Pelvis obgy clinical posting
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is your complete clinical posting guide on Anatomy of the Female Pelvis - structured for MBBS clinical year.
Anatomy of the Female Pelvis - OB/GY Clinical Posting
1. Bony Pelvis
The pelvis is divided into the true pelvis (below the pelvic brim) and false pelvis (above it). The dividing line - the linea terminalis (pelvic brim) - runs from the sacral promontory posteriorly to the superior edge of the pubic symphysis anteriorly.
Bones
The true pelvis is formed by 4 bones:
- 2 innominate (hip) bones - each made up of ilium, ischium, and pubis
- Sacrum
- Coccyx
Female vs. Male Pelvis - Key Differences
| Feature | Female | Male |
|---|---|---|
| Inlet shape | Oval/round (gynecoid) | Heart-shaped |
| Inlet width | Wider | Narrower |
| Subpubic angle | Obtuse (>90°) | Acute (<90°) |
| Sacrum | Shorter, wider, less pronounced promontory | Longer, narrower |
| Pelvic walls | Wider apart | Closer |
The female inlet is oval and wider, facilitating childbirth, but this contributes to relative pelvic floor weakness. - Campbell-Walsh-Wein Urology, p. 3215
2. Pelvic Inlet & Outlet Diameters (Obstetric Importance)
These are high-yield for your OB/GY posting:
| Diameter | Measurement | Clinical Note |
|---|---|---|
| Diagonal conjugate | 12.5-13 cm | Measured clinically per vaginum (sacral promontory to lower border of pubic symphysis) |
| True/obstetric conjugate | ~11 cm | Diagonal conjugate minus 1.5-2 cm; smallest AP diameter of inlet |
| Transverse diameter of inlet | 13 cm | Greatest distance between lineae terminales |
| Interspinous diameter | 11 cm | Distance between ischial spines; narrowest diameter of the outlet |
| Oblique diameter | 12 cm | Sacroiliac joint to opposite iliopectineal eminence |
| AP diameter of outlet | 9 (+2) cm | Lower border of symphysis to tip of coccyx |
General Anatomy and Musculoskeletal System (THIEME Atlas), p. 162
The ischial spine is a crucial clinical landmark - it is used for pudendal nerve block and as the reference point for pelvic organ prolapse staging (station 0 = level of ischial spines).
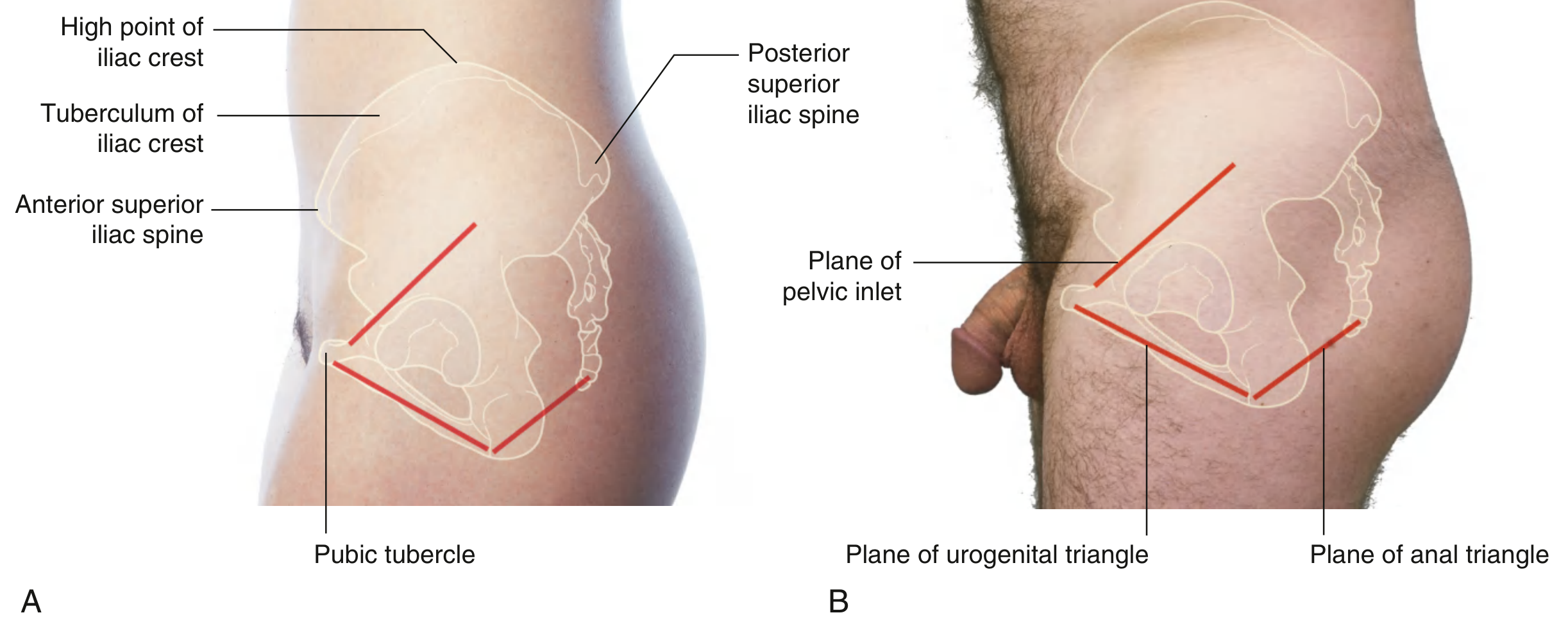
3. Surface Anatomy & Clinical Landmarks
In the anatomical position: the anterior superior iliac spine (ASIS) and the anterior superior edge of the pubic symphysis lie in the same vertical plane. The pelvic inlet faces anterosuperiorly.
Palpable landmarks (use in physical exam):
- Iliac crest - from ASIS to posterior superior iliac spine (PSIS)
- Pubic symphysis - palpable in midline deep to mons pubis in women
- Ischial tuberosities - lateral corners of the diamond-shaped perineum (palpable at the gluteal fold)
- Coccyx tip - palpable in midline, posteriorly, defines the posterior limit of the perineum
- Ischial spine - felt during vaginal examination; landmark for pudendal block and prolapse staging
Perineum
The diamond-shaped perineum is divided by a line between the ischial tuberosities into:
- Urogenital triangle (anterior) - almost horizontal, faces inferiorly
- Anal triangle (posterior) - more vertical, faces posteriorly
4. Pelvic Floor
The pelvic floor is formed by:
- Pelvic diaphragm (levator ani + coccygeus) - the major component
- Perineal membrane (anteriorly)
- Muscles of the deep perineal pouch (anteriorly)
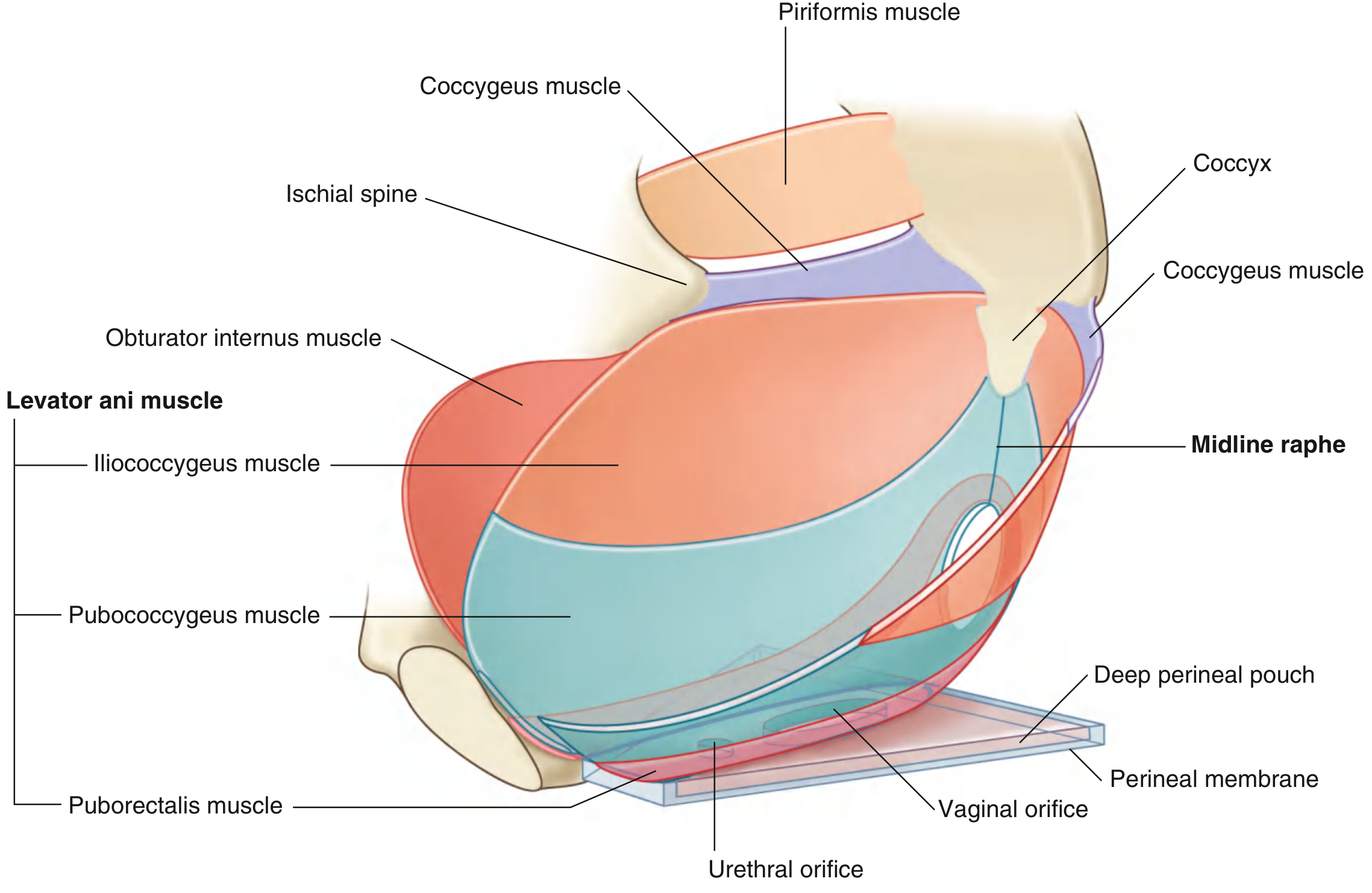
Levator Ani - THE most important pelvic floor muscle
The levator ani is a broad, thin muscle with 3 named parts:
| Part | Origin | Insertion | Key Function |
|---|---|---|---|
| Puborectalis | Posterior aspect of pubic body | Forms U-shaped sling around anorectal junction | Maintains anorectal angle; continence |
| Pubococcygeus | Posterior pubis + tendinous arch | Anococcygeal raphe + visceral organs | Sling around vagina and urethra (pubovaginal muscle) |
| Iliococcygeus | Ischial spine + posterior obturator fossa | Coccyx + anococcygeal raphe | Lateral component of pelvic floor |
Innervation: Levator ani nerve from S3, S4, S5 (traveling medial to the ischial spine) + branches from pudendal nerve (S2-S4).
Coccygeus: Arises from ischial spine and sacrospinous ligament, inserts on sacrum/coccyx. Completes the posterior pelvic diaphragm.
Levator hiatus: The U-shaped defect anteriorly in the levator ani, through which the urethra, vagina, and rectum pass.
Levator plate: Formed by fusion of levator ani muscles in the midline. Serves as a horizontal shelf for pelvic viscera. Weakening leads to sagging and pelvic organ prolapse.
Sustained resting tone of the pelvic floor supports viscera, resists intra-abdominal pressure, and maintains urinary/fecal continence. - Campbell-Walsh-Wein, p. 3215
5. Pelvic Cavity & Viscera
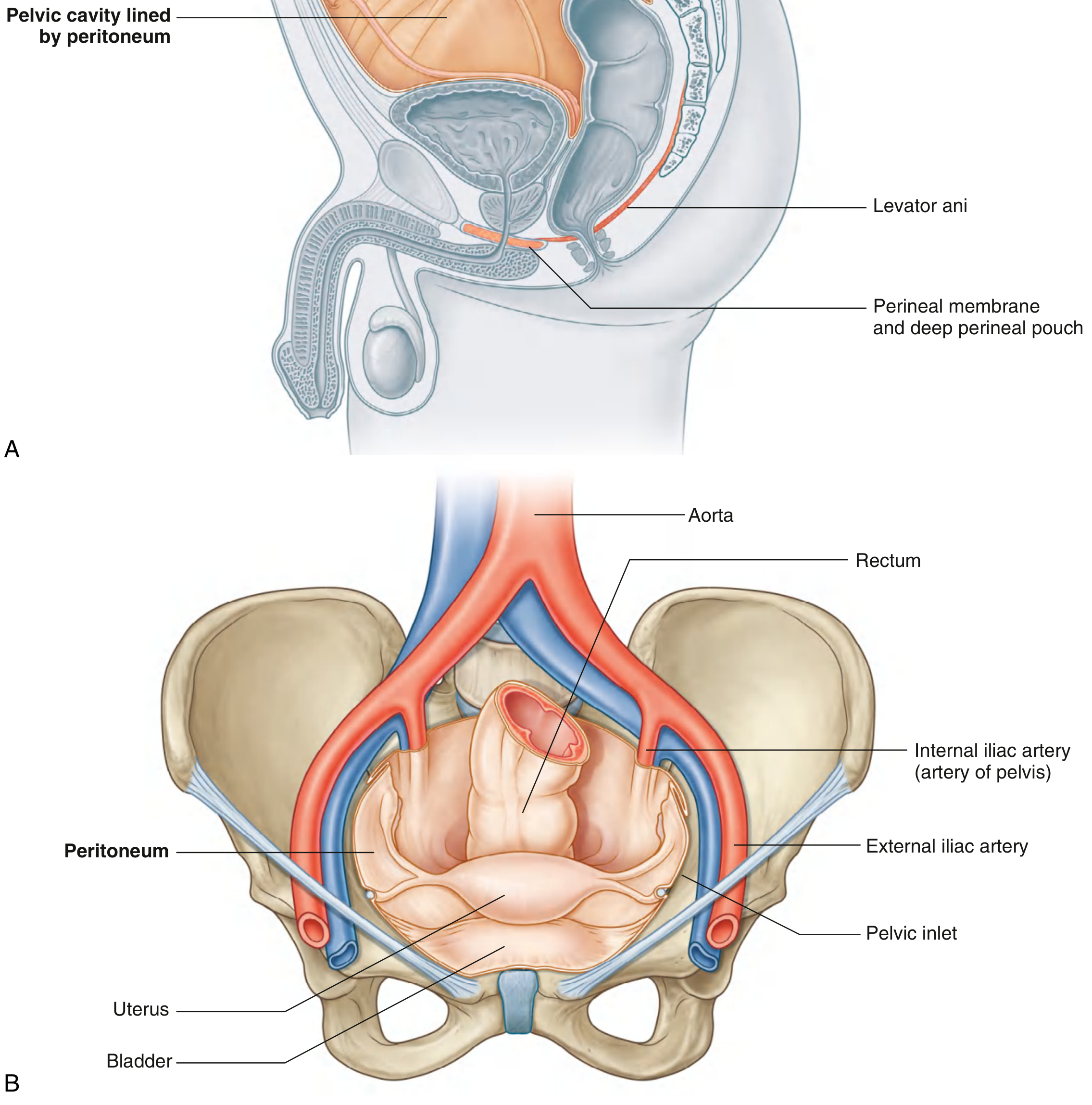
Arrangement (anterior to posterior):
- Bladder (anterior)
- Uterus (middle, between bladder and rectum)
- Rectum (posterior)
Peritoneal pouches in women:
- Vesicouterine (uterovesical) pouch - between bladder and uterus
- Rectouterine pouch (Pouch of Douglas / Cul-de-sac) - between uterus and rectum; the most dependent part of the female peritoneal cavity (fluid collection, endometriosis, ectopic pregnancy)
6. Fascia, Ligaments & Pelvic Spaces
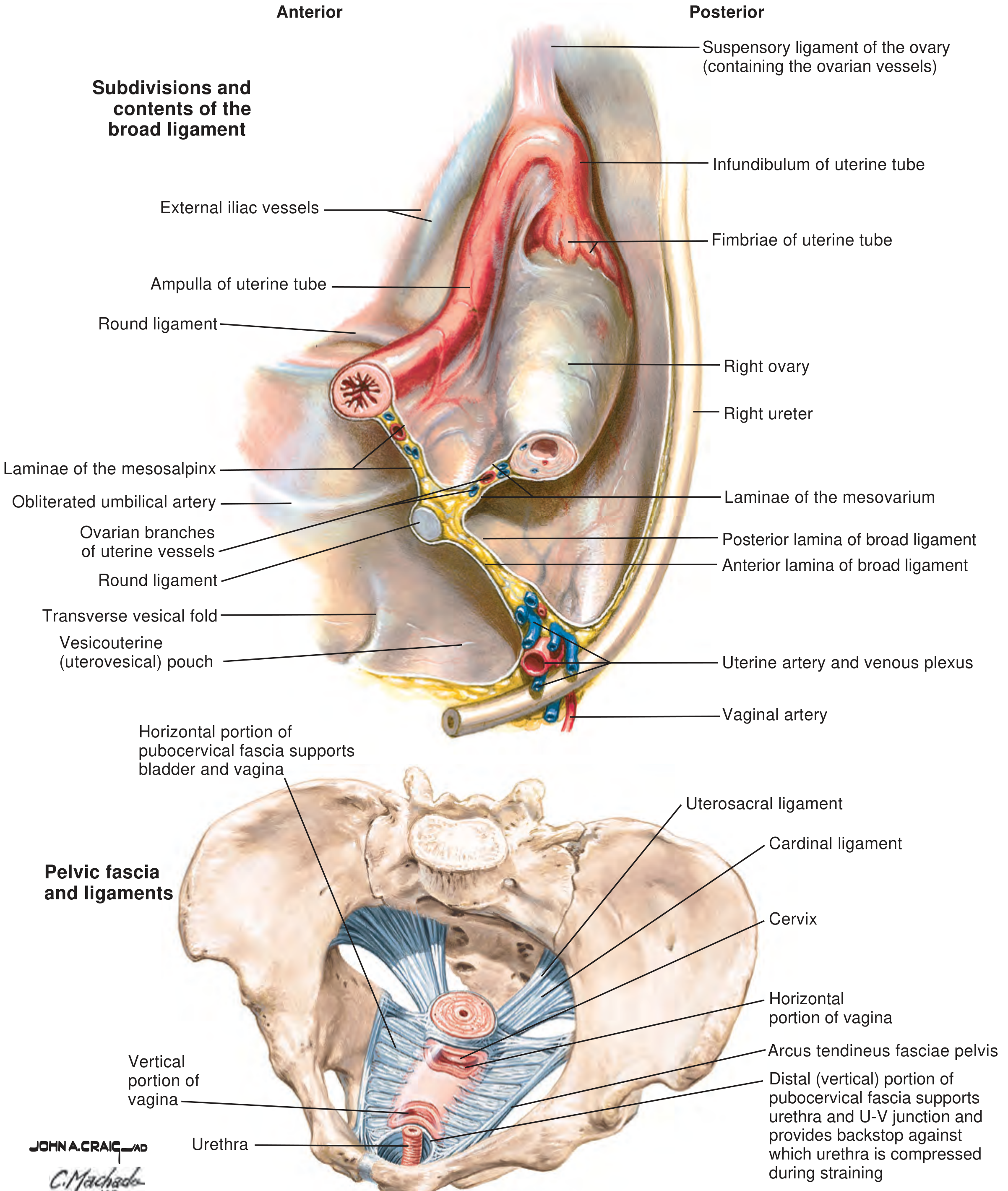
Ligamentous Support of the Uterus
| Ligament | Attachment | Contains / Notes |
|---|---|---|
| Broad ligament | Lateral uterine walls to pelvic side walls | Double peritoneal fold; contains uterine tubes, round ligament, ovarian ligament, uterine vessels, ureter |
| Round ligament | Uterine cornua to labia majora (via inguinal canal) | Maintains anteversion of uterus |
| Cardinal (Mackenrodt's) ligament | Cervix/upper vagina to lateral pelvic walls | Primary support for uterus against downward prolapse |
| Uterosacral ligament | Posterior cervix to sacrum | Pulls cervix posteriorly; maintains uterine anteflexion |
| Pubocervical fascia | Surrounds vagina anteriorly | Bladder support |
Pelvic Spaces (Surgically Important)
- Retropubic (prevesical) space of Retzius - between bladder and pubis
- Vesicovaginal space - between bladder and vagina
- Rectovaginal space - between rectum and vagina (plane for rectocele repair)
- Presacral space - between rectum and sacrum
- Paravesical spaces (bilateral)
- Pararectal spaces (bilateral)
7. Vasculature
Main arterial supply: Internal iliac artery (hypogastric artery)
Key branches relevant to gynecology:
- Uterine artery - crosses OVER the ureter at the base of the broad ligament ("water under the bridge" - ureter is at risk in hysterectomy)
- Ovarian artery - arises directly from the aorta (L2 level); runs in the suspensory ligament of the ovary
- Vaginal artery - branch of internal iliac
- Internal pudendal artery - perineal supply
Venous drainage: Uterine and vaginal venous plexuses drain into the internal iliac vein.
Lymphatic drainage (exam favorite):
- Ovaries → para-aortic nodes (L2 level)
- Uterine body → iliac nodes and para-aortic nodes
- Cervix → external iliac, internal iliac, and obturator nodes
- Vulva → superficial inguinal nodes
8. Nerve Supply
- Pelvic viscera: Inferior hypogastric (pelvic) plexus (sympathetic T10-L2 + parasympathetic S2-S4)
- Pelvic floor muscles: Levator ani nerve (S3-S4-S5)
- Perineum: Pudendal nerve (S2-S4) - runs through the pudendal (Alcock's) canal in the lateral wall of the ischiorectal fossa
- Obturator nerve (L2-L4): Runs through the obturator canal; at risk in lateral pelvic dissection
9. Clinical Correlations for Your Posting
| Anatomical Point | Clinical Significance |
|---|---|
| Ischial spine | Reference point for fetal station (0 station); pudendal nerve block |
| Pouch of Douglas | Fluid in this space on USS = haemoperitoneum / PID / ectopic |
| Uterine artery crossing ureter | "Water under the bridge" - ureteric injury risk in hysterectomy |
| Levator ani weakness | Pelvic organ prolapse (cystocele, rectocele, uterine prolapse) |
| Interspinous diameter <10 cm | Contracted pelvis - likely C-section needed |
| Ovarian lymphatics to para-aortic nodes | Ovarian cancer spreads to para-aortic nodes first |
| Subpubic angle | Narrow angle = android pelvis = obstructed labour risk |
Sources: Gray's Anatomy for Students (5e), Campbell-Walsh-Wein Urology (11e), THIEME Atlas of General Anatomy and Musculoskeletal System.
This is a shared conversation. Sign in to Orris to start your own chat.