BMI , Types of bariatric surgeries Pre op evaluation , intra & post op management of morbid obese patient posted for bariatric surgery MD ANAESTHESIA PG EXAM detailed answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bariatric surgery" AND "anesthesia" AND "perioperative management"
Finding Sources
Finding Sources
Searching PubMed
"bariatric surgery" AND "perioperative" AND "complications"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative anesthesia and surgery textbooks. Let me compile a thorough, exam-quality answer.
Anaesthesia for Morbid Obesity and Bariatric Surgery
MD Anaesthesia PG Exam - Detailed Answer
SECTION 1: BODY MASS INDEX (BMI)
Definition
BMI (Body Mass / Quetelet Index) is the standard clinical tool to quantify obesity:
BMI = Body weight (kg) / Height² (m²)
WHO Classification of Obesity
| Classification | BMI (kg/m²) |
|---|---|
| Underweight | < 18.5 |
| Normal weight | 18.5 - 24.9 |
| Overweight | 25 - 29.9 |
| Class I Obesity | 30 - 34.9 |
| Class II Obesity | 35 - 39.9 |
| Class III / Morbid Obesity | ≥ 40 |
| Super Obesity | ≥ 50 |
| Super-Super Obesity | ≥ 60 |
Source: Barash Clinical Anesthesia 9e, Table 45-1; Fischer's Mastery of Surgery 8e, Table 2.10
Related Weight Concepts (Critical for Drug Dosing)
-
Ideal Body Weight (IBW) - Broca Index:
- Males: IBW (kg) = Height (cm) - 100
- Females: IBW (kg) = Height (cm) - 105
-
Predicted Body Weight (PBW):
- Males: PBW = 50 + 0.91 × (Height[cm] - 152.4)
- Females: PBW = 45.5 + 0.91 × (Height[cm] - 152.4)
-
Lean Body Weight (LBW):
- Males: 1.10 × TBW - 0.0128 × BMI × TBW
- Females: 1.07 × TBW - 0.0148 × BMI × TBW
- Approximation: IBW + 20-30% in morbidly obese
-
Total Body Weight (TBW): Actual measured weight
Metabolic Syndrome (Syndrome X)
Three or more of the following (NCEP ATP III):
- Central obesity: waist > 102 cm (M), > 88 cm (F)
- Triglycerides ≥ 150 mg/dL
- HDL < 40 mg/dL (M), < 50 mg/dL (F)
- BP ≥ 130/85 mmHg
- Fasting glucose ≥ 100 mg/dL
Bariatric surgery resolves metabolic syndrome in > 95% of patients achieving expected weight loss.
SECTION 2: TYPES OF BARIATRIC SURGERIES
Bariatric surgery is the most effective intervention for significant, sustained weight loss. Procedures are broadly classified by mechanism:
A. Restrictive Procedures
Reduce gastric capacity without bypassing absorptive surfaces.
1. Adjustable Gastric Band (AGB / Lap-Band)
- Inflatable silicone band placed laparoscopically around the gastric cardia
- Creates a small pouch (15-30 mL); band tightness adjustable via subcutaneous port
- Advantages: reversible, adjustable, lowest mortality
- Disadvantages: least weight loss, high revision rate, band slippage/erosion, port complications
- Weight loss: ~20% excess body weight (EBW)
2. Sleeve Gastrectomy (SG)
- Laparoscopic resection of ~80% of stomach along the greater curvature
- Creates a tubular "sleeve" (60-100 mL capacity)
- Irreversible; reduces ghrelin production (hunger hormone)
- Advantages: no anastomosis, no foreign body, good weight loss
- Disadvantages: GERD may worsen, irreversible, gastric leak risk
- Weight loss: ~60-70% EBW
- Now the most commonly performed bariatric procedure worldwide
3. Vertical Banded Gastroplasty (VBG) - largely abandoned
B. Restrictive + Malabsorptive Procedures
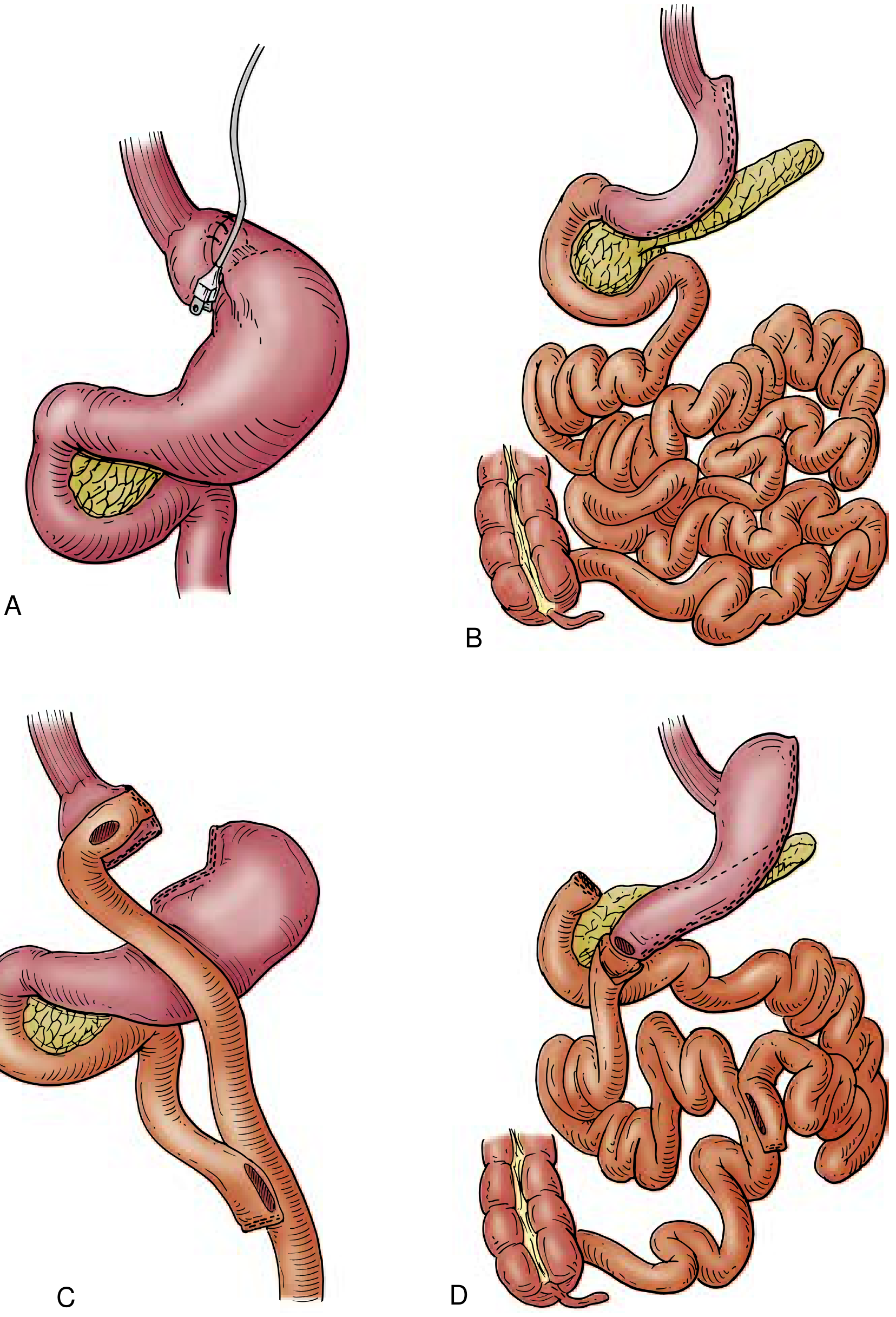
4. Roux-en-Y Gastric Bypass (RYGB)
- Gold standard bariatric procedure
- Small gastric pouch (~30 mL) connected to a Roux limb of jejunum (~75-150 cm)
- Biliopancreatic limb and alimentary limb reunite at jejunojejunostomy
- Mechanism: restriction + malabsorption + gut hormone changes (GLP-1, PYY ↑)
- Advantages: best long-term weight loss, excellent T2DM resolution, durable
- Disadvantages: anastomotic leak, dumping syndrome, nutritional deficiencies (B12, iron, folate, Ca), internal hernias
- Weight loss: ~70-80% EBW
5. Biliopancreatic Diversion (BPD) ± Duodenal Switch (DS)
- Most malabsorptive procedure
- Distal gastrectomy + long Roux limb (250 cm alimentary limb); common channel only 50-100 cm
- With duodenal switch: sleeve gastrectomy + duodenal-ileal anastomosis
- Advantages: maximum weight loss (>80% EBW), excellent metabolic outcomes
- Disadvantages: highest complication rate, severe nutritional deficiencies (fat-soluble vitamins, protein), highest mortality, complex surgery
- Reserved for BMI > 50 or super-obese patients
C. Other/Newer Procedures
- Intragastric balloon: Endoscopic, temporary (6 months), adjunct for pre-op weight loss
- Gastric plication: Endoscopic; experimental
- One anastomosis gastric bypass (OAGB/MGB): Single anastomosis, gaining popularity
| Procedure | Expected EBW Loss | T2DM Resolution | Mortality Risk |
|---|---|---|---|
| Gastric Band | ~20% | 45-60% | 0.1% |
| Sleeve Gastrectomy | ~60-70% | 60-80% | 0.1% |
| RYGB | ~70-80% | 80-90% | 0.3% |
| BPD/DS | >80% | >95% | 1-2% |
SECTION 3: PATHOPHYSIOLOGY OF MORBID OBESITY - ANAESTHETIC RELEVANCE
Understanding the systemic effects is essential for perioperative management:
Respiratory System
- Reduced FRC: Fat deposition on chest wall and diaphragm compresses the lung - FRC may fall below closing capacity in supine position, causing V/Q mismatch and hypoxemia
- Increased oxygen consumption and CO₂ production (proportional to body mass)
- Rapid desaturation on apnea - reduced apnea tolerance (FRC acts as O₂ reservoir)
- Obesity Hypoventilation Syndrome (OHS/Pickwickian): BMI > 30 + PaCO₂ > 45 mmHg without other cause
- Obstructive Sleep Apnea (OSA): High prevalence; screen with STOP-BANG questionnaire
- Pulmonary hypertension in chronic hypoxemia
- Restrictive pattern on spirometry; reduced TLC, RV, ERV
Cardiovascular System
- Increased blood volume and cardiac output (extra 100 mL blood per kg fat)
- Left ventricular hypertrophy (concentric - from HTN; eccentric - from volume overload)
- High incidence of HTN, CAD, cardiomyopathy
- Difficult ECG interpretation - low voltage from fat insulation, false LVH criteria
- Increased risk of arrhythmias
Gastrointestinal System
- Gastroparesis and GERD common
- Increased gastric volume, increased intra-abdominal pressure
- Full stomach risk: Hiatus hernia, increased aspiration risk
- Fatty liver / NAFLD in up to 90%
Endocrine/Metabolic
- High prevalence of Type 2 DM - insulin resistance; risk ↑ by 25% for every 1 kg/m² BMI above 22
- Subclinical hypothyroidism in ~25% of morbidly obese
- Dyslipidemia
- Hypercoagulable state
Pharmacokinetic Changes
Drug dosing must be carefully tailored:
| Drug | Dosing Basis | Reason |
|---|---|---|
| Propofol (induction) | LBW | Mainly distributed to lean tissue |
| Propofol (maintenance) | TBW | Distribution increases with obesity |
| Thiopentone | LBW | |
| Succinylcholine | TBW | Increased plasma cholinesterase |
| Rocuronium/Vecuronium | IBW | Avoid overdose |
| Sugammadex | TBW | |
| Fentanyl | LBW (titrate) | Lipophilic but titrate to effect |
| Remifentanil | LBW | Context-sensitive half-life advantage |
| Midazolam | LBW | Avoid overdose |
| Neostigmine | TBW |
Source: Barash Clinical Anesthesia 9e, Pharmacologic Principles section
SECTION 4: PRE-OPERATIVE EVALUATION
Indications for Bariatric Surgery
- BMI ≥ 40 kg/m² OR
- BMI ≥ 35 with significant obesity-related comorbidities (T2DM, OSA, HTN, joint disease)
- Failure of ≥ 6 months conservative management
- Age 18-65 years (relative limits)
- Psychologically stable; committed to lifestyle changes
Contraindications
- Unstable CAD
- Uncontrolled severe OSA
- Uncontrolled psychiatric disorder (absolute)
- Intellectual disability (IQ < 60)
- Active malignancy with poor 5-year prognosis
- Continued drug/alcohol abuse
- Cirrhotic liver disease with portal hypertension
- Inability to comply with postoperative restrictions
Pre-operative Assessment Framework
1. History
- Duration and degree of obesity
- Previous attempts at weight loss
- Comorbidities: HTN, CAD, T2DM, OSA, GERD, hypothyroidism
- Drug history: antihypertensives, oral hypoglycemics, antidepressants
- Functional capacity (METs): stair climbing, exercise tolerance
- Previous anesthetic difficulties
- STOP-BANG score for OSA (≥ 3 = high risk)
STOP-BANG Questionnaire:
- Snoring
- Tiredness daytime
- Observed apnea
- Pressure (high BP)
- BMI > 35
- Age > 50
- Neck circumference > 40 cm
- Gender = Male
Score ≥ 3: High risk for OSA → refer for sleep study / initiate CPAP
2. Airway Assessment (Critical)
- Mallampati class III/IV (independent risk factor for difficult intubation)
- Neck circumference > 40 cm
- Thyromental distance
- Mouth opening
- Neck extension
- Pretracheal soft tissue thickness on ultrasound
- History of OSA (pharyngeal tissue redundancy)
- Ramped positioning improves laryngoscopic view significantly
3. Cardiovascular Evaluation
- ACC/AHA guidelines; Class III obesity (BMI ≥ 40) warrants ECG + CXR regardless of age if even one CAD risk factor or poor functional capacity
- Echocardiography if LVH, cardiomyopathy, pulmonary HTN suspected
- Stress testing if > 4 METs threshold not met
4. Pulmonary Evaluation
- SpO₂ at rest and on exertion
- ABG if OHS suspected (PaCO₂ > 45 mmHg)
- PFTs if COPD/asthma; restrictive pattern expected
- Polysomnography for OSA
- Chest X-ray
5. Laboratory Investigations
- CBC, blood group and crossmatch
- Blood glucose, HbA1c
- LFTs (NAFLD very common)
- Renal function tests (creatinine, BUN)
- TFTs (hypothyroidism screen)
- Serum electrolytes
- Coagulation profile (PT, aPTT)
- Lipid profile
- 12-lead ECG
- Helicobacter pylori testing (eradicate if positive)
6. Pre-operative Optimization
- Initiate/optimize CPAP therapy if OSA diagnosed - continue perioperatively
- Optimize blood glucose (HbA1c < 8%)
- Control BP
- Pre-operative weight reduction (VLCD - very low calorie diet for 2-4 weeks pre-op reduces liver size, improves surgical access)
- Thromboprophylaxis planning
- Stop metformin 24-48 hours pre-op
- Pre-operative CPAP reduces incidence of post-op pulmonary complications
7. Risk Stratification Tools
- ASA classification: Morbid obesity with comorbidities typically ASA III-IV
- Obesity Surgery Mortality Risk Score (OS-MRS): five risk factors
- BMI ≥ 50
- Male sex
- HTN
- Pulmonary embolism risk (OHS, right heart failure, previous VTE)
- Age ≥ 45 years
- Score 0-1: Class A (0.2% mortality); 2-3: Class B (1.1%); 4-5: Class C (2.4%)
SECTION 5: INTRAOPERATIVE MANAGEMENT
Premedication
- Avoid sedative premedication (benzodiazepines, opioids) - risk of respiratory depression/airway obstruction
- H₂ blockers (ranitidine) + proton pump inhibitors (omeprazole) - reduce gastric volume and acidity
- Metoclopramide 10 mg IV - prokinetic, reduces gastric volume, increases LOS tone
- If CPAP-dependent, apply pre-operatively
Monitoring (Standard + Additional)
- Standard: SpO₂, ETCO₂, ECG, NIBP, temperature
- Arterial line (invasive BP): Often needed - NIBP unreliable with large arm circumference; use correct large cuff (bladder covering ≥ 80% of arm circumference)
- Central venous access if peripheral access difficult
- Foley catheter (urine output monitoring during prolonged procedures)
- Nerve stimulator/TOF monitor - mandatory, neuromuscular blockade harder to assess clinically
- BIS monitor (anesthetic depth - avoid awareness and overdose)
- Oesophageal Doppler / PICCO for haemodynamic monitoring in high-risk patients
Patient Positioning
- Ramped position for intubation: elevate upper body and head until ear aligns with sternum horizontally - significantly improves laryngoscopic view compared to sniffing position alone
- Can achieve with commercially available ramp devices or blanket ramp
- Reverse Trendelenburg (20-30°) improves FRC and reduces regurgitation risk
- Supine position → rhabdomyolysis from gluteal muscle pressure reported
- Careful padding of all pressure points (gel pads)
- Operating table must have adequate weight capacity (bariatric tables)
Airway Management
This is the most critical challenge:
Pre-oxygenation:
- 3-5 minutes of 100% O₂ via tight-fitting mask
- CPAP/BiPAP at 10 cmH₂O during pre-oxygenation dramatically extends safe apnea time by recruiting alveoli and increasing FRC
- Target SpO₂ > 98% before induction
- Reverse Trendelenburg position during pre-oxygenation
Induction Strategy:
- Rapid Sequence Induction (RSI) standard approach - full stomach risk
- Cricoid pressure (Sellick's maneuver) - controversial but widely used
- Drugs: Propofol (2 mg/kg LBW) + Succinylcholine (1.5 mg/kg TBW) or Rocuronium (1.2 mg/kg IBW) for RSI
- Have difficult airway equipment immediately available (videolaryngoscope, airway exchange catheter, emergency surgical airway kit)
- Videolaryngoscopy (e.g. McGrath, GlideScope, C-MAC) preferred or immediately available - improves first-pass success
Intubation:
- Oral endotracheal intubation preferred
- Confirm with waveform capnography (not just SpO₂)
- Lubricated tube stylet, bougie available
- Backup: LMA Supreme as bridge to surgical airway
If Anticipated Difficult Airway:
- Awake fibreoptic intubation (AFOI) - gold standard for anticipated difficult airway
- Nasal route preferred for AFOI
- Adequate topical anaesthesia: lignocaine 4% spray; transtracheal block
Induction Agents
- Propofol: 1-2 mg/kg LBW (induction); avoid overdose
- Thiopentone: LBW dosing
- Ketamine: useful in haemodynamically compromised; 1-2 mg/kg IBW
Maintenance of Anaesthesia
- Total Intravenous Anaesthesia (TIVA): Preferred for bariatric surgery
- Propofol infusion: TBW-based dosing for maintenance
- Remifentanil: LBW (context-insensitive - ideal for obese)
- Reduces PONV vs inhalational agents
- Inhalational agents: Desflurane preferred (lowest fat solubility, fastest emergence) over isoflurane and sevoflurane; however avoid in PONV-high risk
- Nitrous oxide: Avoid - increases bowel distension (laparoscopic surgery), increases PONV
Neuromuscular Blockade
- Succinylcholine: 1.5 mg/kg TBW (plasma cholinesterase activity increases with TBW)
- Rocuronium/Vecuronium: Dose on IBW to avoid prolonged blockade
- Mandatory TOF monitoring throughout
- Sugammadex: Dose on TBW (16 mg/kg TBW for immediate reversal; 4 mg/kg for T2 recovery); preferred reversal agent - faster, more reliable than neostigmine
Ventilation Strategy
- Lung-protective ventilation (LPV):
- Tidal volume (VT): 6-8 mL/kg PBW (NOT TBW - prevents volutrauma)
- PEEP: 10-15 cmH₂O (reduces atelectasis, improves oxygenation)
- Recruitment maneuvers: Apply at induction and during surgery (sustained inflation 40 cmH₂O × 30 sec or incremental PEEP)
- Respiratory rate: titrate to normocapnia (PaCO₂ 35-45)
- FiO₂: lowest to maintain SpO₂ ≥ 95%
- Reverse Trendelenburg position maintains FRC better than supine
- ETCO₂ may underestimate PaCO₂ by 5-10 mmHg in obese patients - ABG correlation recommended
Laparoscopic Considerations
- Pneumoperitoneum (CO₂ insufflation to 12-15 mmHg):
- Further reduces FRC
- Increases airway pressures
- CO₂ absorption increases ETCO₂ - increase RR accordingly
- Head-down (Trendelenburg) → even worse FRC; head-up preferred for bariatric procedures (reverse Trendelenburg or beach chair)
- Vasovagal response on peritoneal insufflation
- Risk of pneumothorax, surgical emphysema, pneumomediastinum
Fluid Management
- Goal-directed fluid therapy recommended
- Avoid excess crystalloid (increased tissue oedema, worse oxygenation post-op)
- Estimated blood volume (EBV) ~50 mL/kg TBW
- Urine output target ≥ 0.5 mL/kg/hr (based on IBW, not TBW)
Analgesia (Multimodal)
- Opioid-sparing strategy preferred (reduces respiratory depression, PONV):
- Paracetamol (acetaminophen) - dose on LBW (max 2g/dose)
- NSAIDs (ketorolac, diclofenac) - unless contraindicated
- Dexmedetomidine infusion: reduces opioid requirements, anxiolytic, no respiratory depression
- Ketamine (sub-anaesthetic doses 0.1-0.5 mg/kg): adjunct analgesia
- Lignocaine infusion: perioperative systemic local anaesthetic reduces opioid requirements
- Regional techniques: TAP block (Transversus Abdominis Plane), wound infiltration, epidural (for open procedures)
- If opioids required: use short-acting agents (remifentanil intraop; fentanyl PCA carefully titrated)
VTE Prophylaxis
- Mechanical: Pneumatic compression devices (PCDs) from induction; TED stockings
- Pharmacological: Low-molecular-weight heparin (LMWH - enoxaparin) - dose on TBW (higher doses needed: enoxaparin 0.5 mg/kg TBW BD or 40 mg BD); start 12 hrs post-op
- Prophylactic IVC filter in very high-risk patients (prior VTE, OHS, pulmonary hypertension)
- Maintain early mobilisation post-operatively
SECTION 6: POST-OPERATIVE MANAGEMENT
Post-Anaesthesia Care Unit (PACU)
- Semi-sitting / head-up position (30-45°) at all times - prevents atelectasis and aspiration
- Never nurse flat or supine
- SpO₂ monitoring continuously
- Supplemental O₂ initially; target SpO₂ ≥ 92-95%
- Resume CPAP/BiPAP immediately in OSA patients - apply in PACU before fully awake if tolerated
- Criteria for safe extubation:
- Awake, following commands
- TOF ratio ≥ 0.9 (neuromuscular blockade fully reversed)
- SpO₂ ≥ 95% on room air or minimal O₂
- Adequate minute ventilation (RR 10-20)
- Normothermic
Extubation Strategy
- Extubate awake (not deep extubation) - aspiration risk
- Extubate in reverse Trendelenburg or semi-sitting
- Have re-intubation equipment immediately ready
- Consider laryngeal mask (LMA) as bridge if oedema anticipated
Respiratory Management Post-Op
- CPAP/BiPAP for OSA patients (continue home settings)
- Incentive spirometry
- Deep breathing exercises, early physiotherapy
- High-Flow Nasal Cannula (HFNC) if standard O₂ insufficient
- Monitor for pulmonary oedema, atelectasis, pneumonia, respiratory failure
Pain Management Post-Op
- Multimodal analgesia continues:
- Regular paracetamol ± NSAIDs
- Opioid PCA - careful monitoring, lowest effective dose
- TAP block / epidural for open procedures
- Avoid IM injections (unreliable absorption, difficult access)
- Monitor sedation score and respiratory rate with opioids
DVT/PE Prophylaxis
- Continue LMWH for 28 days post-op (extended prophylaxis)
- Early ambulation (within 24 hours)
- Graduated compression stockings
Other Post-Operative Concerns
1. PONV (Post-Operative Nausea and Vomiting)
- Very high risk (female, non-smoker, opioids, history of PONV)
- Triple prophylaxis: Ondansetron + Dexamethasone + Droperidol/Scopolamine
- TIVA preferred to reduce PONV
2. Rhabdomyolysis
- From pressure on muscle groups (gluteal) intraoperatively
- Monitor CK levels, urine output, urine colour
- Aggressive IV hydration if suspected
3. Wound Care
- Obese patients have higher risk of wound infection, dehiscence
- Keep skin folds dry; regular inspection
4. Metabolic/Nutritional
- Blood glucose monitoring (insulin sliding scale)
- Early post-op nutritional support per bariatric team protocol
- Vitamin and mineral supplementation (B12, iron, folate, calcium - especially after RYGB)
5. Discharge Criteria
- For day-case/short-stay: More stringent criteria in obese patients
- SOBA (Society for Obesity and Bariatric Anaesthesia) red flags for day surgery:
- BMI ≥ 50
- Uncontrolled OSA / not on CPAP
- OHS
- Uncontrolled comorbidities
- History of difficult airway
6. Complications of Bariatric Surgery - Post-Op Vigilance
- Anastomotic leak (most serious - presents with tachycardia, fever, peritonism; may need re-operation)
- Internal hernia (RYGB - intermittent abdominal pain)
- Dumping syndrome (RYGB - early or late hypoglycemia)
- Nutritional deficiencies (B12, iron, thiamine, folate, Ca, fat-soluble vitamins)
- GERD worsening (sleeve gastrectomy)
- DVT/PE - up to 3 months post-op
- Wound complications
Summary Diagram
MORBID OBESITY (BMI ≥ 40) FOR BARIATRIC SURGERY
│
▼
PRE-OP ──────────────────────────────────────────
• Airway: Mallampati, neck circ, thyromental
• Cardiac: ECG, Echo, stress test (ACC/AHA)
• Pulmonary: SpO₂, ABG, PFTs, sleep study
• Labs: CBC, LFTs, RFTs, HbA1c, TFTs
• OS-MRS risk score
• Optimize: CPAP, glucose, BP, pre-op VLCD
│
▼
INTRA-OP ────────────────────────────────────────
• RSI + Ramped position + Videolaryngoscope
• TIVA (Propofol + Remifentanil)
• Lung-protective ventilation (6-8 mL/kg PBW + PEEP 10-15)
• IBW dosing NMB, sugammadex reversal
• Multimodal analgesia (opioid-sparing)
• Mechanical + LMWH VTE prophylaxis
│
▼
POST-OP ─────────────────────────────────────────
• Semi-sitting, SpO₂ monitoring
• Resume CPAP immediately
• Awake extubation, re-intubation ready
• Multimodal analgesia, PONV prophylaxis
• Early mobilisation, LMWH × 28 days
• Monitor for anastomotic leak, PE, rhabdo
Key Exam Points:
- Drug doses: Succinylcholine on TBW; NMB (rocuronium, vecuronium) on IBW; Sugammadex on TBW; Propofol induction on LBW, maintenance on TBW; Remifentanil on LBW
- Tidal volume always on PBW, never TBW
- Pre-oxygenation + CPAP extends safe apnea time significantly
- Ramped position (ear-sternum alignment) is optimal for intubation
- TIVA (propofol + remifentanil) preferred over inhalational agents for bariatric surgery
- Desflurane is preferred inhalational agent if used (lowest fat solubility)
- Never nurse post-op bariatric patient flat; always semi-sitting ≥ 30°
- PONV triple prophylaxis is standard
- Recent 2025 guidelines from the Society for Obesity and Bariatric Anaesthesia (SOBA) emphasize systematic airway management best practices in obese patients (PMID: 40468902)
Sources: Miller's Anesthesia 10e (Chapters on Morbid Obesity and Bariatric Surgery), Barash Clinical Anesthesia 9e (Chapter 45), Fischer's Mastery of Surgery 8e, Current Surgical Therapy 14e (Metabolic and Bariatric Surgery chapter), Bailey & Love's Surgery 28e
Create a comprehensive study guide PDF on anesthetic management of obese patients for exam revision
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
Running Command
mkdir -p /home/daytona/workspace/obesity-anaesthesia-guide && python3 -c "import reportlab; print('reportlab ok')" && python3 -c "from reportlab.lib import colors; print('colors ok')"
This is a shared conversation. Sign in to Orris to start your own chat.