Diagram of atrial fibrillation
Reading File
Finding Sources
Searching the Web
atrial fibrillation ECG diagram mechanism labeled
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Reading File
I now have all the key diagrams and textbook content needed. Here is a complete, well-illustrated explanation:
Atrial Fibrillation - Diagrams and Mechanism
How AF Starts and How It Looks on ECG
The diagram below from Nature Reviews Disease Primers is the clearest overview - it shows both the cardiac anatomy and the corresponding ECG changes, from normal sinus rhythm through to full AF:
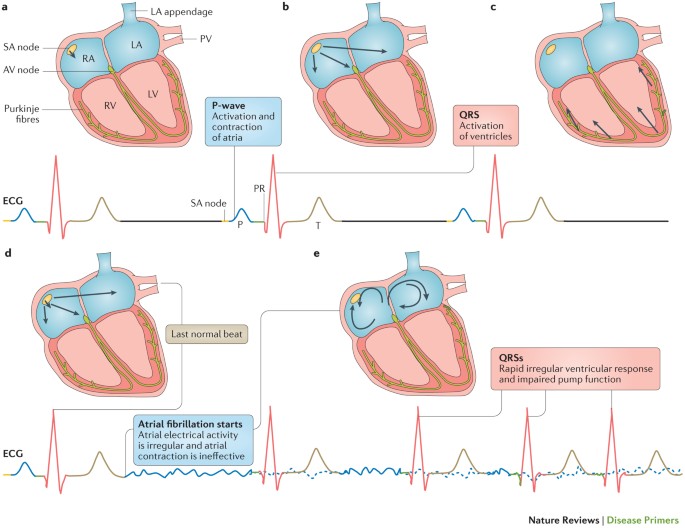
Reading the diagram panel by panel:
- Panel a - Normal cardiac anatomy: SA node triggers an orderly impulse down the AV node to Purkinje fibres (LA = left atrium, RA = right atrium, LV = left ventricle, RV = right ventricle, PV = pulmonary veins)
- Panel b - Normal ECG: organized P wave (atrial contraction) followed by a QRS complex
- Panel c - Normal QRS: organized ventricular activation
- Panel d - AF starts: chaotic re-entrant circuits and/or rapidly firing foci (often from the pulmonary veins) cause disorganized atrial activity - the P wave disappears, replaced by irregular fibrillatory (f) waves
- Panel e - Established AF: the AV node is bombarded with 350-600 impulses/min, conducts unpredictably, producing rapid, irregularly irregular QRS complexes ("QRSs") and impaired pump function
ECG Appearance in AF
Figure 66.2 from Braunwald's Heart Disease - prominent fibrillatory (f) waves in V1 mimicking flutter, confirmed as AF by typical f waves in leads II and V1:
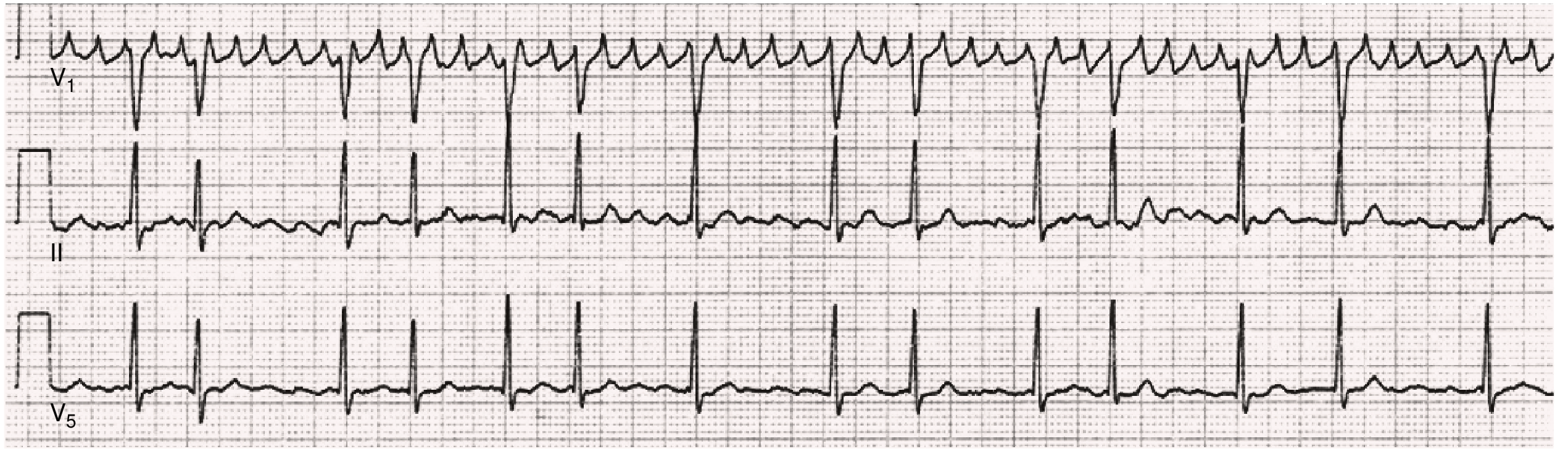
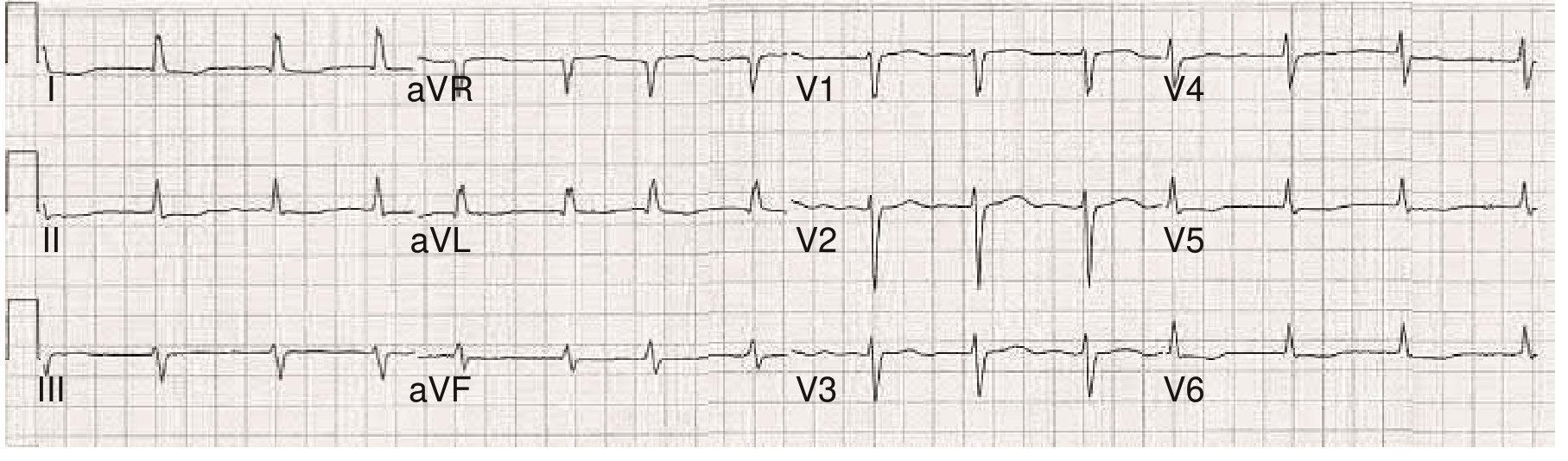
Figure 66.3 from Braunwald's Heart Disease - 12-lead ECG where no discrete f waves are visible, but the irregularly irregular ventricular rate establishes the diagnosis:
Three Key ECG Features of AF
| Feature | Normal Sinus Rhythm | Atrial Fibrillation |
|---|---|---|
| P waves | Present, upright, regular | Absent - replaced by chaotic f waves (350-600/min) |
| RR interval | Regular | Irregularly irregular |
| Ventricular rate | 60-100 bpm | Variable (often 100-160 bpm if uncontrolled) |
Mechanisms (from Braunwald's Heart Disease, p. 522)
Three main mechanistic concepts underlie AF:
- Multiple reentrant wavelets - multiple simultaneous re-entry circuits in the atria, continuously recycling and sustaining chaos
- Rapidly discharging autonomic foci - ectopic firing foci, most commonly in the pulmonary veins, trigger and maintain AF (especially paroxysmal AF)
- Single reentrant circuit with fibrillatory conduction - a "mother rotor" drives multiple daughter wavelets across the atria
In persistent AF, atrial remodeling (including interstitial fibrosis and conduction abnormalities) provides the substrate that maintains the arrhythmia beyond the initial trigger.
Clinical Consequences
- The AV node acts as a gatekeeper, but still allows irregular, rapid ventricular responses
- Loss of atrial "kick" (active atrial contraction) reduces cardiac output by ~10-20%, which matters most in patients with stiff/hypertrophic ventricles
- Blood stasis in the left atrial appendage promotes thrombus formation, leading to AF's 5-fold increase in stroke risk
- CHA₂DS₂-VASc score guides anticoagulation decisions
Sources: Braunwald's Heart Disease (9780323722193), Chapter 66; Nature Reviews Disease Primers 2016
This is a shared conversation. Sign in to Orris to start your own chat.