Diseases of cornea
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have enough content for a comprehensive response. Let me compile everything.
Diseases of the Cornea
Based on Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
Overview and Classification
Corneal diseases can be broadly divided into:
- Infections (Keratitis) - bacterial, fungal, viral, protozoal, helminthic
- Corneal Ectasias - keratoconus, pellucid marginal degeneration
- Corneal Dystrophies - epithelial, Bowman layer, stromal, endothelial
- Corneal Degenerations - age-related and other
- Metabolic Keratopathies - drug-induced, systemic disease
- Immune-mediated / Hypersensitivity disorders
- Interstitial Keratitis
1. BACTERIAL KERATITIS
Pathogens
- Pseudomonas aeruginosa - Gram-negative; responsible for >60% of contact lens-related keratitis; typically aggressive
- Staphylococcus aureus - Gram-positive, coagulase-positive; presents with a focal, well-defined white or yellow-white infiltrate
- Streptococci (S. pyogenes, S. pneumoniae) - often aggressive
- Neisseria gonorrhoeae, C. diphtheriae, H. influenzae - can penetrate an intact epithelium
Risk Factors
- Contact lens wear (especially extended-wear soft lenses) - the most important risk factor
- Corneal trauma, including refractive surgery (LASIK)
- Ocular surface disease, dry eye
- Topical steroid use
- Systemic immunosuppression
Clinical Features
- Pain, photophobia, redness, discharge, reduced vision
- Stromal infiltrate with overlying epithelial defect
- Anterior chamber reaction, hypopyon in severe cases
- Pseudomonas: rapid progression, stromal lysis, ring infiltrate
- S. aureus: fairly well-demarcated yellow-white infiltrate
Management
- Corneal scraping for microscopy and culture before treatment
- Intensive topical fluoroquinolones (ciprofloxacin or moxifloxacin) first-line
- Fortified antibiotics (vancomycin + ceftazidime/tobramycin) for severe cases
- Cycloplegia for pain and to prevent posterior synechiae
2. FUNGAL KERATITIS
Pathogens
- Yeasts (Candida) - predominant in temperate climates, immunocompromised hosts
- Filamentous fungi (Fusarium, Aspergillus) - predominant in tropical climates; often post-trauma with plant material
Predisposing Factors
Chronic ocular surface disease, long-term topical steroids, contact lens wear, systemic immunosuppression, diabetes, agricultural trauma
Clinical Features
Diagnosis is frequently delayed; often confused with bacterial keratitis.
- Gradual onset of pain, grittiness, photophobia, blurred vision
- Candida: dense, yellow-white suppurative infiltrate
- Filamentous: grey/yellow-white stromal infiltrate with indistinct fluffy margins, feathery branch-like extensions, satellite lesions
- Progressive necrosis and thinning
- Penetration of Descemet membrane can occur without frank perforation → endophthalmitis
Management
- Natamycin (5%) - first-line for filamentous fungi
- Voriconazole - broad-spectrum, good penetration
- Amphotericin B - for Candida and some filamentous
- Treatment often prolonged (weeks to months); penetrating keratoplasty may be required
3. HERPES SIMPLEX KERATITIS (HSK)
The leading infectious cause of corneal blindness in developed countries.
Epithelial (Dendritic) Keratitis
Active viral replication in corneal epithelium.
- Linear-branching (dendritic) ulcer with characteristic terminal buds staining with fluorescein
- Virus-laden marginal cells stain with rose Bengal
- Reduced corneal sensation
- Inadvertent topical steroid use causes enlargement to a geographic/amoeboid ulcer
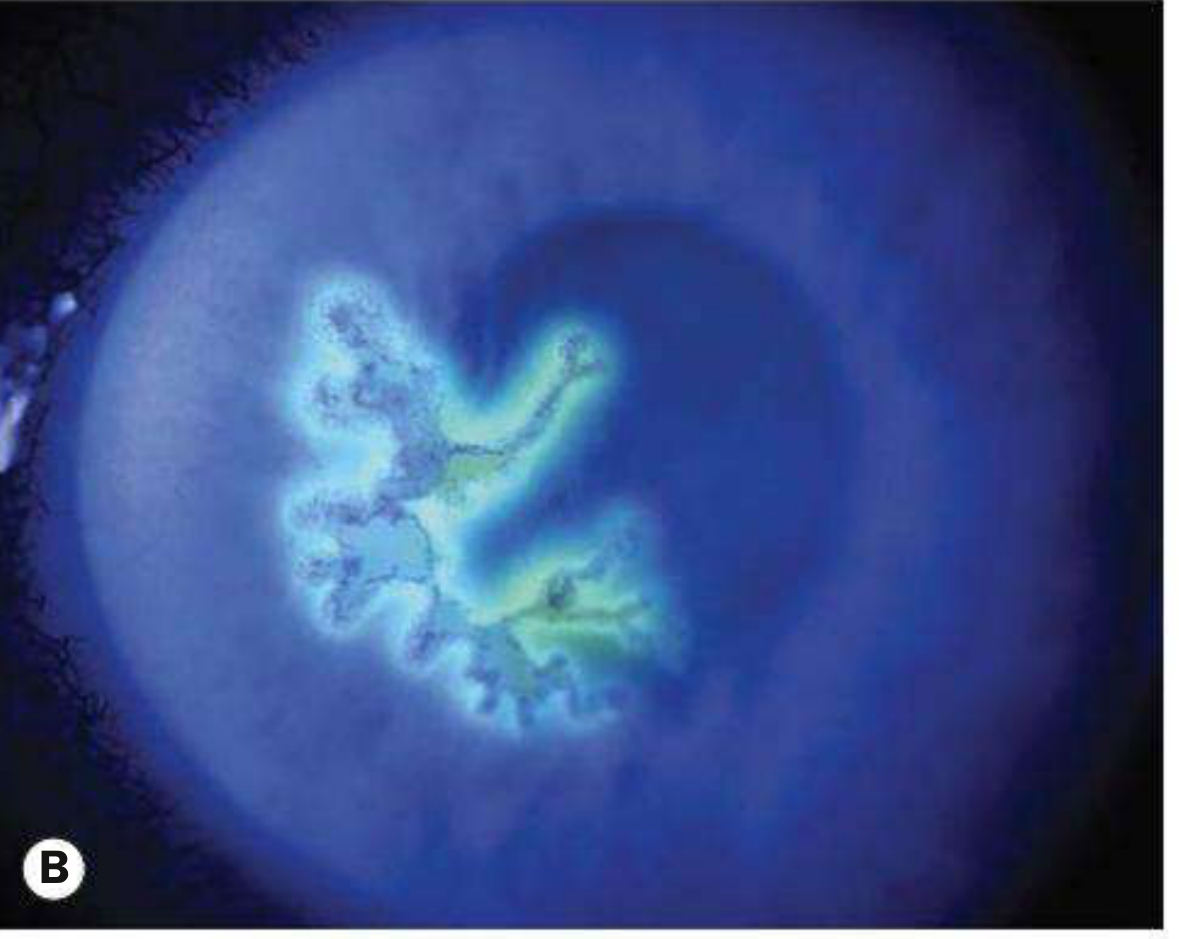
Fig: HSV epithelial keratitis - dendritic ulcer with fluorescein staining
Disciform (Stromal Immune) Keratitis
Immune-mediated stromal edema, not active viral replication.
- Central disc-shaped stromal edema with overlying epithelial bullae
- Descemet folds
- Reduced corneal sensation
- Mild anterior uveitis
Treatment
- Epithelial: topical aciclovir 3% ointment 5x/day for 10-14 days (or ganciclovir gel)
- Disciform: topical steroids + antiviral cover
- Long-term oral aciclovir/valaciclovir reduces recurrence frequency (HEDS trial)
4. ACANTHAMOEBA KERATITIS
Epidemiology
Acanthamoeba spp. are free-living protozoa found in soil, fresh/brackish water. Associated with contact lens wear and use of tap water for lens rinsing.
Clinical Features
- Pain often disproportionately severe relative to clinical signs (pathognomonic clue)
- Early: irregular, greyish epithelial surface; pseudodendrites (mimics HSV)
- Radial keratoneuritis (perineural infiltrates) - virtually pathognomonic
- Ring abscess formation (late stage)
- Scleritis (reactive)
- Often misdiagnosed initially as herpes simplex keratitis
Investigations
- Calcofluor white or PAS staining of scrapings (detects cysts)
- Non-nutrient agar seeded with dead E. coli for culture
- In vivo confocal microscopy
- PCR
Treatment
- Polyhexamethylene biguanide (PHMB) + propamidine isethionate (Brolene) - first-line
- Chlorhexidine as alternative
- Avoid steroids before commencing specific treatment
- Treatment is prolonged (6+ months)
5. INTERSTITIAL KERATITIS (IK)
Inflammation of the corneal stroma without primary epithelial or endothelial involvement; usually immune-mediated.
Causes: Syphilis (prototype), HSV, VZV, tuberculosis, Lyme disease, sarcoidosis, Cogan syndrome
Syphilitic IK
- Usually due to congenital syphilis; presents between ages 5-25 years
- Bilateral in 80% (but usually not simultaneous)
- Deep stromal vascularization giving a "salmon patch" appearance
- Granulomatous anterior uveitis
- After months, cornea clears with ghost vessels (non-perfused vessels) remaining
- Associated systemic signs: Hutchinson teeth, saddle-nose deformity, sensorineural deafness, sabre tibiae
Cogan Syndrome
- Non-syphilitic IK + audiovestibular dysfunction
- Associated with systemic vasculitis (up to 10% develop aortitis)
- Treatment: systemic steroids
6. CORNEAL ECTASIA
Keratoconus (KC)
A progressive disorder of central/paracentral corneal thinning with apical protrusion and irregular astigmatism.
- Prevalence: 0.1-0.2%; slightly more common in men
- Onset: typically teens to twenties
- Risk factors: eye rubbing, allergy, eczema, asthma
- Systemic associations: Down syndrome, Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta
Signs
- "Oil droplet" red reflex on ophthalmoscopy (classic sign)
- "Scissoring" retinoscopy reflex
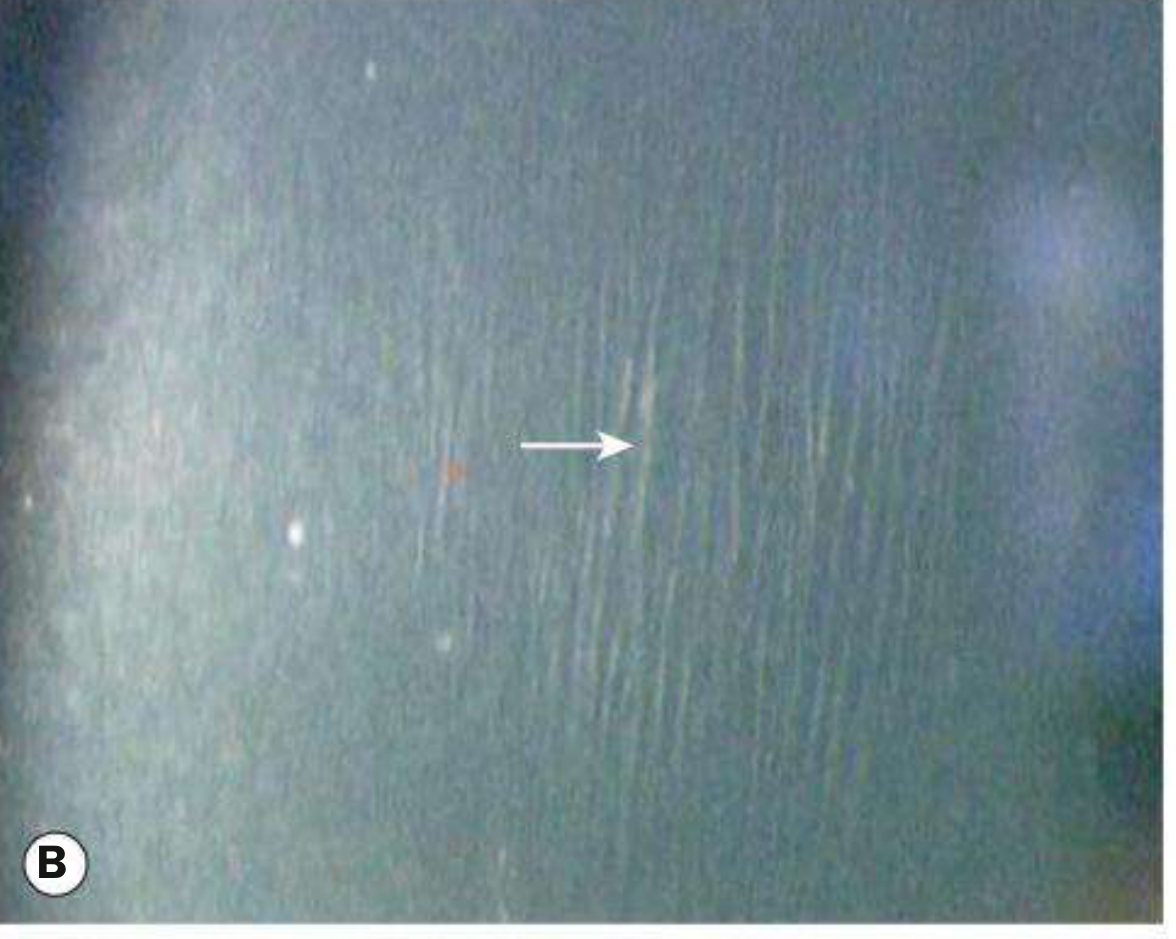
- Vogt striae: fine vertical stress lines in deep stroma
- Munson sign: V-shaped deformation of lower eyelid on downgaze
- Fleischer ring: iron deposition at base of cone (Perl's stain)
- Corneal thinning and protrusion
- Acute hydrops: sudden Descemet rupture → corneal edema → spontaneously resolves over 3 months

Fig: Keratoconus - oil droplet red reflex on ophthalmoscopy
Grading
- Mild: <48 D, Moderate: 48-54 D, Severe: >54 D (corneal power on keratometry)
Management
| Stage | Management |
|---|---|
| Early | Spectacles or soft contact lenses |
| Moderate | Rigid gas-permeable (RGP) lenses |
| Progressive | Corneal collagen crosslinking (CXL) to halt progression |
| Advanced | Intrastromal corneal ring segments (ICRS), penetrating keratoplasty |
7. CORNEAL DYSTROPHIES
Bilateral, hereditary, primary corneal disorders; classified by anatomical layer affected.
General rule: most dystrophies are bilateral, affect primarily one layer, and are slowly progressive.
A. Epithelial Dystrophies
Cogan (Epithelial Basement Membrane) Dystrophy
- Usually sporadic (degenerative); rare AD familial cases
- Thickening of basement membrane; deficient hemidesmosomes
- Classic "map-dot-fingerprint" pattern
- ~10% develop recurrent corneal erosions
- Treatment: lubricants, hypertonic saline, PTK (phototherapeutic keratectomy)
Meesmann Epithelial Dystrophy
- Rare, AD; mutations in corneal epithelial keratin genes
- Myriad tiny intraepithelial cysts of uniform size, maximal centrally
- Usually mild symptoms; recurrent erosions possible
B. Bowman Layer / Anterior Stromal Dystrophies
Reis-Bücklers Dystrophy (CBD1)
- AD; gene TGFB1
- Histology: replacement of Bowman layer by connective tissue
- Grey-white geographic subepithelial opacities, denser centrally
- Severe recurrent erosions in childhood; visual impairment with age
Thiel-Behnke Dystrophy (CBD2)
- AD; gene TGFB1 and others
- "Curly fibres" on electron microscopy
- Honeycomb-like subepithelial opacities
- Less severe than Reis-Bücklers
C. Stromal Dystrophies
Lattice Corneal Dystrophy (TGFB1 type)
- AD; gene TGFB1
- Histology: amyloid deposits staining with Congo red; green birefringence with polarizing filter
- Recurrent erosions + progressive visual deterioration
- Signs: fine linear branching opacities in anterior stroma, with intervening haze; clear peripheral zone
- Treatment: PTK; penetrating keratoplasty in advanced cases; recurrence in grafts common
Granular Corneal Dystrophy (GCD type 1)
- AD; gene TGFB1
- Histology: hyaline deposits (Masson trichrome stain: red)
- Well-defined, discrete white granular opacities in anterior stroma, separated by clear intervals
- Superficial erosions may occur
Macular Corneal Dystrophy
- Autosomal recessive (unusual among dystrophies); gene CHST6
- Histology: glycosaminoglycan accumulation; stains with Alcian blue and colloidal iron
- Dense greyish-white spots in anterior stroma centrally; no clear zone between opacities
- Progression to full-thickness stroma; corneal thinning; worst visual prognosis among stromal dystrophies
- Treatment: penetrating keratoplasty (frequent recurrence)
Schnyder Corneal Dystrophy
- AD; gene UBIAD1
- Disorder of corneal lipid metabolism; phospholipid and cholesterol deposits
- Central haze, glare; corneal crystals (variable)
- Associated systemic dyslipidaemia in some patients
D. Endothelial Dystrophies
Fuchs Endothelial Dystrophy
- Most common endothelial dystrophy; usually sporadic; more common in women
- AD in familial cases
- Histology: guttae (excrescences of Descemet membrane), endothelial cell loss
- Early: bilateral guttae (cornea guttata), halos/glare, worse in morning
- Late: stromal and epithelial edema, painful bullous keratopathy, visual failure
- Treatment: DSEK/DMEK (Descemet membrane endothelial keratoplasty) preferred over penetrating keratoplasty
Congenital Hereditary Endothelial Dystrophy (CHED)
- AR (CHED2, gene SLC4A11); presents at birth or shortly after
- Diffuse ground-glass corneal clouding; nystagmus may develop
- Treatment: early keratoplasty
Posterior Polymorphous Dystrophy
- AD; usually asymptomatic
- Vesicular, band-like or diffuse endothelial lesions
- Rarely progresses to corneal edema
8. CORNEAL DEGENERATIONS
Age-Related Degenerations
Arcus Senilis (Gerontoxon)
- Most common peripheral corneal opacity
- Stromal lipid deposition in perilimbal cornea forming a white band ~1 mm wide; sharp peripheral edge, diffuse central border, clear zone between band and limbus
- In elderly, no systemic significance; in younger patients (arcus juvenilis) investigate for dyslipidaemia
Vogt Limbal Girdle
- Present in up to 60% of individuals >40 years
- Whitish crescentic bands at 3 and 9 o'clock; harmless
Cornea Farinata
- Bilateral minute flour-like deposits in deep stroma; visually insignificant
Other Degenerations
Band Keratopathy
- Calcium deposition in Bowman layer, progressing as a band across the interpalpebral zone
- Causes: chronic ocular inflammation (especially JIA-associated uveitis), hypercalcaemia, renal failure, sarcoidosis, chronic corneal disease
- Treatment: EDTA chelation under topical anaesthesia; PTK
Pterygium
- Triangular fibrovascular growth of conjunctival tissue encroaching onto cornea, usually nasally
- Risk factors: UV exposure, dry/dusty environments
- Treatment: surgical excision with conjunctival autograft (bare sclera technique has high recurrence)
Pinguicula
- Yellow-white deposits in bulbar conjunctiva at 3 and 9 o'clock; does not usually extend onto cornea
Pellucid Marginal Degeneration
- Inferior peripheral thinning without vascularization or inflammation
- Differentiated from keratoconus by inferior peripheral (not central/paracentral) location
- Treatment similar to keratoconus
Terrien Marginal Degeneration
- Bilateral, slowly progressive peripheral thinning; predominantly superior
- Non-inflammatory; vascularized
9. METABOLIC KERATOPATHY / DRUG-INDUCED
Vortex Keratopathy (Cornea Verticillata)
- Whorl-like golden-brown opacities in corneal epithelium below the pupil
- Causes: amiodarone (virtually all patients), antimalarials (chloroquine/hydroxychloroquine), Fabry disease, numerous other drugs
Chlorpromazine Keratopathy
- Yellowish-brown granular deposits in endothelium, Descemet membrane and deep stroma
Wilson Disease
- Kayser-Fleischer ring: golden-brown copper deposits in peripheral Descemet membrane; seen in hepatolenticular degeneration
10. IMMUNE / HYPERSENSITIVITY-MEDIATED DISEASE
Marginal Keratitis
- Bacterial (staphylococcal) hypersensitivity reaction
- Peripheral crescent-shaped infiltrates with a clear zone between infiltrate and limbus
- Distinct from bacterial keratitis (no organisms in infiltrate)
- Treatment: topical steroids ± antibiotics (for associated blepharitis)
Phlyctenulosis
- Nodular hypersensitivity reaction at limbus; associated with TB, staphylococcal antigen
- Leads to corneal vascularization if repeated
Mooren Ulcer
- Progressive painful peripheral ulceration; cause unknown (possibly autoimmune)
- Bilateral form is more common in Africa
- Treatment: aggressive immunosuppression; keratoplasty in severe cases
Summary Table: Key Differentiating Features
| Disease | Key Feature | Gene / Cause |
|---|---|---|
| Bacterial keratitis | Stromal infiltrate + epithelial defect | Pseudomonas (CL), Staph |
| Fungal keratitis | Fluffy margins, satellite lesions | Fusarium, Candida |
| HSV epithelial | Dendritic ulcer, terminal buds | HSV-1 |
| Acanthamoeba | Radial keratoneuritis, severe pain | Acanthamoeba spp. |
| Syphilitic IK | Salmon patch, ghost vessels | Treponema pallidum |
| Keratoconus | Oil droplet reflex, Vogt striae | Multifactorial |
| Lattice dystrophy | Amyloid (Congo red+) | TGFB1 |
| Granular dystrophy | Hyaline (trichrome red) | TGFB1 |
| Macular dystrophy | Glycosaminoglycans (Alcian blue+), AR | CHST6 |
| Fuchs dystrophy | Guttae, morning blur | SLC4A11/ZEB1 |
| Arcus senilis | Perilimbal lipid band, clear zone at limbus | Age/lipids |
| Band keratopathy | Calcium in Bowman, interpalpebral | Chronic inflammation, hypercalcaemia |
| Vortex keratopathy | Whorl pattern, epithelium | Amiodarone, Fabry |
Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
Give me notes on keratotoconus
Reading File
Searching PubMed
keratoconus management
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I have all the content needed. Here are comprehensive notes:
Keratoconus - Notes
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
Definition
Keratoconus (KC) is a progressive, non-inflammatory disorder characterized by:
- Central or paracentral corneal stromal thinning
- Apical protrusion (cone formation)
- Irregular astigmatism and progressive myopia
Epidemiology
- Prevalence: 0.1-0.2% of the population
- Slightly more common in males
- Typically presents in the teens or twenties
- Initially unilateral, but both eyes are eventually affected in almost all cases (at least on topography)
- ~50% of clinically normal fellow eyes progress to KC within 16 years
Genetics
- Most cases are sporadic (no family history)
- Only ~10% of offspring develop KC
- Autosomal dominant with incomplete penetrance has been proposed
Associations
Risk Factors
- Eye rubbing (persistent, from any cause) - modifiable and important
- Allergy, asthma, eczema
- Atopic disease (vernal keratoconjunctivitis - strong ocular association)
Systemic Associations
| Condition | Notes |
|---|---|
| Down syndrome | Most common systemic association |
| Ehlers-Danlos syndrome | Connective tissue disorder |
| Marfan syndrome | Connective tissue disorder |
| Osteogenesis imperfecta | Connective tissue disorder |
Ocular Associations
- Vernal keratoconjunctivitis
- Blue sclera
- Aniridia
- Leber congenital amaurosis
- Retinitis pigmentosa
Clinical Features
Symptoms
- Progressive, often initially unilateral blurring of vision
- Increasing myopia and astigmatism
- Monocular diplopia / ghost images
- Glare and haloes
- Difficulty with spectacle correction (frequently changing prescription)
- Occasionally first presents with acute hydrops
Signs
On Ophthalmoscopy
"Oil droplet" red reflex - a fairly well-delineated darker central area when viewed from ~0.5 m distance
On Retinoscopy
- Irregular "scissoring" reflex
On Slit-Lamp Biomicroscopy
1. Vogt striae
Fine, vertical stress lines in the deep stroma - disappear with gentle pressure on the globe
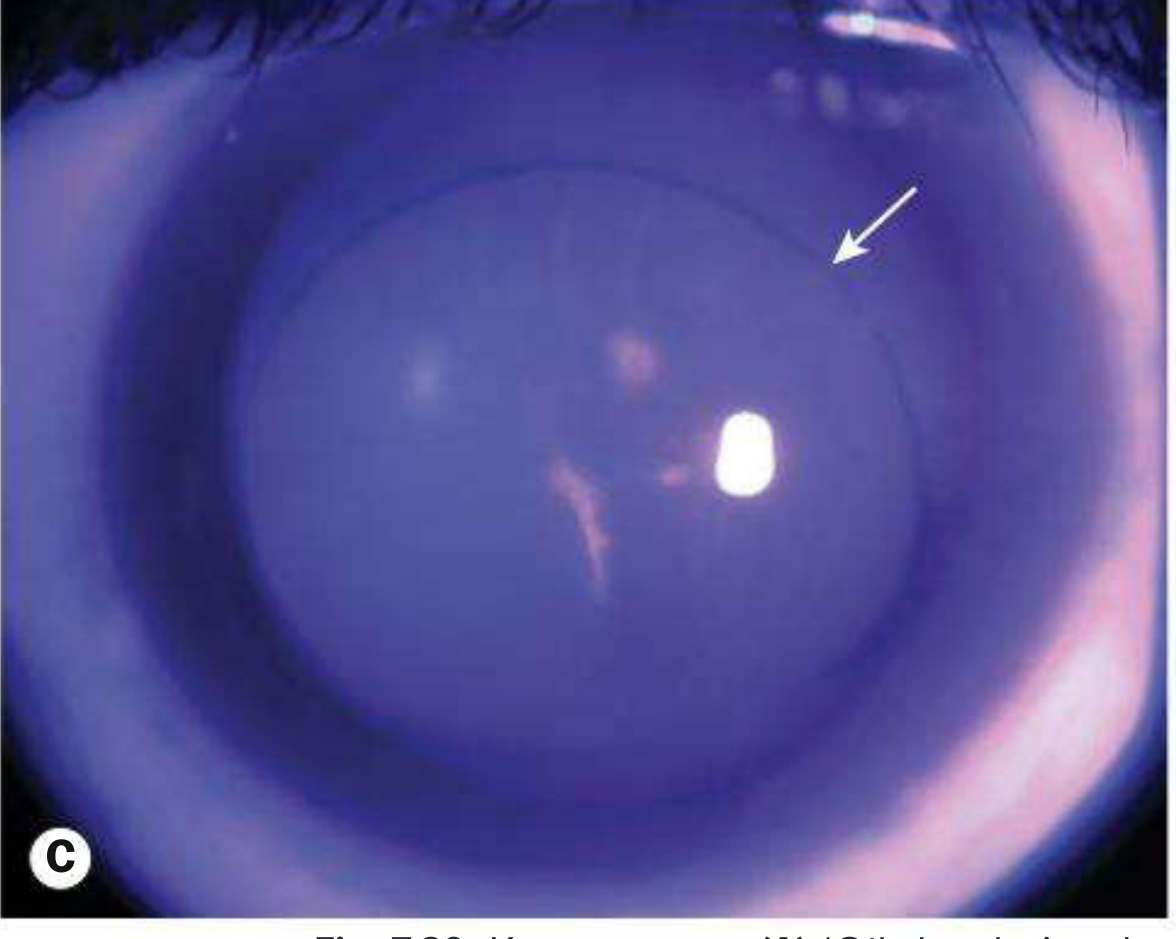
2. Fleischer ring
Epithelial iron deposits surrounding the base of the cone; best seen with cobalt blue filter
3. Corneal cone
Progressive protrusion in a cone configuration; thinning maximal at the apex
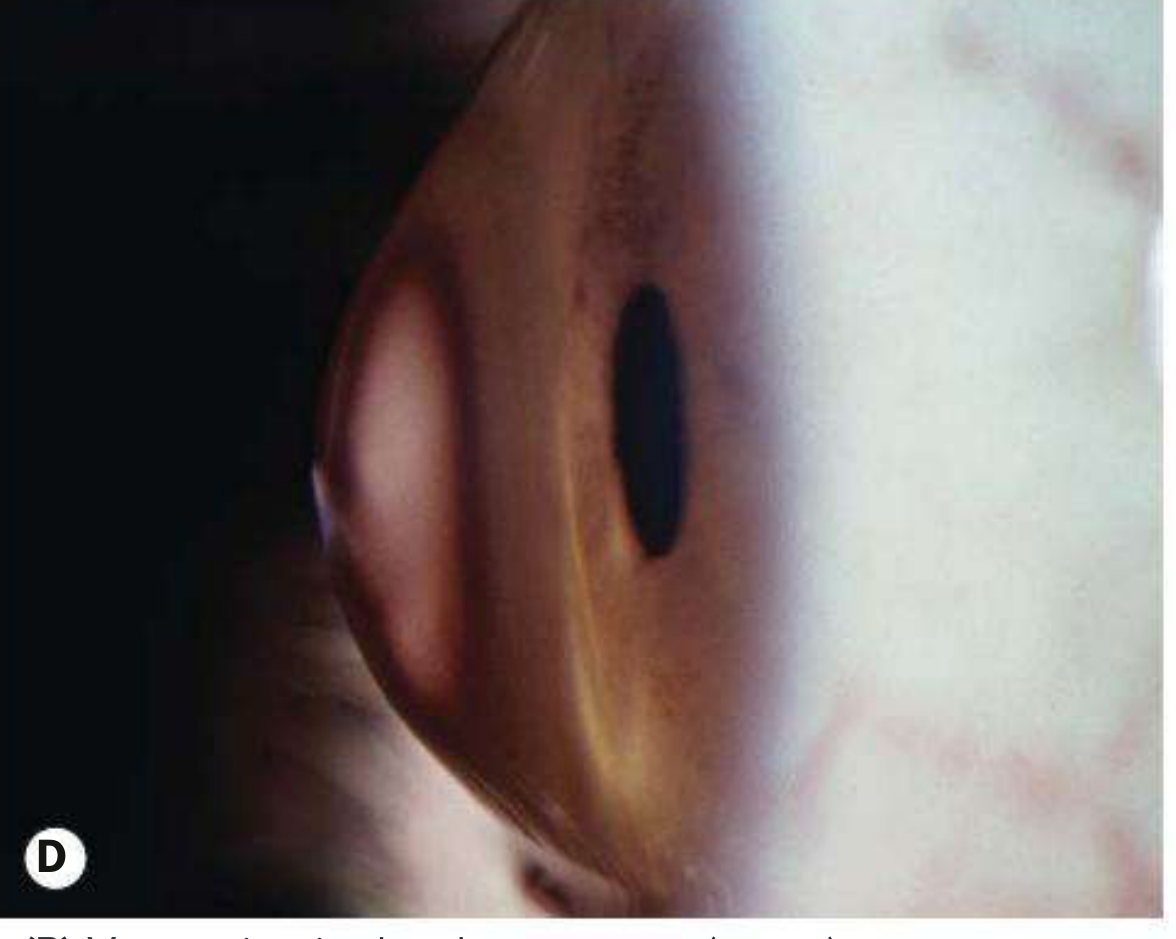
4. Munson sign
V-shaped deformation of the lower eyelid on downgaze - a late sign reflecting the degree of protrusion
5. Rizzuti sign
A bright conical beam of light on the nasal limbus when a pen-torch is shone from the temporal side
Acute Hydrops
A complication of keratoconus, not always a presentation.
- Mechanism: Sudden rupture in the stretched Descemet membrane → aqueous floods the stroma → acute corneal edema
- Symptoms: Sudden onset pain, photophobia, dramatically decreased vision, lacrimation
- Signs: Localized opaque area of stromal edema; may be sectoral or diffuse
- Resolution: Descemet break heals within 6-10 weeks; edema gradually clears
- Outcome: Variable stromal scarring; paradoxically, scarring can sometimes flatten the cone and improve VA
- Management:
- Cycloplegia
- Hypertonic saline (5%) ointment
- Soft bandage contact lens / patching
- Intracameral gas injection may accelerate resolution
Grading (by Maximum Keratometry)
| Grade | K reading |
|---|---|
| Mild | < 48 D |
| Moderate | 48-54 D |
| Severe | > 54 D |
Investigations
Corneal Topography / Tomography
- Most sensitive for detection and monitoring
- Corneal power maps show characteristic asymmetric astigmatism evolving from:
- Symmetrical bow-tie → 2. Asymmetrical bow-tie → 3. Inferotemporal displaced steep-sided cone
- Sometimes a central ('nipple') cone develops
Keratometry
- Steep readings, often asymmetric between eyes
Pachymetry
- Corneal thinning, especially at the apex
Contact lens warpage can mimic KC on topography, but typically shows a more arcuate-shaped pattern
Management
Treatment is stepwise based on severity and progression:
Step 1 - Optical Correction (Early)
- Spectacles - adequate in very early cases
- Soft contact lenses - for mild irregular astigmatism
Step 2 - Rigid Contact Lenses (Moderate)
- Rigid gas-permeable (RGP) lenses - vault over the irregular surface and provide a regular refracting surface
- Scleral lenses - for higher degrees of astigmatism / lens intolerance; large-diameter lenses that vault the entire cornea
Step 3 - Corneal Collagen Cross-Linking (CXL) - For Progressive Disease
- Mechanism: Riboflavin (vitamin B2) drops photosensitize the corneal stroma, then exposure to UV-A light (370 nm) creates new covalent bonds between collagen fibrils → stiffens the cornea
- Indication: Documented progression (steepening on topography, worsening VA, increasing refraction)
- Efficacy: Successful in >90% of cases at halting progression; some cases show flattening
- Standard (epithelium-off / Dresden) protocol: Epithelium removed; riboflavin 0.1% drops instilled for 30 min; UV-A 3 mW/cm² for 30 min
- Accelerated (epithelium-on) protocol: Epithelium retained; higher UV-A intensity - a 2025 meta-analysis (PMID: 40856685) found epithelium-off remains more effective for halting progression
- Minimum requirement: Corneal thickness ≥400 µm to avoid endothelial damage
Step 4 - Intrastromal Corneal Ring Segments (ICRS / Ferrara/Intacs rings)
- Inserted into mid-peripheral stroma via femtosecond laser channels
- Flatten and regularize the cornea
- May allow patients to resume contact lens wear
- Does not halt progression - often combined with CXL
Step 5 - Keratoplasty (Advanced)
- Indicated when contact lenses are no longer tolerable or vision cannot be corrected adequately
- Deep Anterior Lamellar Keratoplasty (DALK) - preferred where possible; replaces stroma while preserving host Descemet membrane + endothelium → avoids endothelial rejection risk
- Penetrating Keratoplasty (PK) - full-thickness graft; used when DALK is not feasible (e.g. post-hydrops scarring involving deep stroma/Descemet)
- Excellent long-term outcomes; graft rejection is the main concern with PK
Summary Diagram
KERATOCONUS
│
├── Pathology: Stromal thinning + cone protrusion + irregular astigmatism
│
├── Key Signs
│ ├── Oil droplet reflex (ophthalmoscopy)
│ ├── Scissoring reflex (retinoscopy)
│ ├── Vogt striae (slit lamp - deep stroma)
│ ├── Fleischer ring (slit lamp - cobalt blue)
│ └── Munson sign (downgaze)
│
├── Complication: Acute Hydrops
│ └── Descemet rupture → acute edema → resolves 6-10 wks
│
└── Management (stepwise)
├── Spectacles / soft lenses
├── RGP / scleral lenses
├── CXL (if progressing) - >90% effective
├── ICRS (rings)
└── DALK / PK (advanced)
Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed.
Recent evidence note: A 2025 meta-analysis (PMID: 40856685) comparing epithelium-on vs epithelium-off CXL confirms that the standard epithelium-off (Dresden) protocol remains superior in halting keratoconus progression, though epithelium-on has less discomfort and faster recovery.
This is a shared conversation. Sign in to Orris to start your own chat.