Diagnostic approach to diabetes mellitus
Reading File
Finding Sources
Searching PubMed
"diabetes mellitus"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Diagnostic Approach to Diabetes Mellitus
Overview
Diabetes mellitus (DM) is a heterogeneous spectrum of metabolic disorders unified by impaired glucose homeostasis and hyperglycemia. The diagnostic approach involves recognizing the clinical presentation, selecting the appropriate biochemical test(s), interpreting results against established criteria, and classifying the type of diabetes to guide management.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Harrison's Principles of Internal Medicine, 22nd Ed.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
- Robbins & Kumar Basic Pathology
- Guyton and Hall Textbook of Medical Physiology
Step 1: Recognize Clinical Features
Classic symptoms that prompt diagnostic testing:
| Symptom | Mechanism |
|---|---|
| Polyuria | Osmotic diuresis from glucosuria |
| Polydipsia | Compensatory fluid intake |
| Polyphagia | Cellular starvation despite hyperglycemia |
| Unexplained weight loss | Fat/protein catabolism (especially T1DM) |
| Fatigue, blurred vision | Osmotic effects on lens and tissues |
| Acetone (fruity) breath | Ketoacidosis (T1DM, severe T2DM) |
| Recurrent infections | Impaired immune function |
Note: Many patients with T2DM are asymptomatic at diagnosis - hyperglycemia may be a relatively late development, which is why screening of at-risk populations is important.
Step 2: Diagnostic Tests
There are four accepted methods, any one of which is diagnostic:
1. Fasting Plasma Glucose (FPG)
- Fast for at least 8 hours (no caloric intake)
- Normal: <100 mg/dL (<5.6 mmol/L)
- Prediabetes (IFG): 100-125 mg/dL (5.6-6.9 mmol/L)
- Diabetes: ≥126 mg/dL (≥7.0 mmol/L)
- Limitation: Large biological variation (day-to-day), lower sensitivity than OGTT, risk of glycolysis in the test tube if processing is delayed.
2. Oral Glucose Tolerance Test (OGTT)
- 75 g anhydrous glucose dissolved in 300 mL water, ingested over 5 minutes
- Plasma glucose measured at fasting and at 2 hours
- For children: 1.75 g/kg body weight (up to 75 g maximum)
- Normal: 2h PG <140 mg/dL
- Prediabetes (IGT): 2h PG 140-199 mg/dL
- Diabetes: 2h PG ≥200 mg/dL (≥11.1 mmol/L)
Pre-test conditions required:
- Unrestricted diet with ≥150 g carbohydrate/day for 3 days prior
- 10-16 hour overnight fast
- Ambulatory outpatient (not hospitalized or acutely ill)
- Avoid medications affecting glucose tolerance (thiazides, corticosteroids, oral contraceptives)
- No smoking or caffeine during the test
- Remain seated; test begins between 7:00-9:00 AM
The glucose tolerance curve below illustrates the difference between normal and diabetic responses:
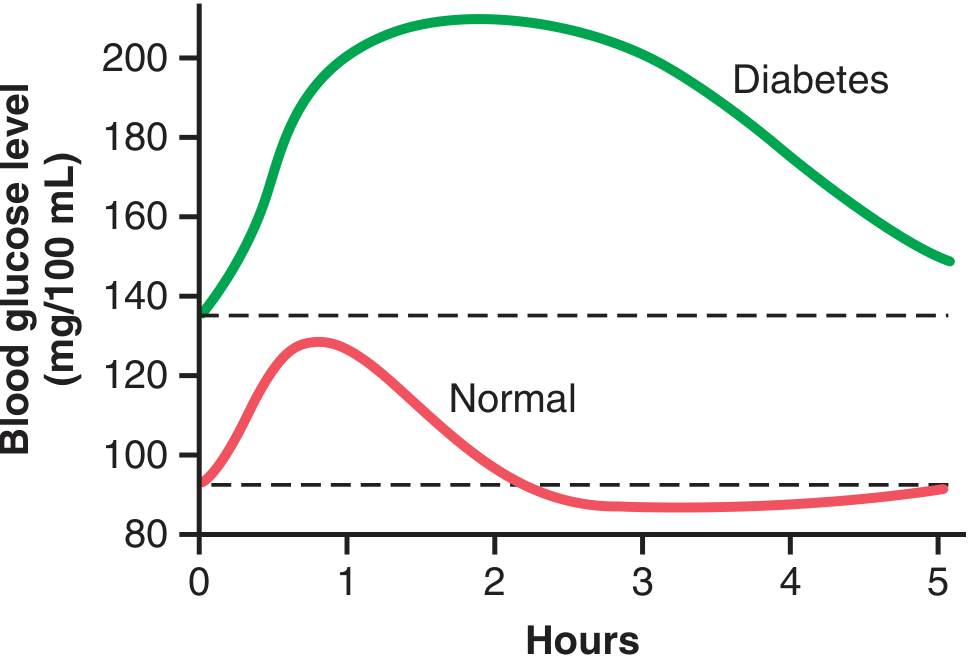
Figure: Glucose tolerance curve - normal person (pink) vs. diabetic person (green). In diabetes, peak glucose rises above 200 mg/dL and fails to return to baseline by 2 hours. (Guyton and Hall, Fig. 79.12)
When is OGTT specifically indicated?
- Diagnosis of gestational diabetes mellitus (GDM)
- Initial postpartum screening for T2DM in women with GDM
- Diagnosing impaired glucose tolerance (IGT)
- Evaluation of unexplained nephropathy/neuropathy/retinopathy with random glucose <140 mg/dL
3. HbA1c (Glycated Hemoglobin)
- Reflects average blood glucose over the previous 2-3 months (based on the ~120-day RBC lifespan)
- Prediabetes: 5.7-6.4%
- Diabetes: ≥6.5% (≥48 mmol/mol)
- Advantages over glucose testing: No fasting required, low biological variability, sample is stable, reflects long-term control
- Requirements: Must be performed in a laboratory using an NGSP-certified method standardized to the DCCT assay. Point-of-care assays should generally not be used for diagnosis (though some POC assays now meet NGSP criteria per Harrison's 2024 update).
- Limitations/Contraindications: Unreliable in hemolytic anemias, hemoglobinopathies (sickle cell, thalassemia), iron deficiency anemia, recent blood transfusion, pregnancy, or chronic kidney disease.
4. Random Plasma Glucose
- Taken at any time, regardless of last meal
- Diabetes: ≥200 mg/dL (≥11.1 mmol/L) with classic symptoms of hyperglycemia (polyuria, polydipsia, unexplained weight loss) or hyperglycemic crisis
- This criterion alone is diagnostic only when classic symptoms are present
Step 3: Confirmation Rule
| Situation | Rule |
|---|---|
| Classic symptoms + random PG ≥200 mg/dL | Single test is diagnostic |
| Unequivocal hyperglycemia + acute metabolic decompensation | No repeat needed |
| All other situations | Two abnormal results required - either from the same sample or on two separate occasions |
Important: Stress hyperglycemia from severe infections, burns, or trauma (due to catecholamines/cortisol) can cause transient hyperglycemia. Diabetes requires persistent hyperglycemia after resolution of the acute illness.
Step 4: Interpret the Spectrum - Normal, Prediabetes, Diabetes
| Category | FPG (mg/dL) | 2h OGTT (mg/dL) | HbA1c (%) |
|---|---|---|---|
| Normal | <100 | <140 | <5.7 |
| Prediabetes (IFG/IGT) | 100-125 | 140-199 | 5.7-6.4 |
| Diabetes | ≥126 | ≥200 | ≥6.5 |
- Prediabetes confers 5-10% annual risk of progressing to T2DM; risk is highest with obesity and family history
- Individuals with both IFG and IGT have a higher conversion rate than either alone
- Prediabetes also carries elevated cardiovascular disease risk independent of overt diabetes
Step 5: Classify the Type of Diabetes
| Type | Mechanism | Key Features |
|---|---|---|
| Type 1 DM | Autoimmune destruction of β-cells → absolute insulin deficiency | Young (but can occur at any age), lean, prone to DKA, low/undetectable C-peptide, positive autoantibodies (GAD65, IA-2, ZnT8, IAA) |
| Type 2 DM | Peripheral insulin resistance + relative β-cell failure | Older (increasingly younger), obese, insidious onset, plasma insulin normal or elevated initially |
| Gestational DM (GDM) | Placental hormones → insulin resistance during pregnancy | Diagnosed at 24-28 weeks; use 1-step (75g OGTT) or 2-step (50g screen then 100g OGTT) protocol |
| MODY (Monogenic) | Single gene defects (HNF1A, GCK, HNF4A) | Autosomal dominant; family history; young onset; no autoantibodies |
| Secondary Diabetes | Pancreatic disease, endocrinopathies (Cushing, acromegaly), drugs (corticosteroids, thiazides, atypical antipsychotics) | Context-dependent |
| Atypical/Ketosis-prone | Features of both T1 and T2 | African American/Asian heritage; may not need long-term insulin |
Differentiating T1 from T2 by lab:
- Plasma insulin/C-peptide: Very low or undetectable in T1; normal or elevated in early T2
- Autoantibodies (GAD65, IA-2, ZnT8, IAA): Positive in ~95% of T1DM
- After glucose load: T2DM shows exaggerated insulin secretion relative to basal; T1DM shows flat or no response
Step 6: Additional Tests in Specific Contexts
| Test | Indication |
|---|---|
| Plasma insulin / C-peptide | Distinguish T1 from T2; assess residual β-cell function |
| Islet autoantibodies (GAD65, IA-2, ZnT8) | Confirm T1DM; screen relatives |
| Urinalysis for glucose/ketones | Rapid screening; glucosuria suggests hyperglycemia; ketonuria signals DKA |
| Urine/serum ketones | Evaluate for DKA in symptomatic T1DM |
| Intravenous GTT (IVGTT) | Malabsorption, post-gastric surgery, research setting for first-phase insulin response |
| Genetic testing (MODY panel) | Young onset, non-obese, strong family history, autoantibody-negative |
| Lipid panel, BP, renal function | Comorbidities that accelerate cardiovascular risk |
| Screening for complications | At diagnosis and periodically: retina, urine albumin, nerve conduction, foot exam |
Screening (Who to Test Without Symptoms?)
The ADA recommends testing for T2DM in:
- Adults ≥35 years of age (regardless of BMI)
- Overweight/obese adults (BMI ≥25, or ≥23 in Asian Americans) with one or more risk factors:
- First-degree relative with diabetes
- High-risk ethnicity (African American, Latino, Native American, Asian American, Pacific Islander)
- History of GDM or delivering a baby >9 lbs
- Hypertension (≥140/90 or on antihypertensive therapy)
- Dyslipidemia (HDL <35 mg/dL or TG >250 mg/dL)
- Polycystic ovary syndrome (PCOS)
- Physical inactivity
- Previous prediabetes
- HIV infection
Summary Algorithm
Clinical suspicion or screening trigger
|
v
Choose test: FPG (fasting ≥8h) | OGTT (75g, 2h PG) | HbA1c | Random PG
|
v
Classic symptoms + random PG ≥200? --> Diagnose DM (single test sufficient)
|
No classic symptoms?
v
Result meets DM threshold?
Yes --> Repeat on separate occasion (OR use second test from same sample)
Both abnormal --> Diagnose DM
|
v
Result in prediabetes range? --> Lifestyle intervention, rescreen q1 year
|
v
Normal? --> Rescreen every 3 years (or annually if high risk)
|
v
Classify type (T1, T2, GDM, MODY, secondary) based on clinical features + C-peptide + autoantibodies
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Box 47.3 (Criteria for Diagnosis), p. 1731-1732
- Robbins & Kumar Basic Pathology - Diagnosis section, p. 2425-2435
- Guyton and Hall Medical Physiology - Physiology of Diagnosis, p. 976-977
- Harrison's Principles of Internal Medicine, 22nd Ed. - Standards of Care 2024 update
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Pathophysiology and Diagnosis, p. 2271-2276
- Tintinalli's Emergency Medicine - Diagnosis, p. 2555-2558
This is a shared conversation. Sign in to Orris to start your own chat.