Explain herniactomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hernia repair"[MeSH Terms] AND "surgical techniques"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to write a full, well-cited explanation.
Herniorrhaphy (Hernia Repair Surgery)
Note on terminology: The user asked about "herniactomy" - the correct surgical term is herniotomy (sac excision alone) or herniorrhaphy (repair including wall reconstruction). Both are explained below.
What Is a Hernia?
A hernia occurs when an organ or tissue (most commonly bowel or omentum) pushes through a defect or weakness in the surrounding muscle or fascial wall. The most common type is the inguinal hernia - accounting for the vast majority of hernia repairs worldwide.
Terminology Clarified
| Term | Meaning |
|---|---|
| Herniotomy | Simple excision (cutting away) of the hernia sac alone - no wall repair |
| Herniorrhaphy | Sac removal + surgical repair/strengthening of the abdominal wall |
| Hernioplasty | Repair using a prosthetic mesh to reinforce the defect |
In children, herniotomy alone is sufficient because the inguinal canal musculature is still developing. In adults, herniotomy alone has a high recurrence rate and some form of muscle-strengthening repair (herniorrhaphy) is mandatory. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Indications for Surgery
- Symptomatic inguinal hernia (pain, dragging discomfort)
- Increasing hernia size
- Irreducible (incarcerated) hernia
- Strangulated hernia (emergency - ~5% of cases) - time-critical due to risk of bowel infarction
- Asymptomatic small direct hernias in elderly patients may be managed conservatively; surgical trusses are not recommended
Surgical Approaches
1. Herniotomy (Children)
In children with a lateral (indirect) hernia due to a patent processus vaginalis, it is sufficient to simply excise and close the hernia sac. The steps are:
- Incision over the inguinal canal, Scarpa's fascia opened
- External oblique aponeurosis incised
- Cremaster opened to identify the sac
- Sac mobilised from the testicular vessels and vas deferens
- Sac divided, twisted to reduce any contents, and transfixed/ligated at the internal ring
- Wound closed in layers
2. Open Suture Repair (Herniorrhaphy)
Bassini Repair (1890) - the historical gold standard:
- The inguinal canal is entered by opening the external oblique aponeurosis
- Spermatic cord is dissected free
- For lateral hernias: sac is separated from cord, opened, contents reduced, sac closed at its neck and excised
- For medial hernias: sac is inverted and the transversalis fascia is suture plicated
- Sutures are placed between the conjoint tendon (above) and inguinal ligament (below) from pubic tubercle to deep inguinal ring - strengthening the posterior wall
Shouldice Repair - the best suture-only technique:
- The transversalis fascia is opened centrally and then closed to create a two-layered (double-breasted) posterior wall
- Expert centres report lifetime failure rates of less than 2%, but it is technically demanding
- Most surgeons achieve similar results to Bassini
Maloney Darn - uses continuous non-absorbable nylon or polypropylene suture darned between the conjoint tendon and inguinal ligament; gives excellent results and is the most common operation in countries where mesh is too expensive.
Desarda Repair - a 1-2 cm strip of external oblique aponeurosis is isolated and sutured to reinforce the posterior wall; considered equivalent to Shouldice repair. - Bailey and Love's, 28th Ed.
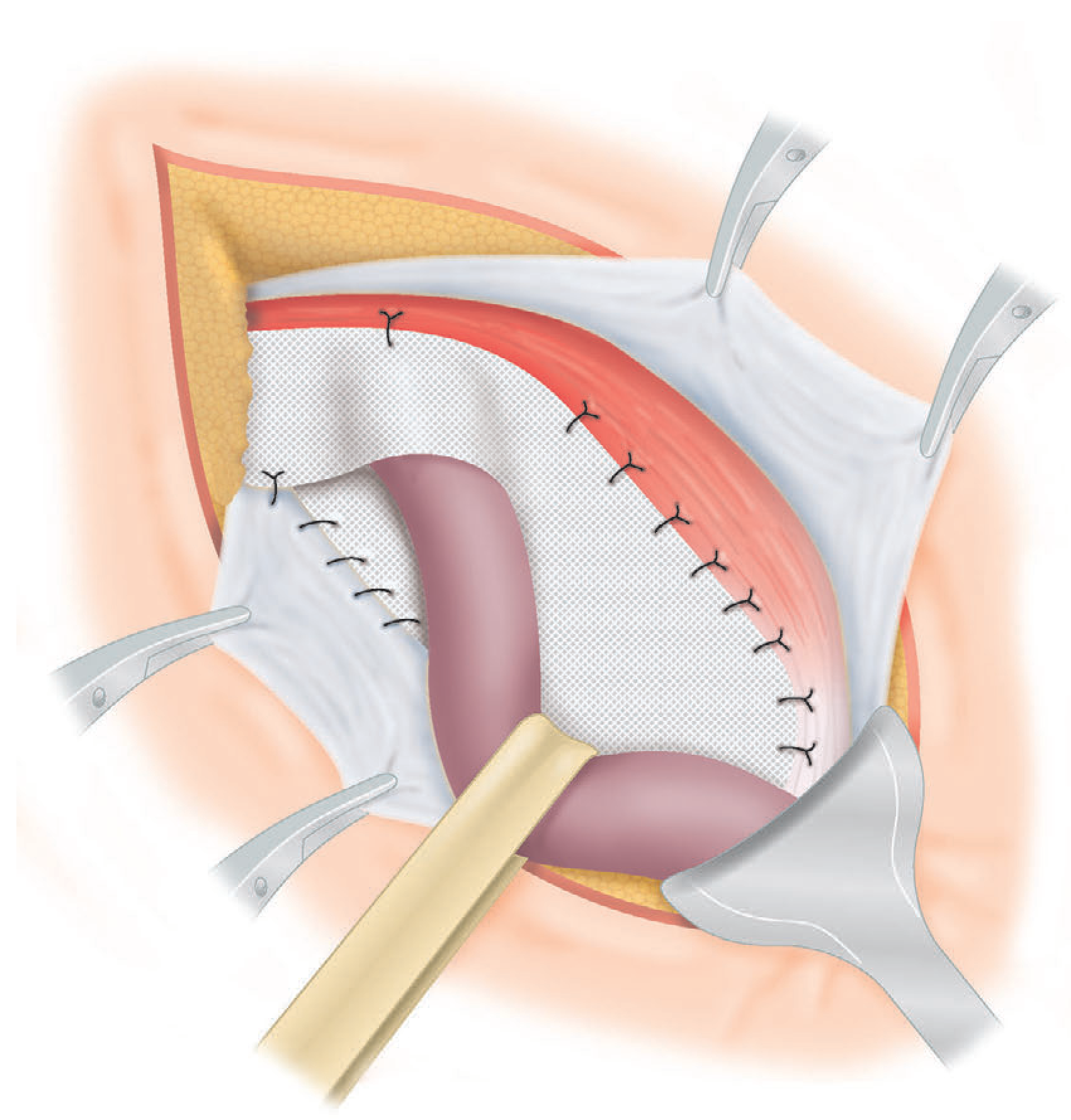
3. Open Mesh Repair (Hernioplasty) - Most Common Today
Lichtenstein Tension-Free Repair (since 1980s) - the most common operation for inguinal hernia in resource-rich countries:
- Initial dissection identical to Bassini
- Hernia sac removed; medial defect closed if present
- A flat polypropylene mesh (8 x 15 cm) is placed over the posterior wall, behind the spermatic cord
- The mesh is slit to wrap around the spermatic cord at the deep inguinal ring
- Loose sutures fix the mesh to the inguinal ligament and conjoint tendon
Two key advantages: lower recurrence rates and faster postoperative recovery. However, chronic pain is the most reported complication, with rates as high as 20%. - Bailey and Love's, 28th Ed.
4. Laparoscopic Repair
Two main techniques:
| Technique | Full Name | Description |
|---|---|---|
| TEP | Totally Extraperitoneal | Mesh placed in the preperitoneal space without entering the peritoneal cavity |
| TAPP | Transabdominal Preperitoneal | Peritoneal cavity entered, mesh placed behind the peritoneum |
Both approaches require general anaesthesia and place a large mesh in the preperitoneal space. Advantages include:
- Less postoperative pain (particularly for bilateral or recurrent hernias)
- Faster return to normal activities
- Lower rates of chronic pain vs. Lichtenstein
Robot-assisted laparoscopic repair is increasingly used; the enhanced surgical view and ergonomic comfort for the surgeon are recognised benefits, though little additional patient benefit has been demonstrated and the cost is hard to justify for simple inguinal repair.
Mesh Materials
Three main classes of synthetic mesh are used:
| Material | Properties |
|---|---|
| Polypropylene | Inert, hydrophobic monofilament; resists bacterial ingrowth; most commonly used |
| Polyester | Hydrophilic; encourages microvascular ingrowth |
| PTFE (polytetrafluoroethylene) | Flat sheets; very inert; resists both tissue ingrowth and adhesion formation |
Mesh can be used to: bridge a defect (patch over), plug a defect (pushed into the defect - largely abandoned due to "meshoma" formation), or augment a primary suture repair. Inlay (edge-to-edge suturing into the defect with no overlap) is not recommended. - Bailey and Love's, 28th Ed.
Emergency Hernia Surgery
About 5% of inguinal hernias present as an irreducible, painful lump that may progress to strangulation and bowel infarction. Key points:
- Time is critical in the presence of ischaemic bowel
- ~20% of emergency cases require bowel resection
- May require conversion to midline laparotomy
- Synthetic mesh is acceptable unless there is significant contamination (with appropriate antibiotics)
Complications
| Category | Complications |
|---|---|
| Immediate | Haematoma (subcutaneous vessels; rarely inferior epigastric/iliac vessels), urinary retention, femoral nerve blockade from local anaesthetic |
| Short-term | Wound infection (<5% in groin herniorrhaphy), seroma, testicular swelling |
| Long-term | Chronic groin pain (most common overall - up to 20% with mesh), hernia recurrence, injury to vas deferens causing infertility (mesh can obstruct vas in inguinal canal), nerve injury (ilio-inguinal, iliohypogastric, genitofemoral nerves) |
| Rare | Enterocutaneous fistula (2-5% of all ECF cases involve prior herniorrhaphy) |
Anaesthesia
Herniorrhaphy can be performed under local, regional, or general anaesthesia with minimal risk even in high-risk patients. Postoperative pain is managed by iliohypogastric and ilio-inguinal nerve blocks using bupivacaine 0.5% (10 mL each) injected 2 cm medial to the anterior superior iliac spine, providing relief for up to 6 hours. - Pye's Surgical Handicraft, 22nd Ed.
Choosing the Right Operation
No single operation suits all hernias. Factors to consider:
- Surgeon's skills and available equipment
- Patient type (age, fitness, bilateral vs. unilateral, recurrent vs. primary)
- Hernia characteristics (direct vs. indirect, size of defect)
In summary, the Lichtenstein open mesh repair is the dominant operation in resource-rich settings; laparoscopic TEP/TAPP is preferred for bilateral or recurrent hernias; and suture-only repairs (Shouldice, Maloney, Desarda) remain the standard where mesh is unavailable. - Bailey and Love's, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.