles after peripheral saline injection demonstrates intrapulmonary shunting |
| Best noninvasive predictors | Platelet count + spleen length (ultrasound) + serum albumin |
Treatment
Acute Variceal Hemorrhage
Stabilization first:
- IV crystalloid resuscitation → RBC replacement
- Target Hb 7–9 g/dL (avoid over-transfusion — raises portal pressure)
- Correct coagulopathy: Vitamin K, platelets, FFP as needed
- Nasogastric tube (confirm blood, monitor bleeding)
- IV H2 blocker or PPI (reduce gastric erosion risk)
- IV antibiotics (high risk of infectious complications)
Pharmacologic reduction of portal pressure:
| Drug | Dose | Notes |
|---|---|---|
| Vasopressin | 0.33 units/kg bolus over 20 min → 0.33 units/kg/hr or 0.2 units/1.73 m²/min continuous | ↑ splanchnic vascular tone → ↓ portal flow. Side effects: vasoconstriction → impaired cardiac, bowel, renal perfusion; fluid retention |
| Octreotide (preferred) | 1 μg/kg bolus → 1.0–5.0 μg/kg/hr continuous IV | Somatostatin analog; ↓ splanchnic flow with fewer side effects |
15% of children with portal hypertensive bleed will have persistent hemorrhage despite splanchnic vasoconstriction.
Endoscopic therapy (after pharmacologic failure or after stabilization):
- Variceal band ligation — preferred (more effective, fewer side effects than sclerotherapy in adults)
- Sclerotherapy — for smaller children where banding device cannot be used; intra- or paravariceal injection. Complications: bleeding, bacteremia, esophageal ulceration, stricture
- After ligation or sclerosis → repeat endoscopy until varices obliterated
If bleeding persists despite above:
- Sengstaken-Blakemore tube — mechanical compression of esophageal and gastric varices. Rarely used; high complication rate; high rebleed rate on removal; risk of aspiration. Requires sedation/intubation in children. Bridge to definitive procedure only.
Surgical Options
| Procedure | Details |
|---|---|
| Portacaval shunt | Diverts nearly all portal flow to IVC. Significant encephalopathy risk in parenchymal disease |
| Mesocaval / Distal splenorenal shunt | More selective; allows greater hepatopetal flow. Technically challenging in infants (shunt thrombosis risk) |
| Meso-Rex shunt | Superior mesenteric vein → left portal vein bypass. Restores physiologic portal flow. 84% success rate for idiopathic extrahepatic portal vein thrombosis. Improves growth and cognitive function |
| TIPS | Stent between right hepatic vein and right/left portal vein branch. Useful as bridge to transplant. Risks: hepatic encephalopathy, thrombosis |
| Liver transplantation | Definitive therapy for intrahepatic disease/cirrhosis and for HPS. Prior shunt surgery does not preclude transplant (but makes it technically harder) |
Prophylaxis
- β-blockers (propranolol): used extensively in adults — lower cardiac output, induce splanchnic vasoconstriction. Adults: reduces variceal hemorrhage and improves survival. Effect considered when pulse rate reduced by ≥25%. Limited data in children.
- Primary and secondary prevention of variceal bleeding: endoscopic band ligation program after obliteration.
Prognosis
- Portal hypertension from intrahepatic disease has a poor prognosis — usually progressive with deteriorating liver function.
- Focus: prompt treatment of acute bleeding + prevention of recurrence.
- Patients with progressive liver disease + significant varices → ultimately require orthotopic liver transplantation.
- Liver transplantation is the only effective therapy for HPS.
- Also indicated for hepatic vein obstruction and severe venoocclusive disease.
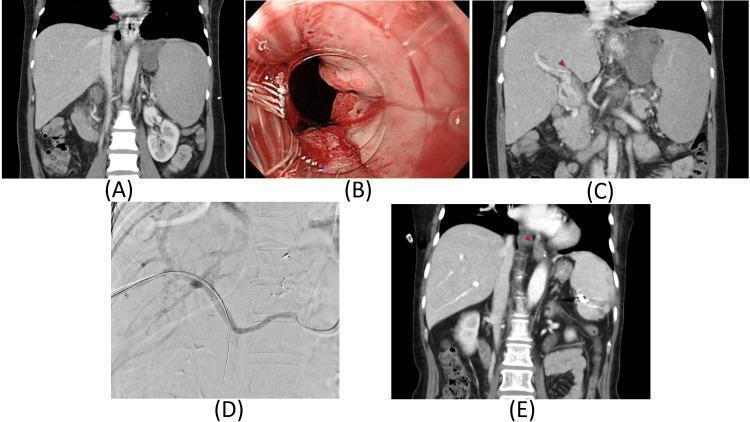
Composite illustrating portal hypertension: (A) CT showing splenomegaly and esophageal varices, (B) endoscopic view of esophageal varices with white nipple sign indicating recent hemorrhage, (C) CT showing portal vein thrombosis (filling defect), (D) fluoroscopic image of portal vein stenting, (E) follow-up CT showing variceal resolution after stenting.
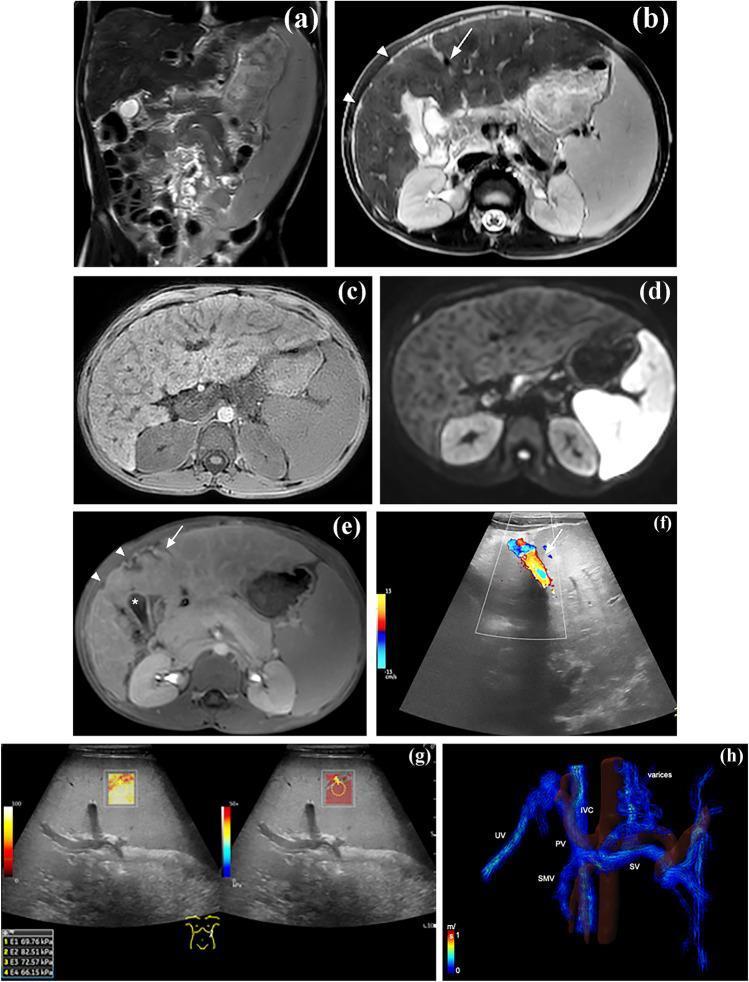
MRI and Doppler ultrasound in a pediatric patient with congenital hepatic fibrosis showing massive splenomegaly, hepatic morphological changes, recanalized umbilical vein, increased spleen stiffness on shear-wave elastography, and portosystemic communications on 4D-flow MRI.
Source: Nelson Textbook of Pediatrics, 2024, Chapter 415 (Part XVI: The Digestive System), pp. 2505–2506
This is a shared conversation. Sign in to Orris to start your own chat.