Flow chart of OHA which one to start, for which range of HbA1c
"type 2 diabetes" AND "HbA1c" AND "antidiabetic" treatment algorithm
"type 2 diabetes" AND "glycemic control" AND "guidelines"
"type 2 diabetes" AND "metformin" AND "treatment initiation"
A detailed medical flowchart titled "OHA Selection Algorithm Based on HbA1c in Type 2 Diabetes Mellitus". The chart flows top to bottom with clearly labeled decision boxes and arrows. Starting point: "Newly Diagnosed T2DM - Start Lifestyle Modification (Diet + Exercise)". Then branches based on HbA1c levels: Branch 1: HbA1c 6.5-7.5% (at or near target) → Monotherapy: Metformin (first-line) → if not tolerated: DPP-4 inhibitor or SGLT-2 inhibitor or GLP-1 RA. Branch 2: HbA1c 7.5-9% (above target) → Dual therapy: Metformin + one of the following (choose based on comorbidity): SGLT-2i (if CVD/HF/CKD), GLP-1 RA (if obesity/CVD), DPP-4i (if neutral weight), SU (if cost concern), Pioglitazone (if NAFLD). Branch 3: HbA1c 9-10% (significantly above target) → Dual or Triple therapy: Metformin + 2 agents OR if symptomatic consider insulin + OHA. Branch 4: HbA1c >10% or symptomatic hyperglycemia → Insulin-based therapy (Basal insulin ± OHA), consider GLP-1 RA combination. At the bottom: Re-evaluate HbA1c every 3 months → if not at goal, intensify therapy. Target HbA1c goals shown in a legend box: General: <7%, Young/no comorbidities: <6.5%, Elderly/CVD/limited life expectancy: <8%. Use clean medical diagram style, color-coded boxes (green for mild, yellow for moderate, orange for high, red for very high HbA1c), professional clinical appearance.
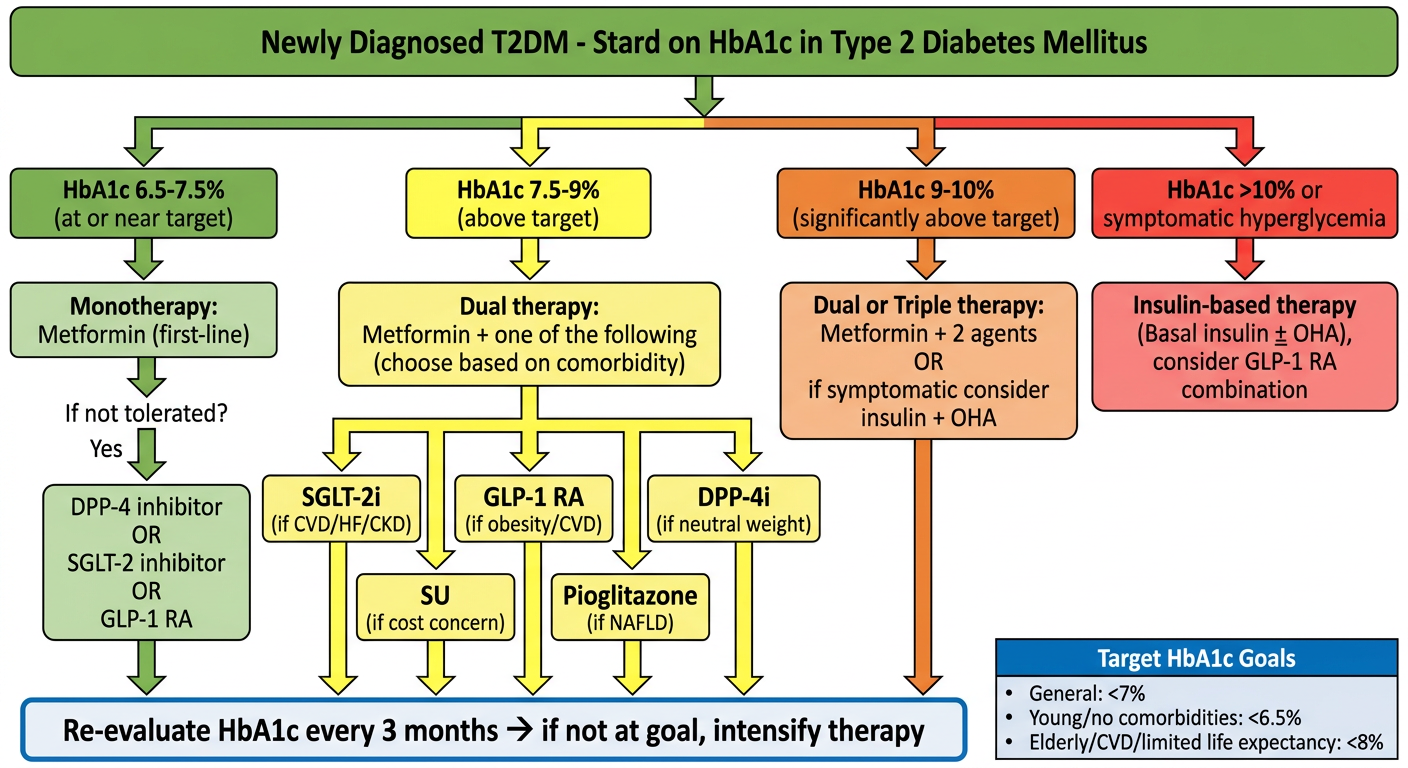
OHA Algorithm: Which Drug, for Which HbA1c Range
Step 0 - At Diagnosis (Any HbA1c)
HbA1c 6.5% - 7.5% (at or near target)
- Metformin - first-line universally (unless contraindicated: eGFR <30, contrast dye, lactic acidosis risk)
- Alternatives if metformin not tolerated:
- DPP-4 inhibitor (sitagliptin, vildagliptin) - weight neutral
- GLP-1 RA (semaglutide, liraglutide) - if obesity
- SGLT-2 inhibitor (empagliflozin, dapagliflozin) - if CVD/CKD
HbA1c 7.5% - 9% (above target)
| Comorbidity | Add-on Agent |
|---|---|
| Established CVD / high CV risk | GLP-1 RA or SGLT-2i |
| Heart failure / CKD | SGLT-2 inhibitor |
| Obesity, weight loss needed | GLP-1 RA |
| Hypoglycemia risk (elderly) | DPP-4i or SGLT-2i |
| Cost constraint | Sulfonylurea (glimepiride, glipizide) |
| NAFLD / insulin resistance | Pioglitazone |
HbA1c 9% - 10% (significantly above target)
- Metformin + 2 agents (e.g., GLP-1 RA + SGLT-2i), OR
- If symptomatic hyperglycemia: add basal insulin (glargine/degludec) 10 units at bedtime + continue OHA
HbA1c >10% or Symptomatic (polyuria, polydipsia, weight loss)
- Basal insulin (0.1-0.2 units/kg/day) + Metformin
- Consider GLP-1 RA + basal insulin combination (reduces dose requirement)
- Once HbA1c improves, may de-intensify if hypoglycemia occurs
Glycemic Targets (ADA/AACE)
| Patient Profile | HbA1c Target |
|---|---|
| Young, no comorbidities | < 6.5% |
| General adult T2DM | < 7.0% |
| Elderly, CVD, limited life expectancy | < 7.5% - 8.0% |
| Pregnancy | < 6.0% (fasting <95 mg/dL) |
Key Points
- Re-check HbA1c every 3 months if not at goal; every 6 months if controlled
- SGLT-2i and GLP-1 RA are preferred add-ons when atherosclerotic CVD, heart failure, or CKD is present - independent of glucose lowering
- Sulfonylureas carry hypoglycemia risk; avoid as first add-on in the elderly
- Pioglitazone is contraindicated in heart failure and bladder cancer history
- A1C <6.5%-7% is associated with lowest risk of microvascular complications
Everything about VIPoma
"VIPoma" AND "vasoactive intestinal peptide"
VIPoma - Complete Overview
Definition & Eponym
- Verner-Morrison syndrome (after the two physicians who first described it in 1958)
- Pancreatic cholera syndrome
Epidemiology
- Incidence: approximately 1 in 10 million per year - extremely rare
- Mean age at presentation: 42-51 years
- No clear gender predominance
- Most are sporadic, but a minority arise in the setting of MEN1 (Multiple Endocrine Neoplasia type 1)
Pathophysiology
- VIP binds to receptors on intestinal epithelial cells → stimulates adenylyl cyclase → ↑ cAMP → massive chloride and fluid secretion into the gut lumen (mechanism identical to cholera toxin)
- Increases smooth-muscle contractility → profuse diarrhea
- Inhibits gastric acid secretion → achlorhydria
- Stimulates renin secretion → secondary hyperaldosteronism → additional potassium wasting (compounding hypokalemia beyond just fecal losses)
- Promotes hepatic glycogenolysis → glucose intolerance/hyperglycemia
- Vasodilatory effect → cutaneous flushing (minority of patients)
- Stimulates calcium reabsorption → mild hypercalcemia
Clinical Features (WDHA Syndrome)
| Feature | Details |
|---|---|
| Watery diarrhea | Almost universal; initially intermittent, becomes unrelenting. Stool volume 6-8 L/day (sometimes up to 20 L). "Weak tea" appearance, no steatorrhea. Persists during fasting - key feature of secretory diarrhea |
| Hypokalemia | Often severe (<2.5 mEq/L); from fecal K+ loss + secondary hyperaldosteronism |
| Achlorhydria | VIP inhibits gastric acid secretion |
| Weight loss | ~75% of patients, from volume depletion and malnutrition |
| Volume depletion | ~50% of patients - can be life-threatening |
| Metabolic acidosis | From bicarbonate loss in diarrhea |
| Hyperglycemia | ~50% - from hepatic glycogenolysis |
| Hypercalcemia | ~50% - mild; mechanism not fully clarified |
| Flushing | Minority - erythematous rash over head/trunk from vasodilation |
| Muscle weakness/lethargy/nausea | Secondary to hypokalemia |
| Potentially fatal arrhythmias | From severe electrolyte imbalances |
The diarrhea is secretory in nature - it does NOT abate with fasting and has NO osmotic gap on stool osmolality testing. This is the key feature distinguishing it from osmotic diarrhea.
Tumor Characteristics
- 80-90% arise in the pancreas (most commonly body and tail, 70%)
- 10-20% are extrapancreatic: retroperitoneum, chest, intestine, adrenal gland
- Neural crest tumors (neuroblastomas, ganglioneuroblastomas, ganglioneuromas) and pheochromocytomas can also produce VIP and cause VIPoma syndrome
- Usually large, solitary lesions
- High malignancy rate: 50-89% are metastatic at presentation (most commonly to the liver)
- 5-year survival: >90% for localized disease vs ~60% for metastatic disease
Diagnosis
Step 1 - Clinical Suspicion
- Large-volume (>1 L/day) secretory diarrhea that persists during fasting
- Associated hypokalemia and achlorhydria
Step 2 - Biochemical Confirmation
- Serum VIP level >200 pg/mL (fasting) - markedly elevated (normal upper limit: 75-190 pg/mL; VIPoma patients may reach 7200 pg/mL)
- Because VIP secretion is episodic, draw samples during active diarrhea, not during remission; repeat measurements may be needed
- Confirm stool volume >0.5-1.0 L/day during a fast
- Note: Mildly elevated VIP can occur in heart failure, renal disease, inflammatory bowel disease, small bowel resection, radiation enteritis - these must be excluded
Step 3 - Rule Out Other Causes of Secretory Diarrhea (Differential Diagnosis)
| Entity | Distinguishing Workup |
|---|---|
| Villous adenoma | Lower GI endoscopy |
| Laxative abuse | Stool for phenolphthalein; urine screen |
| Celiac disease | Fecal fat, D-xylose test, small bowel biopsy |
| Gastrinoma (ZES) | Serum gastrin, gastric acid analysis, secretin stimulation |
| Carcinoid syndrome | Urinary 5-HIAA, serum serotonin |
| Infectious/parasitic | Stool culture, O&P, C. difficile toxin |
| IBD | Colonoscopy, upper GI series |
Step 4 - Tumor Localization
- CT scan (abdomen/pelvis with IV contrast) - first-line imaging; most VIPomas are large and easily seen
- Endoscopic ultrasound (EUS) - most sensitive for small pancreatic tumors
- Somatostatin receptor scintigraphy (SRS) / Octreoscan - best for detecting metastatic disease; most reliable
- MRI - alternative to CT
- DOTATATE PET scan - increasingly used, highly sensitive for NET metastases
- Preoperative localization is critical since 10% of tumors are extrapancreatic (retroperitoneum or chest)
Management
A. Immediate Supportive Care (Priority #1)
- Aggressive IV fluid resuscitation (large volumes often required)
- IV potassium replacement (severe hypokalemia needs aggressive correction)
- Correct metabolic acidosis
- Electrolyte monitoring
B. Medical Therapy - Somatostatin Analogues
- Reduce circulating VIP levels
- Eliminate diarrhea in ~50% of patients
- Decrease stool volume in the majority of the remaining patients
- Effect is usually durable but may require dose escalation over time
- Useful both as pre-operative bridge (stabilizing the patient before surgery) and for unresectable/metastatic disease (long-term symptom control)
- Octreotide LAR 20-30 mg IM every 4 weeks is the long-acting formulation used
- High-dose corticosteroids - some benefit but poorly tolerated
- Antimotility agents (loperamide) - inferior to octreotide
C. Surgical Treatment
- Localized disease in the pancreatic tail (most common): Distal pancreatectomy (often curative)
- Extrapancreatic tumors: retroperitoneal or thoracic resection
- Pre-operative stabilization with fluids/electrolytes and octreotide is mandatory before operating
- Even in metastatic disease, cytoreductive surgery (debulking) is recommended to reduce tumor burden and improve symptom control
D. Management of Metastatic Disease
- Hepatic metastases are present in the majority at diagnosis
- Surgical resection of liver metastases (when feasible)
- Hepatic artery embolization or chemoembolization (TACE)
- Radiofrequency ablation (RFA) or other ablative strategies
- Systemic chemotherapy: Streptozotocin + 5-fluorouracil (historical standard); newer options include everolimus, sunitinib
- PRRT (Peptide Receptor Radionuclide Therapy) with 177Lu-DOTATATE for somatostatin receptor-positive tumors
- Interferon-alpha (second-line)
VIPoma in MEN1
- VIPomas have been reported in a few patients with MEN1 (Multiple Endocrine Neoplasia type 1)
- MEN1-associated PanNETs are typically multiple
- Surgery is approached cautiously in MEN1 given the high probability of multiple/recurrent tumors
- For symptomatic or growing tumors >2 cm, surgical resection may still be considered
Prognosis
| Scenario | 5-Year Survival |
|---|---|
| Localized (resected) | >90% |
| Metastatic disease | ~60% |
| Resected metastatic disease | Variable; cytoreduction improves symptoms significantly |
Key Distinguishing Features from Other Functional PanNETs
| Tumor | Key Syndrome | Key Hormone | Key Finding |
|---|---|---|---|
| VIPoma | WDHA / Verner-Morrison | VIP | Massive secretory diarrhea, hypokalemia, achlorhydria |
| Insulinoma | Whipple's triad | Insulin | Fasting hypoglycemia |
| Gastrinoma (ZES) | Zollinger-Ellison | Gastrin | Intractable peptic ulcers, acid hypersecretion |
| Glucagonoma | 4D syndrome | Glucagon | Necrolytic migratory erythema, diabetes, DVT |
| Somatostatinoma | Inhibitory syndrome | Somatostatin | Diabetes, cholelithiasis, steatorrhea |
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 1777-1778, 1795
- Sabiston Textbook of Surgery, 21st ed., pp. 1593-1594
- Mulholland & Greenfield's Surgery, 7th ed., pp. 2752-2755
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Robbins & Cotran Pathologic Basis of Disease
- Fischer's Mastery of Surgery, 8th ed., p. 5142