cereberrum
Reading File
Finding Sources
Searching the Web
cerebrum anatomy functions lobes overview
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of the cerebrum (note: the correct spelling is cerebrum, not "cereberrum") drawn from authoritative neuroscience textbooks.
The Cerebrum
Overview
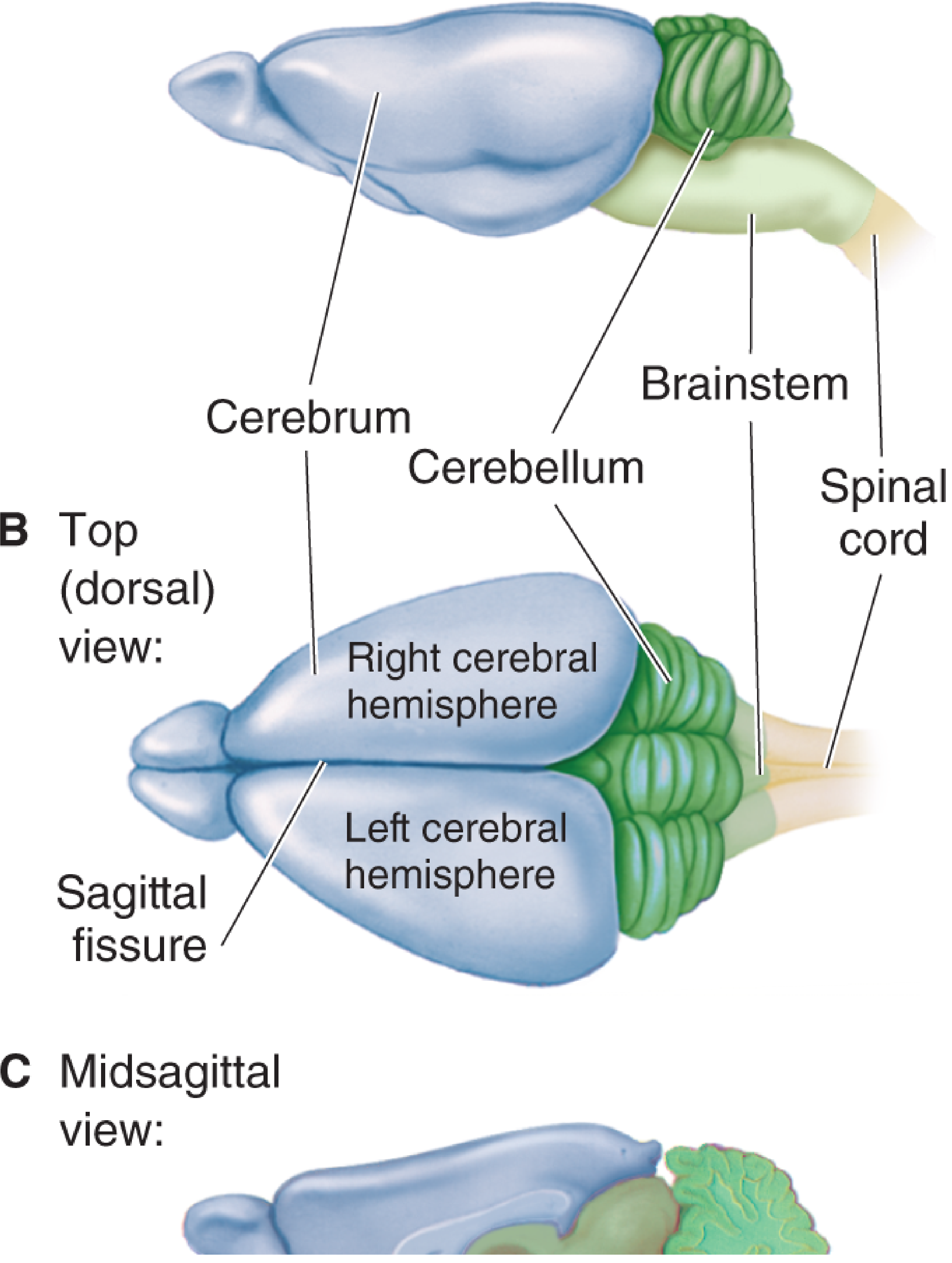
The cerebrum is the rostral-most and largest part of the brain, forming the bulk of the central nervous system. It sits atop the brainstem, from which it and the cerebellum sprout. The cerebrum is divided down the middle by the deep sagittal fissure into two cerebral hemispheres - left and right.
- The right hemisphere receives sensations from and controls movements of the left side of the body.
- The left hemisphere is concerned with the right side of the body.
(Neuroscience: Exploring the Brain, 5th Ed.)
Surface Anatomy: Gyri, Sulci, and Fissures
The cerebrum has a convoluted surface:
- Gyri - the bumps/ridges
- Sulci - the grooves
- Fissures - especially deep grooves (e.g., the lateral/Sylvian fissure, sagittal fissure)
Key landmarks:
- Precentral gyrus (anterior to central sulcus) - controls voluntary movement
- Postcentral gyrus (posterior to central sulcus) - processes somatic sensation (touch)
- Superior temporal gyrus - involved in audition (hearing)
The folded surface dramatically increases the cortical surface area that fits within the skull.
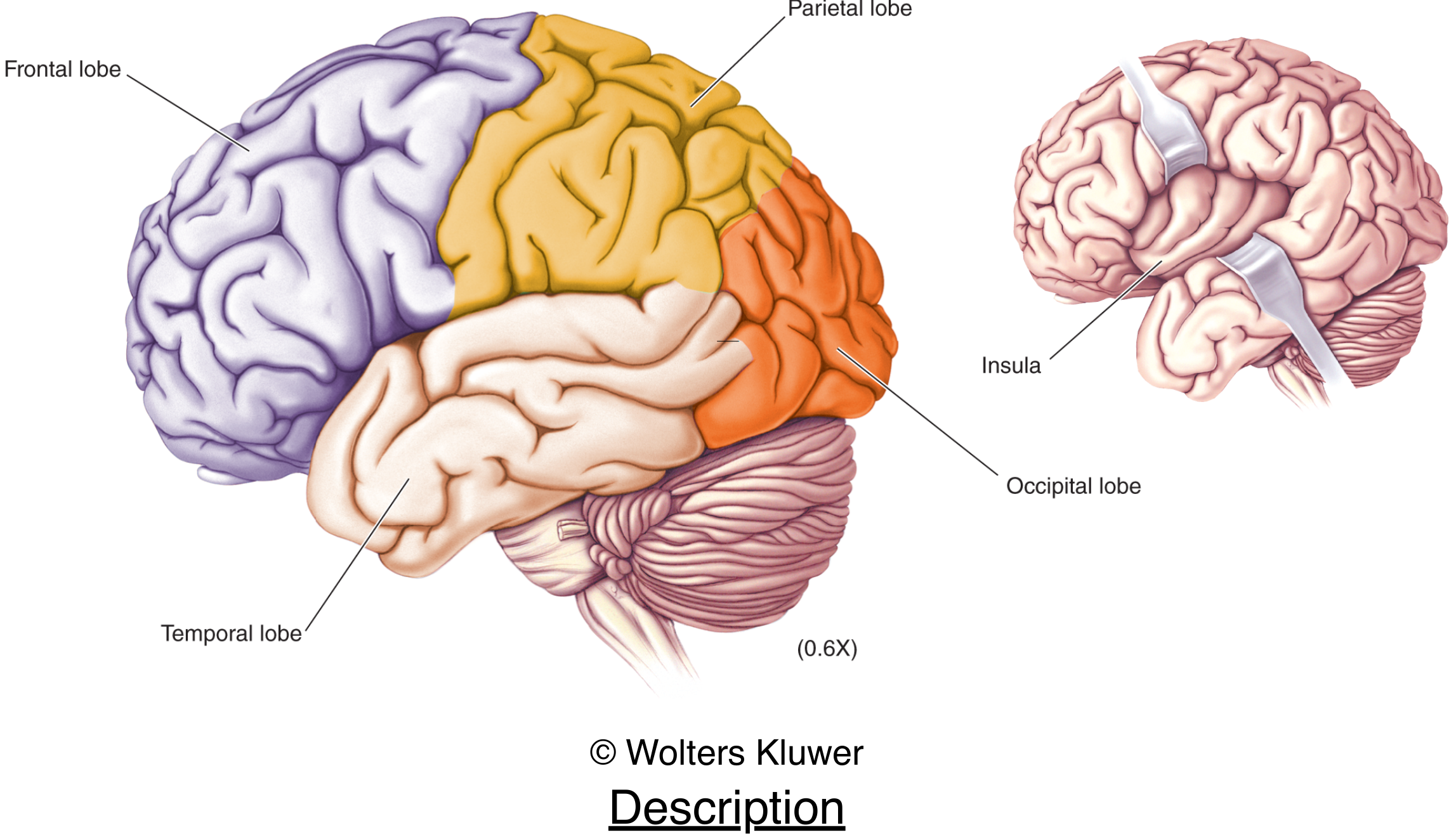
Lobes of the Cerebrum
By convention, the cerebrum is subdivided into lobes named after the overlying skull bones:
| Lobe | Location | Key Functions |
|---|---|---|
| Frontal | Anterior, largest lobe (~30% of cerebrum in humans) | Voluntary movement (motor cortex), executive function, personality, language (Broca's area in left hemisphere) |
| Parietal | Posterior to frontal, separated by central sulcus | Somatic sensation, spatial processing, sensory integration |
| Temporal | Ventral to lateral fissure | Auditory processing, memory (hippocampus), language comprehension (Wernicke's area) |
| Occipital | Posterior pole of the cerebrum | Visual processing (primary visual cortex) |
| Insula | Buried within the lateral fissure | Taste (gustatory cortex), interoception, emotional processing |
(Neuroscience: Exploring the Brain, 5th Ed.; Adams and Victor's Principles of Neurology, 12th Ed.)
Cerebral Cortex Organization
The cerebral cortex - the outermost layer of the cerebrum - is organized into functionally distinct areas (originally mapped by Brodmann):
- Primary sensory areas: Visual (occipital), auditory (temporal), somatosensory (parietal)
- Primary motor area: Precentral gyrus of the frontal lobe
- Association areas: Large cortical regions not assigned to a single sensory/motor function - include the prefrontal cortex (cognition, working memory), posterior parietal cortex (spatial awareness), and inferotemporal cortex (object recognition, face processing)
Internal Structure
Beneath the cortex lie:
- White matter - axon tracts connecting cortical areas
- Corpus callosum - a massive fiber bundle connecting the two hemispheres
- Basal ganglia - subcortical nuclei involved in motor control (the caudate nucleus curves through all lobes)
- Limbic structures - hippocampus (memory), amygdala (emotion, fear), fornix (connects hippocampus to hypothalamus)
The corpus callosum is particularly important: its surgical cutting (callosotomy) has revealed that the two hemispheres can function independently and have distinct specializations (split-brain research).
Cerebrum vs. Other Brain Parts
| Structure | Location | Key Role |
|---|---|---|
| Cerebrum | Uppermost/largest | Consciousness, thought, voluntary action, sensation |
| Cerebellum | Posterior, behind brainstem | Movement coordination and balance |
| Brainstem | Stalk of brain | Vital functions (breathing, consciousness, temperature control) |
Damage to the cerebrum or cerebellum can be survived; brainstem damage is usually fatal.
For a visual walkthrough of the cerebral cortex and its lobes, this lecture is a great resource:
knee joint from human anatomy bd chaurasia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete, well-illustrated account of the Knee Joint from Gray's Anatomy for Students - the standard equivalent to BD Chaurasia in coverage and style.
Note: BD Chaurasia's Human Anatomy is not available in the library. The content below is from Gray's Anatomy for Students, which covers the same topics with the same depth and is widely used alongside Chaurasia.
Knee Joint
Type and Overview
The knee joint is the largest synovial joint in the body. It consists of two articulations within a single joint cavity:
- Femorotibial articulation - between the femoral condyles and tibial condyles (weight-bearing)
- Patellofemoral articulation - between the patella and the patellar surface of the femur (redirects quadriceps pull)
Functionally, it is primarily a hinge joint allowing flexion and extension, with a small degree of rotation.
Articular Surfaces
Covered by hyaline cartilage:
- Two femoral condyles - curved/round posteriorly (articulate in flexion); flat inferiorly (articulate in full extension)
- Superior tibial condyles (tibial plateau)
- Patella - articulates with the V-shaped trench on the anterior distal femur
All surfaces share a single articular cavity.
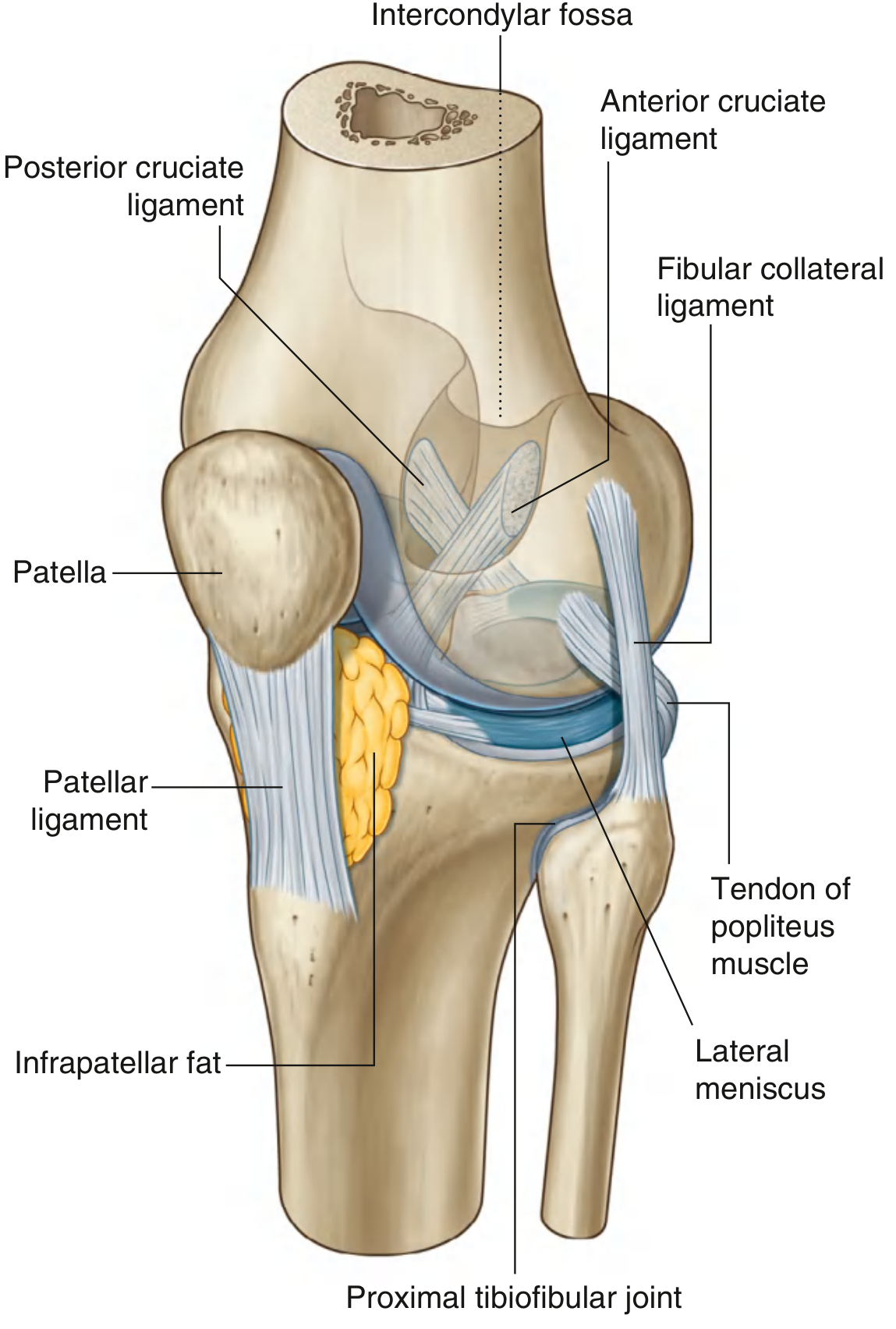
Fig. 6.73 - Knee Joint (anterior view, capsule not shown)
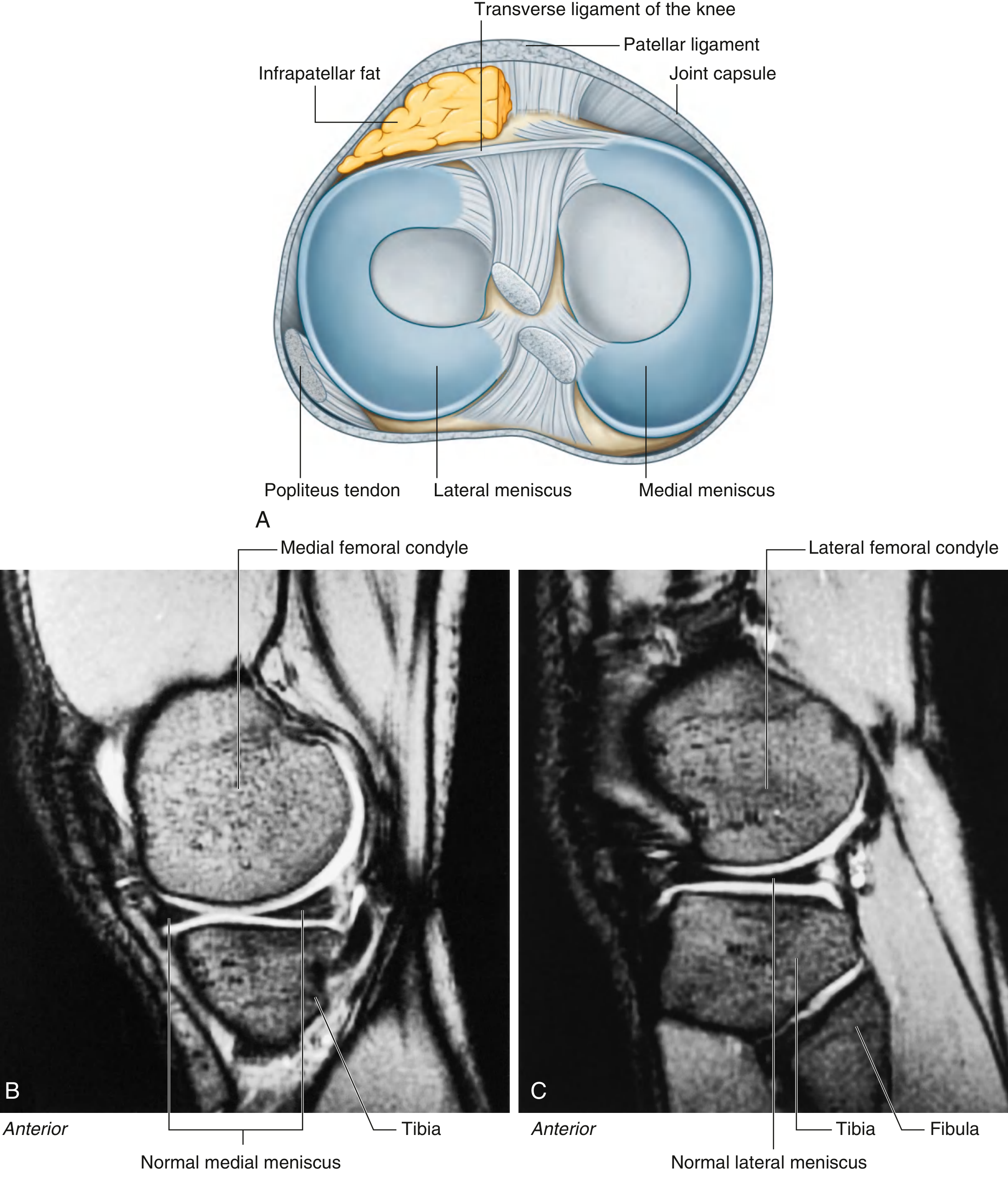
Menisci
Two C-shaped fibrocartilaginous discs sit between the femoral and tibial condyles:
| Medial Meniscus | Lateral Meniscus | |
|---|---|---|
| Shape | Larger C-shape | Smaller, more circular |
| Capsule attachment | Firmly attached | Not attached (more mobile) |
| Collateral ligament | Fused to tibial collateral ligament | Separate from fibular collateral ligament |
| Extra connections | - | Connected to popliteus tendon |
- Both are joined anteriorly by the transverse ligament of the knee
- The menisci improve congruency between femoral and tibial surfaces as joint shape changes from flexion (curved surfaces) to extension (flat surfaces)
Fig. 6.75 - Menisci (superior view + MRI)
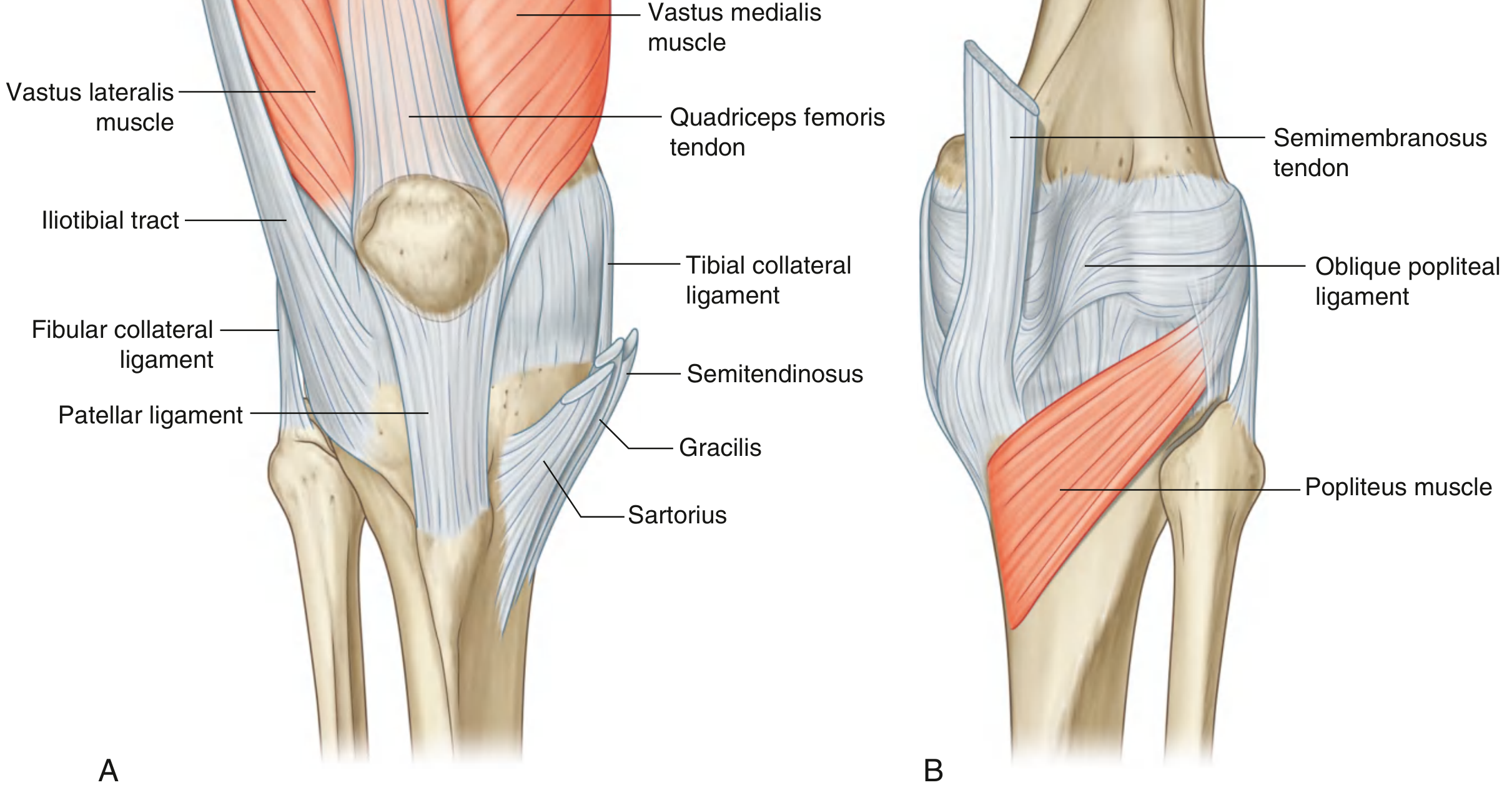
Fibrous Membrane (Joint Capsule)
- On the medial side: blends with and is attached to the tibial collateral ligament and medial meniscus
- On the lateral side: separated from the fibular collateral ligament by a bursa; not attached to the lateral meniscus
- Anteriorly: attached to patella margins, reinforced by expansions from vastus lateralis and medialis
- Anterolaterally: reinforced by the iliotibial tract
- Posteromedially: reinforced by the oblique popliteal ligament (from semimembranosus tendon)
Fig. 6.78 - Fibrous Membrane (anterior and posterior views)
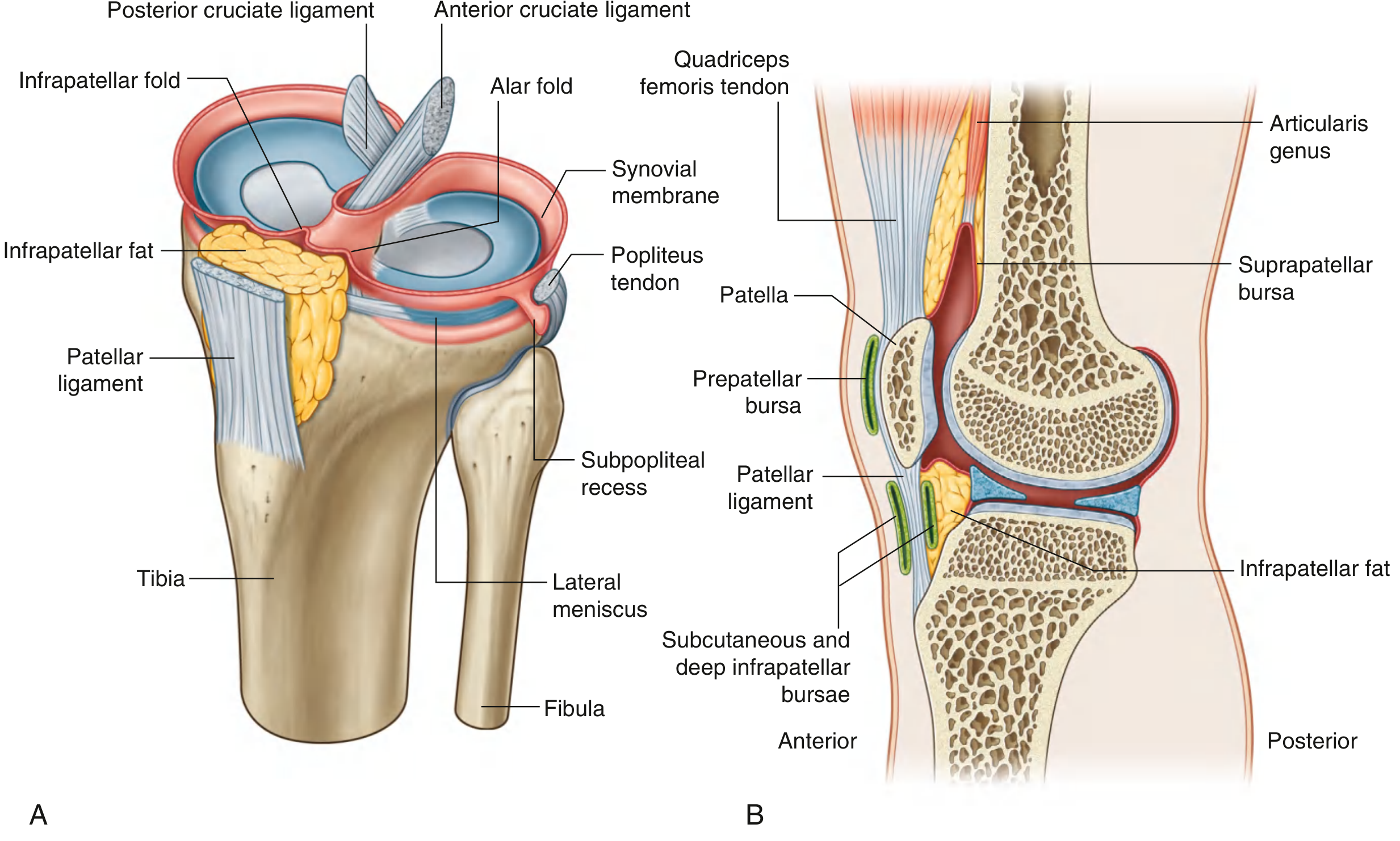
Synovial Membrane and Bursae
The synovial membrane lines the fibrous capsule and attaches to the meniscal margins. The cruciate ligaments lie outside the articular cavity but inside the fibrous capsule.
Key pouches and bursae:
| Bursa/Pouch | Location | Communication with joint |
|---|---|---|
| Suprapatellar bursa | Between distal femur and quadriceps tendon | Yes (communicates freely) |
| Subpopliteal recess | Posterolateral, between lateral meniscus and popliteus tendon | Yes |
| Prepatellar bursa | Subcutaneous, anterior to patella | No |
| Deep infrapatellar bursa | Deep to patellar ligament | No |
| Subcutaneous infrapatellar bursa | Superficial to patellar ligament | No |
The infrapatellar fat pad separates the patellar ligament from the synovial membrane anteriorly. Alar folds and the infrapatellar synovial fold project into the joint cavity.
Fig. 6.77 - Synovial Membrane and Bursae
Ligaments
1. Patellar Ligament
- Continuation of the quadriceps femoris tendon below the patella
- Attaches: apex/margins of patella → tibial tuberosity
2. Collateral Ligaments
Fibular (lateral) collateral ligament:
- Cord-like; separated from capsule by a bursa
- Attaches: lateral femoral epicondyle → lateral surface of fibular head
- Injured by varus force
Tibial (medial) collateral ligament:
- Broad and flat; fused to capsule and medial meniscus
- Attaches: medial femoral epicondyle → medial surface of tibia
- Injured by valgus force; part of the "unhappy triad" (with medial meniscus + ACL tears)
3. Cruciate Ligaments
Named because they cross each other in the sagittal plane:
| ACL | PCL | |
|---|---|---|
| Tibial attachment | Anterior intercondylar area | Posterior intercondylar area |
| Femoral attachment | Back of lateral condyle (intercondylar fossa) | Medial wall of intercondylar fossa |
| Function | Prevents anterior tibial displacement | Prevents posterior tibial displacement |
Locking Mechanism
When standing, the knee "locks" to save muscle energy:
- Shape change: As the knee extends, the femoral condyle surfaces shift from small curved areas (in flexion) to large flat areas (in extension) - increasing joint stability
- Medial rotation of femur: During the final degrees of extension, the femur rotates medially on the tibia, tightening all ligaments
- Center of gravity: Passes anterior to the knee joint, maintaining passive extension
Unlocking: The popliteus muscle initiates lateral rotation of the femur on the tibia to "unlock" the knee at the start of flexion.
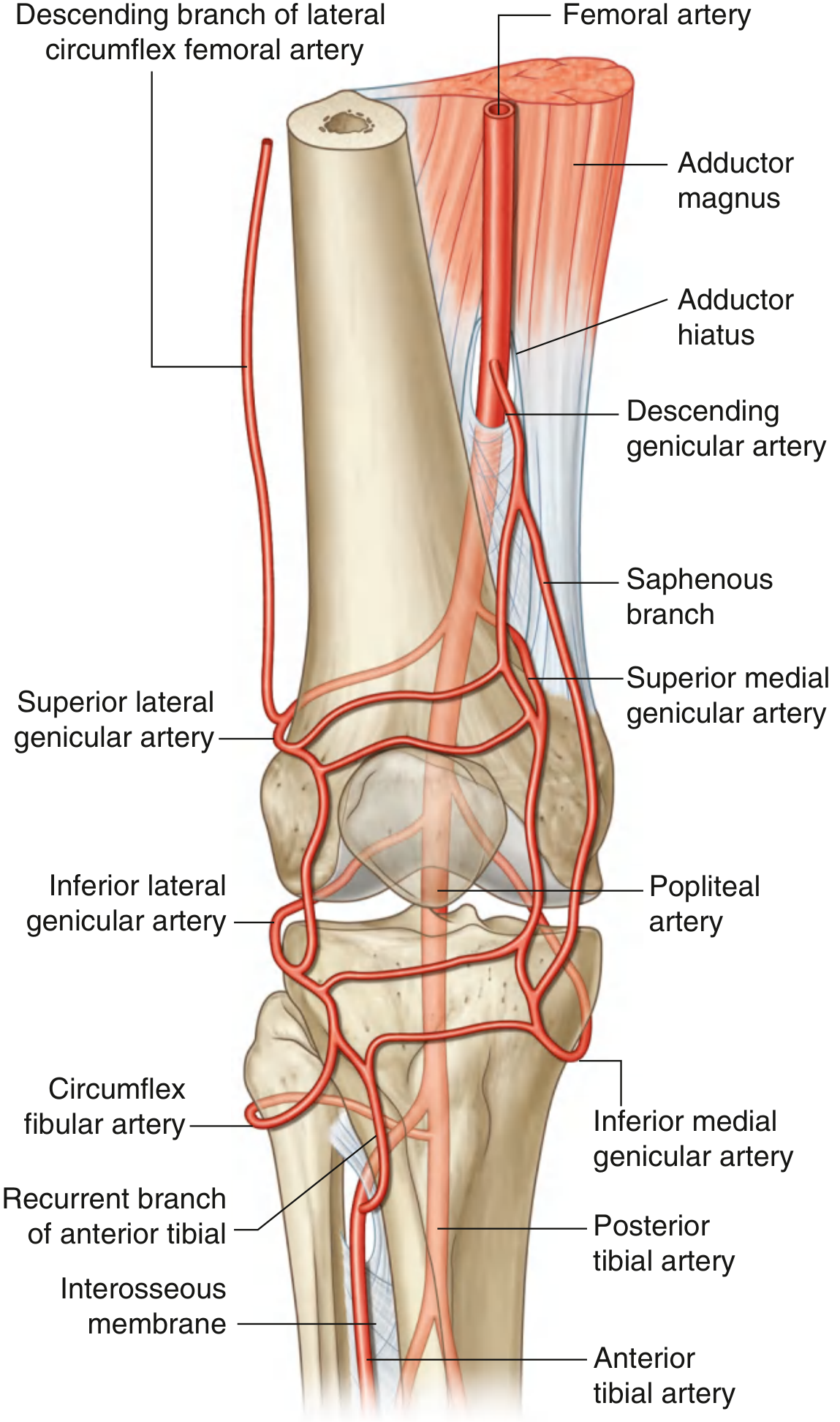
Vascular Supply
An anastomotic network around the knee is formed by:
- Descending genicular artery (from femoral artery)
- Superior and inferior medial/lateral genicular arteries (from popliteal artery)
- Circumflex fibular artery
- Recurrent branches of the anterior tibial artery
Fig. 6.82 - Arterial Anastomoses Around the Knee
Innervation
Branches from four nerves:
- Obturator nerve
- Femoral nerve
- Tibial nerve
- Common fibular (peroneal) nerve
Clinical Notes
Meniscal tears: Caused by forceful rotation/twisting. Patterns include vertical, horizontal, and bucket-handle tears. MRI is the investigation of choice. Arthroscopy is used for repair or debridement.
Unhappy triad (O'Donoghue's triad): Valgus force tears the tibial collateral ligament + medial meniscus + ACL simultaneously.
Collateral ligament injuries: Graded from sprains (fibers stretched) to full-thickness tears (all fibers torn, joint unstable).
Source: Gray's Anatomy for Students, pp. 709-717
hip joint
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete, illustrated account of the Hip Joint from Gray's Anatomy for Students.
Hip Joint
Type and Overview
The hip joint is a multiaxial ball-and-socket synovial joint between the head of the femur and the acetabulum of the pelvic bone. It is designed primarily for stability and weight-bearing, sacrificing some mobility compared to the shoulder joint.
Movements possible: flexion, extension, abduction, adduction, medial rotation, lateral rotation, and circumduction.
Fig. 6.30 - Articular Surfaces and Rotation
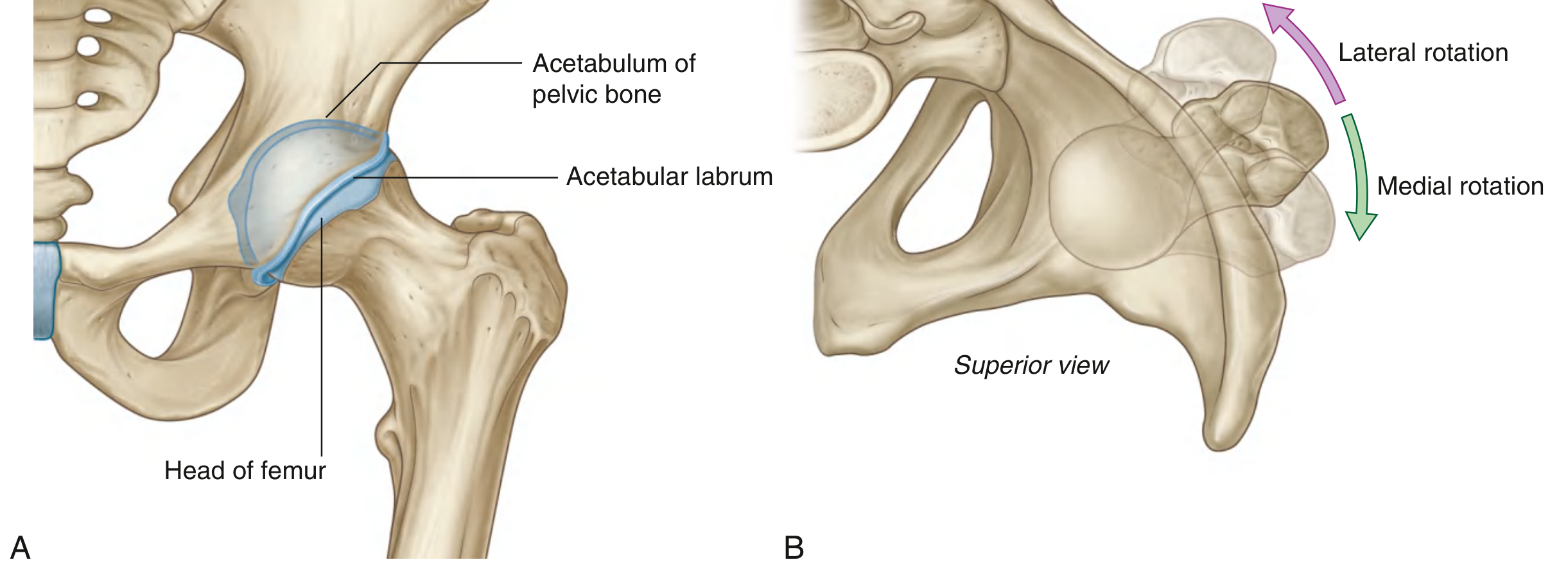
Articular Surfaces
| Structure | Detail |
|---|---|
| Head of femur | Spherical; covered entirely by hyaline cartilage except at the fovea |
| Acetabulum | Lunate (C-shaped) articular surface; covered by hyaline cartilage; broadest superiorly |
| Acetabular fossa | Non-articular central depression; contains loose connective tissue |
The acetabulum almost entirely encompasses the femoral head, which is the primary source of hip joint stability.
Acetabular Labrum and Transverse Ligament
- The rim of the acetabulum is deepened by a fibrocartilaginous collar - the acetabular labrum - which increases the depth of the socket
- Inferiorly, the labrum bridges the acetabular notch as the transverse acetabular ligament, converting the notch into a foramen
Fig. 6.31 - Transverse Acetabular Ligament & Ligament of the Head
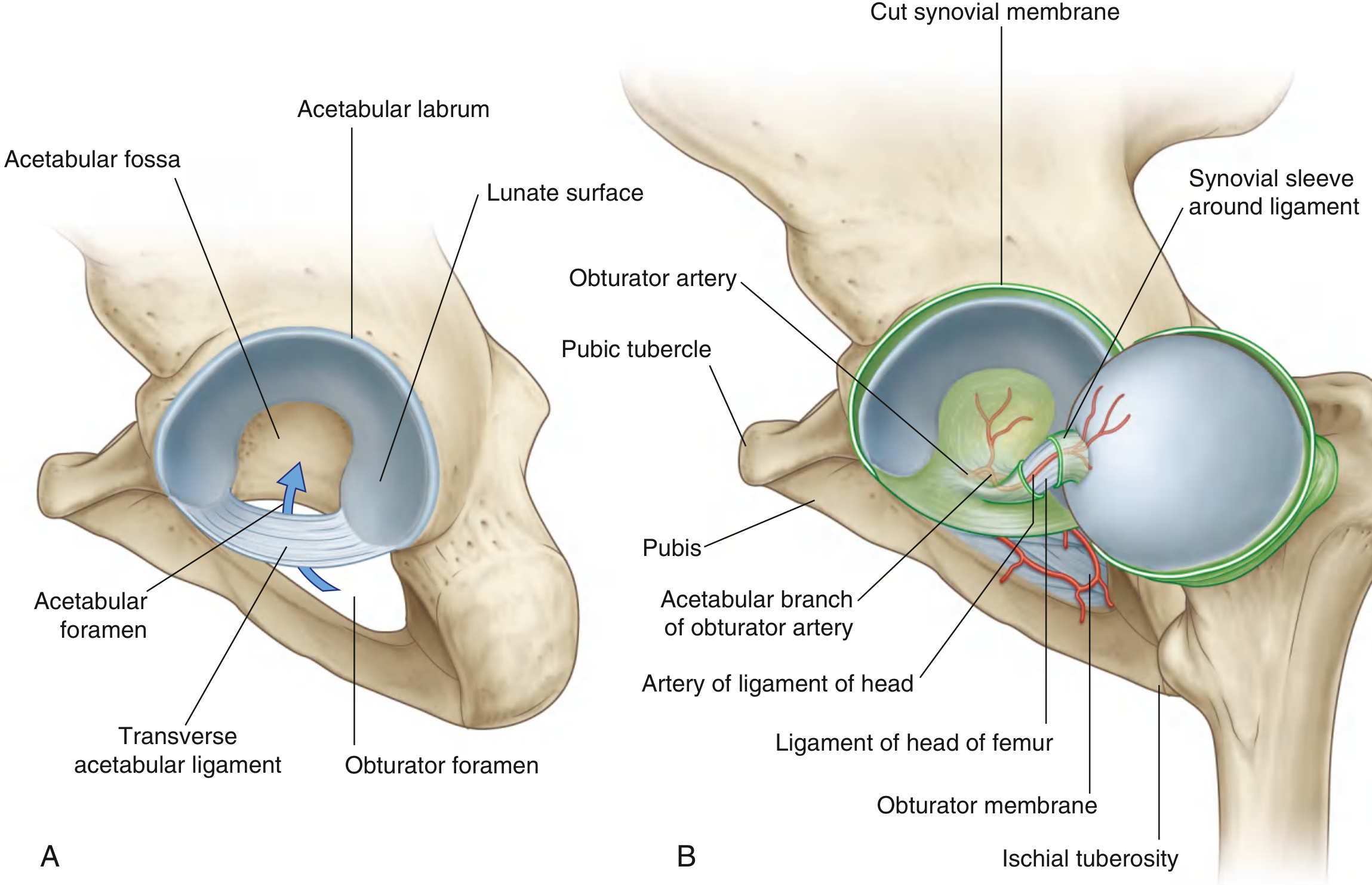
Ligament of the Head of the Femur (Ligamentum Teres)
- A flat band of delicate connective tissue
- Attaches: fovea on the head of the femur → acetabular fossa, transverse acetabular ligament, and margins of the acetabular notch
- Carries a small branch of the obturator artery - the artery of the ligament of the head - which contributes to the blood supply of the femoral head (clinically important in fracture-dislocations)
Fibrous Membrane (Joint Capsule)
Strong, generally thick capsule:
- Medially: attached to the margin of the acetabulum, transverse acetabular ligament, and adjacent margin of the obturator foramen
- Laterally (anterior): attached to the intertrochanteric line of the femur
- Laterally (posterior): attached to the femoral neck, just proximal to the intertrochanteric crest
This means the entire femoral neck is intracapsular anteriorly, but only the proximal part of the neck is intracapsular posteriorly. This is why femoral neck fractures disrupt the blood supply to the femoral head.
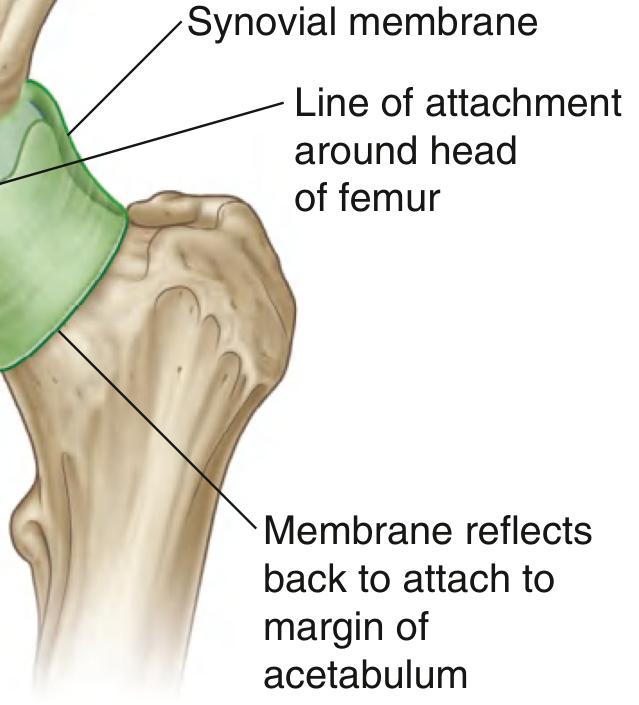
Synovial Membrane
- Lines the fibrous capsule from acetabular margin to the articular cartilage of the femoral head
- Reflects back along the femoral neck as retinacula (carrying blood vessels to the head)
- Covers the ligament of the head with a synovial sleeve
Fig. 6.32 - Synovial Membrane
Ligaments (Extracapsular)
Three ligaments reinforce the external surface of the fibrous capsule. All have spirally oriented fibers that become taut in extension, stabilizing the standing position with minimal muscle effort.
Fig. 6.33 - Ligaments of the Hip Joint
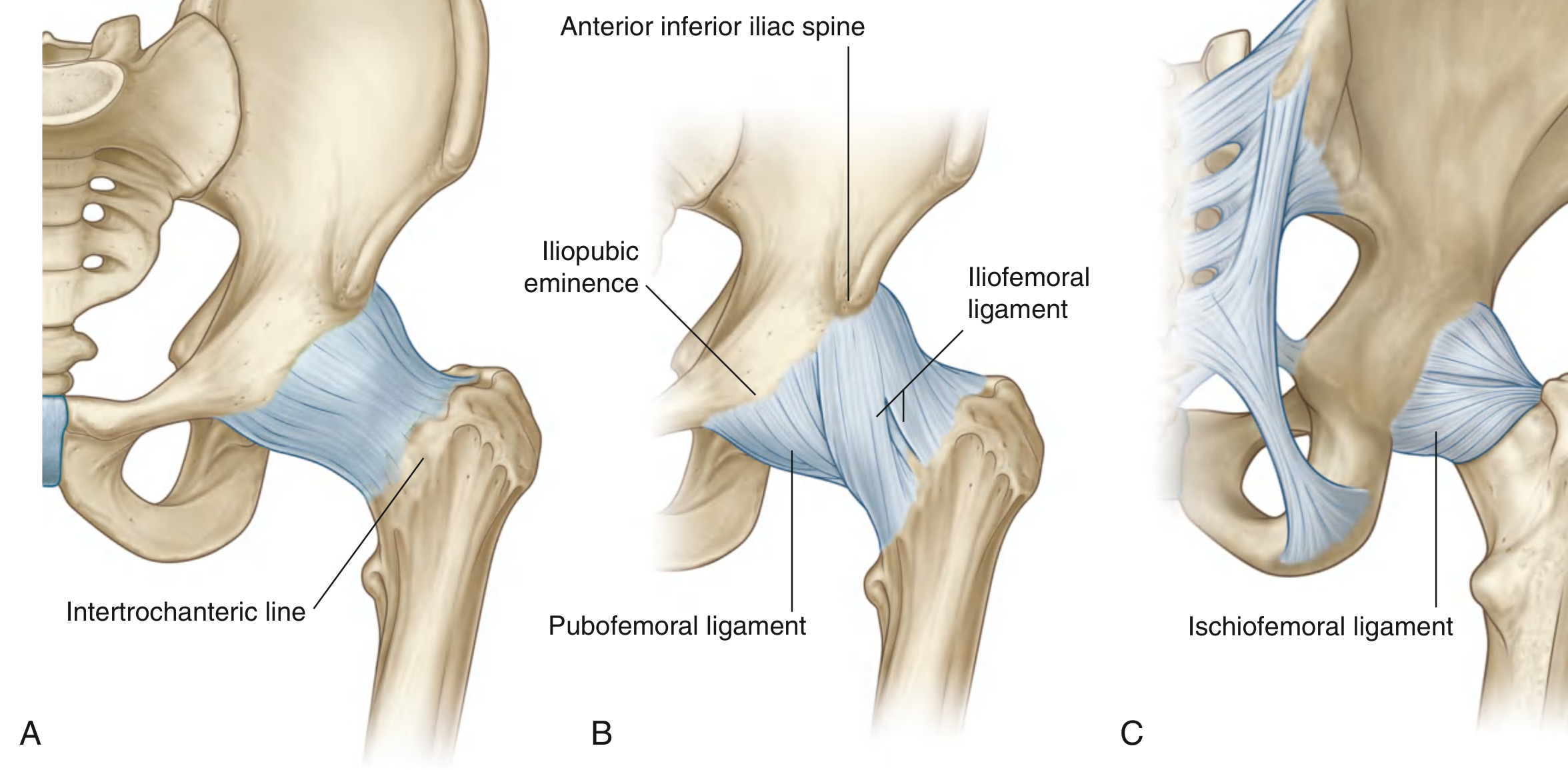
| Ligament | Position | Attachments | Shape/Note |
|---|---|---|---|
| Iliofemoral | Anterior | AIIS + acetabular margin → intertrochanteric line | Y-shaped (inverted Y); strongest ligament in the body |
| Pubofemoral | Anteroinferior | Iliopubic eminence + obturator membrane → blends with iliofemoral ligament | Triangular |
| Ischiofemoral | Posterior | Ischium (posteroinferior to acetabulum) → greater trochanter | Reinforces posterior capsule |
All three become taut in extension - locking the hip when standing upright.
Vascular Supply
An anastomotic arterial network around the joint is formed by:
- Medial circumflex femoral artery (dominant supply to femoral head - travels along the posterior femoral neck)
- Lateral circumflex femoral artery
- Obturator artery (acetabular branch → artery of ligament of head)
- Superior and inferior gluteal arteries
- 1st perforating branch of the deep artery of the thigh
Fig. 6.34 - Blood Supply of the Hip Joint
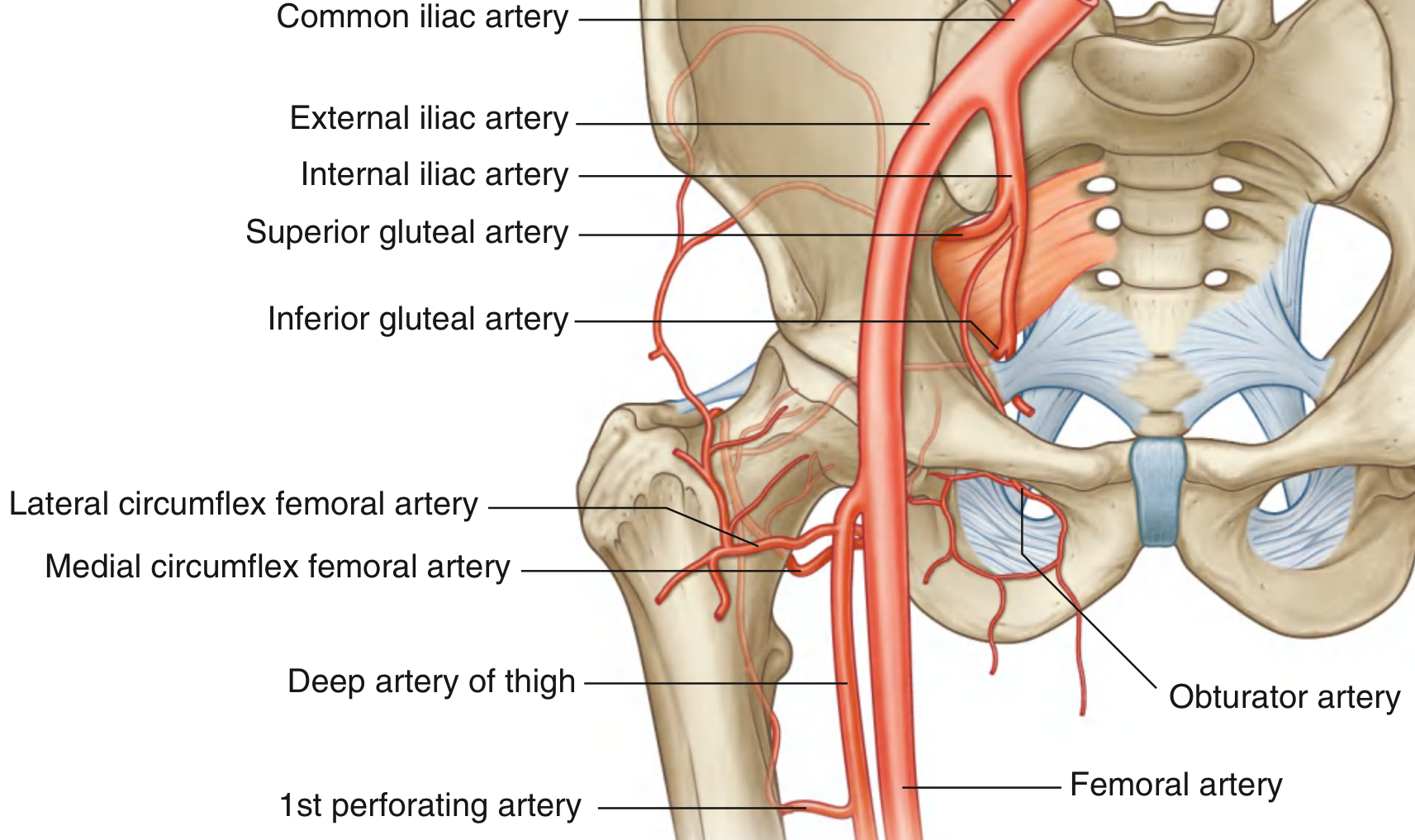
Clinical point: The medial circumflex femoral artery is the most important contributor to the blood supply of the femoral head. It travels along the posterior femoral neck and is at risk in posterior hip dislocations and intracapsular femoral neck fractures, leading to avascular necrosis (AVN) of the femoral head.
Innervation
The hip joint receives branches from:
- Femoral nerve
- Obturator nerve
- Superior gluteal nerve
- Nerve to quadratus femoris
(Hilton's Law: the joint is supplied by the same nerves that supply the muscles acting over it.)
Movements and Muscles
| Movement | Prime Movers |
|---|---|
| Flexion | Iliopsoas, rectus femoris, sartorius, tensor fasciae latae |
| Extension | Gluteus maximus, hamstrings |
| Abduction | Gluteus medius and minimus |
| Adduction | Adductor longus, brevis, magnus; gracilis |
| Medial rotation | Gluteus medius/minimus (anterior fibers), TFL |
| Lateral rotation | Obturator internus/externus, gemelli, piriformis, quadratus femoris |
Stability of the Hip Joint
The hip is far more stable than the shoulder due to:
- Deep acetabular socket - deepened further by the labrum
- Strong, thick capsule reinforced by three powerful ligaments
- Spiral ligament arrangement - tightens in extension (most common standing position)
- Surrounding musculature - particularly the gluteal muscles and iliopsoas
- Body weight - the center of gravity helps compress the joint
Source: Gray's Anatomy for Students, pp. 661-664
Ventricle
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.