Poynting effect
Searching the Web
Poynting effect physics explanation
Searching the Web
Poynting effect rubber elasticity nonlinear mechanics
The "Poynting effect" actually refers to three distinct phenomena, all named after English physicist John Henry Poynting (1852-1914), but otherwise completely unrelated to each other.
1. Solid Mechanics - The Poynting Effect in Elasticity
This is what most physicists and engineers mean today by "the Poynting effect."
What it is: A nonlinear elastic phenomenon where a material under shear or torsion develops stresses (or deformations) perpendicular to the applied loading direction.
Two manifestations:
- Torsion version (classical, 1909): When a cylinder or wire is twisted, it tends to elongate axially. Poynting observed this experimentally with metal wires - a loaded wire gets longer when twisted. To maintain constant length, you must apply a compressive axial force. This is the positive Poynting effect.
- Simple shear version: When a soft elastic block is sheared between two plates, normal stresses develop perpendicular to the shearing direction. To maintain constant separation between the plates, you must apply a compressive force - the plates are pushed apart by the material.
Why it happens: It is an inherently nonlinear (finite strain) effect. Linear elasticity predicts zero normal stress from shear. The effect only appears at second order in the strain, arising from the nonlinear constitutive response of the material (the stored energy function must contain terms beyond quadratic in strain).
Reverse Poynting effect: Some soft materials (certain gels, biopolymer networks) actually shorten under torsion or pull the plates together under shear. This "negative" or reverse Poynting effect has been actively studied in recent years and is linked to strain-stiffening constitutive models.
Practical significance:
- Characterizing rubber, biological tissues, hydrogels
- Understanding soft robotics materials
- Biomechanics (tendons, arteries exhibit Poynting-type responses)
- Seismic wave propagation in nonlinear media
2. Thermodynamics - The Poynting Effect on Vapor Pressure
What it is: The increase in vapor pressure of a liquid when external (mechanical) pressure is applied to it by an insoluble, non-condensable gas.
Origin: Poynting generalized the Kelvin equation in 1881, showing that vapor pressure changes not only due to surface curvature (Laplace pressure) but due to any applied pressure source.
The physics: Applying pressure to a liquid increases the chemical potential of the liquid phase. The vapor phase responds by increasing its pressure to maintain thermodynamic equilibrium. The relationship comes from the Maxwell relation:
(∂μ/∂P){T,N} = (∂V/∂N){T,P} = V_m (molar volume of liquid)
Formula (Poynting correction):
ln(P_vap / P°_vap) ≈ V_m · ΔP / RT
where ΔP is the applied excess pressure.
Important nuance: If the pressurizing gas is soluble in the liquid, it also lowers vapor pressure via a colligative effect, which can cancel or overwhelm the Poynting increase.
Applications:
- Fuel injection systems (pressure on liquid fuel raises its vapor pressure)
- Supercritical extraction processes
- Phase equilibrium calculations in chemical engineering
- Enhanced oil recovery
3. Electromagnetism - The Poynting Vector / Poynting's Theorem
Though usually called the "Poynting vector" rather than the "Poynting effect," it is sometimes grouped under the same name.
The Poynting vector S describes the directional energy flux (power per unit area) of an electromagnetic field:
S = E × H (W/m²)
In SI units, using E (V/m) and H (A/m), S has units of watts per square meter.
Poynting's theorem is the EM energy conservation law:
∂u/∂t = -∇·S - J·E
- ∂u/∂t = rate of change of EM energy density
- -∇·S = energy flowing into the region
- -J·E = power delivered to charges (resistive heating, etc.)
Counterintuitive result: Energy in a circuit does not flow through the wires - it flows through the surrounding electromagnetic field. For a coaxial cable carrying current I and voltage V, the Poynting vector points axially along the cable in the dielectric space between conductors, not inside the conductor.
Summary Table
| Context | What It Describes | Year |
|---|---|---|
| Solid mechanics | Normal stress/strain from shear/torsion (nonlinear elasticity) | 1909 |
| Thermodynamics | Vapor pressure increase under applied mechanical pressure | 1881 |
| Electromagnetism | Directional energy flux of EM fields (S = E × H) | 1884 |
All three are named after J. H. Poynting, who made foundational contributions across multiple branches of physics in the late 19th and early 20th centuries. The solid mechanics Poynting effect is currently the most active research area, with a 2025 review in the Journal of Elasticity (Springer, 2025) covering recent results on soft elastic materials including the reverse Poynting effect.
Fast ultrasound m.d.anaesthesi a 20 marks answer
Reading File
Finding Sources
Finding Sources
Searching the Web
FAST ultrasound anaesthesia MD exam focused assessment sonography trauma protocol
Reading File
Reading File
Reading Web Page
https://pedsanesthesia.org/wp-content/uploads/2025/06/309029…
Reading File
Finding Sources
Loading Image
Here is a complete, well-structured 20-mark MD Anaesthesia answer on FAST Ultrasound:
FAST Ultrasound in Anaesthesia
(Focused Assessment with Sonography for Trauma)
1. Introduction and Definition
FAST (Focused Assessment with Sonography for Trauma) is a rapid, bedside, goal-directed ultrasound protocol designed to detect pathological free fluid (anechoic collections) in the pericardial, peritoneal, and pleural cavities in trauma and critically ill patients. It is a key component of Point-of-Care Ultrasound (PoCUS) and is integrated into ATLS (Advanced Trauma Life Support) as an adjunct to the primary survey.
Originally developed as an alternative to Diagnostic Peritoneal Lavage (DPL), FAST is:
- Non-invasive
- Repeatable
- Rapid (completable in under 5 minutes by trained personnel)
- Bedside-applicable without disruption of resuscitation
The American Board of Anesthesiology (ABA) now recognizes FAST as a key competency in trauma anaesthesia practice.
2. Principle
FAST exploits the principle that free intraperitoneal fluid settles into dependent spaces when the patient is supine. Blood, ascites, or other pathological fluid appears as an anechoic (black) collection in these spaces. Even as little as 100-200 mL of free fluid is detectable by an experienced sonographer.
3. The Four Standard FAST Views
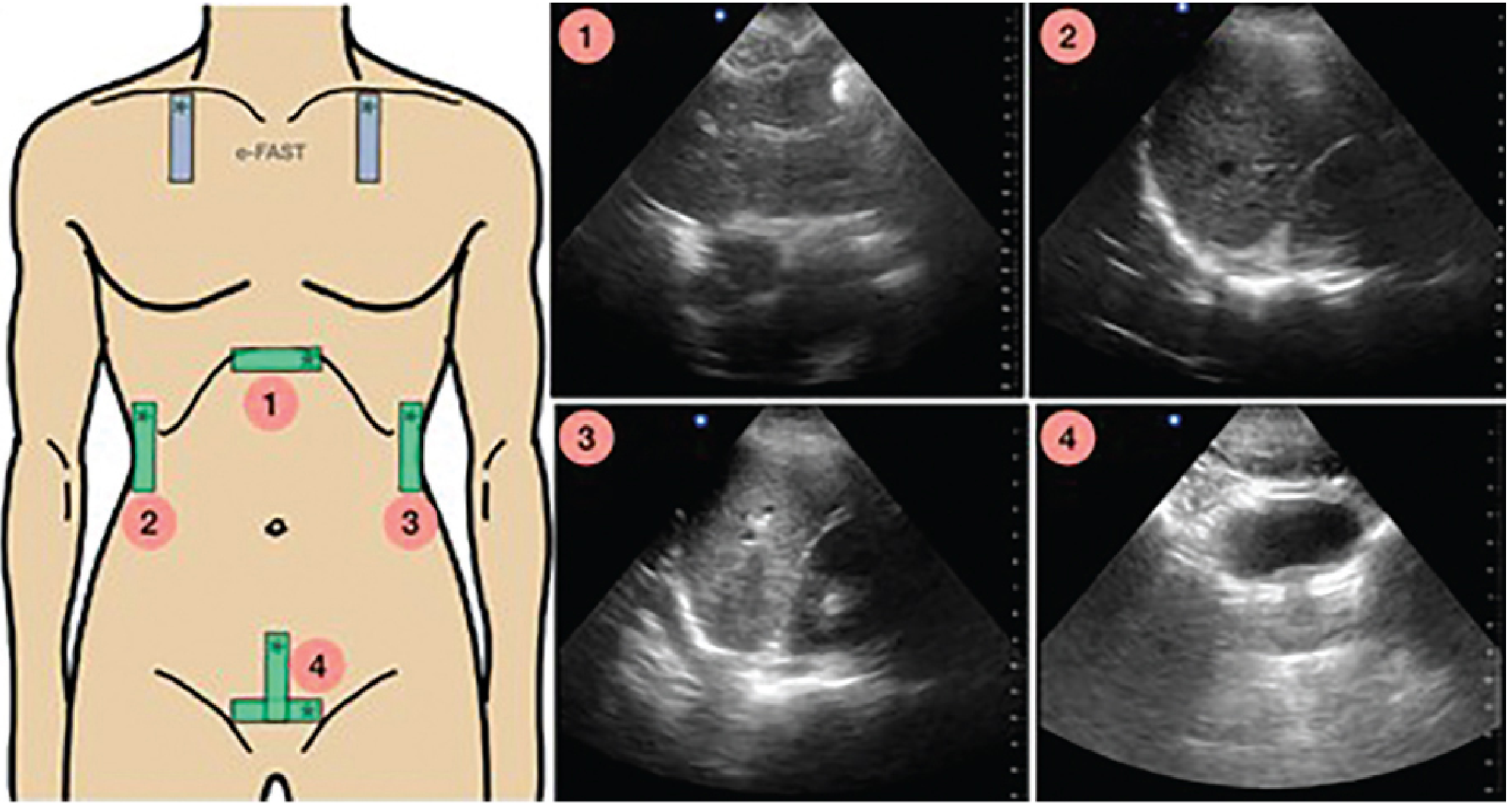
Probe placements (1-4) and corresponding normal ultrasound images: (1) Subxiphoid cardiac, (2) Right upper quadrant/Morison's pouch, (3) Left upper quadrant/perisplenic, (4) Suprapubic/pelvic. Blue probes at bilateral anterior chest = E-FAST additions.
| View | Position | Probe Placement | What Is Assessed |
|---|---|---|---|
| Subxiphoid (pericardial) | Subxiphoid, probe angled toward left shoulder | Phased array / curvilinear | Pericardial effusion, cardiac tamponade, cardiac activity |
| RUQ - Morison's Pouch | Right flank, mid-axillary line, 8th-11th rib | Curvilinear | Hepatorenal space - most sensitive for haemoperitoneum |
| LUQ - Perisplenic | Left flank, posterior axillary line, 8th-11th rib | Curvilinear | Splenorenal space, subdiaphragmatic fluid |
| Suprapubic (pelvic) | Just above pubic symphysis, sagittal then transverse | Curvilinear | Pouch of Douglas (females), rectovesical pouch (males) |
Scanning sequence: Subxiphoid → RUQ → LUQ → Suprapubic (can be adapted based on clinical priority).
Probe used: Low-frequency curvilinear probe (3-5 MHz) for abdominal views; phased array for cardiac window.
4. Extended FAST (E-FAST)
E-FAST adds bilateral anterior thoracic views to the standard FAST to assess for:
- Pneumothorax
- Haemothorax / pleural effusion
- Diaphragm dysfunction
Technique for pneumothorax assessment (E-FAST):
- High-frequency linear probe (10-15 MHz) in the parasagittal orientation on the anterior chest wall
- Patient supine - air rises anteriorly, so pneumothorax will be anterior
- Normal finding: "Lung sliding sign" - dynamic shimmering movement of visceral pleura against parietal pleura with respiration
- Positive for pneumothorax:
- Absence of lung sliding
- "Barcode sign" on M-mode (horizontal lines throughout, replacing the normal "seashore sign")
- Lung point - transition between sliding and absent sliding confirms pneumothorax
For haemothorax: Costophrenic angle view using curvilinear probe; can detect as little as 10 mL of fluid.
| Finding | B-mode | M-mode |
|---|---|---|
| Normal lung | Lung sliding present | "Seashore sign" (waves above, sand below pleura) |
| Pneumothorax | No lung sliding | "Barcode sign" (all horizontal lines) |
| Haemothorax | Anechoic/hypoechoic collection above diaphragm | - |
5. Diagnostic Performance
| Parameter | Blunt Trauma | Penetrating Trauma |
|---|---|---|
| Sensitivity | 74-82% (normalised); approaches 100% in hypotensive patients | 28-75% |
| Specificity | 96-99% | 94-100% |
| E-FAST for pneumothorax | Sensitivity 91%, Specificity 99% | Outperforms CXR (CXR sensitivity only 47%) |
Sources: Barash Clinical Anaesthesia 9e; Roberts and Hedges Emergency Medicine Procedures
6. Role of FAST in Anaesthesia Practice
A. Trauma Resuscitation
- Performed simultaneously with resuscitation without interrupting ATLS primary survey
- A positive FAST in a hypotensive patient directs the patient to the operating room for laparotomy without waiting for CT scan
- Reduces time to surgery, reduces CT use, reduces hospital length of stay (Level I randomised trial evidence)
B. Peri-operative Setting
- Unexplained haemodynamic instability in PACU or ICU - FAST can rapidly identify haemoperitoneum
- Post hip arthroscopy pain - free fluid in Morison's pouch from fluid extravasation from hip joint capsule
- Critically ill patients in PACU - FAST combined with cardiac, lung, IVC, and aorta views (RUSH protocol)
- Ruptured ectopic pregnancy in the emergency/operating setting
C. Airway Management Adjunct
- Identifies cricothyroid membrane for front-of-neck access (FONA)
- Predicts difficult airway
- Confirms endotracheal vs. oesophageal intubation (especially valuable in low cardiac output where capnography is unreliable)
D. Cardiac Tamponade Diagnosis
- Subxiphoid view rapidly shows pericardial effusion and diastolic collapse of right ventricle (tamponade physiology)
- Guides pericardiocentesis
7. Limitations of FAST
| Limitation | Clinical Impact |
|---|---|
| Operator dependent | Small collections missed by inexperienced operators |
| Retroperitoneal injuries (renal, aortic) NOT detected | Missed haemorrhage; CT mandatory |
| Bowel, mesenteric, pancreatic, diaphragmatic injuries missed | Requires CT for complete assessment |
| Obesity, subcutaneous emphysema, bowel gas | Degrades image quality |
| Pericardial fat vs. effusion confusion | False positive pericardial diagnosis |
| Pre-existing ascites / peritoneal dialysis | Cannot differentiate from new haemorrhage |
| Gallbladder, ovarian cysts, hepatic veins mistaken for free fluid | False positives |
| Poor in penetrating trauma | Lower sensitivity vs. blunt trauma |
Key principle: A negative FAST does not exclude injury. When clinical suspicion is high, CT scan is mandatory.
8. I-AIM Framework (Anaesthesia Application)
| Scenario | |
|---|---|
| Indication | Hypotensive trauma; re-evaluation of trauma; abdominal pain post hip arthroscopy; critically ill in PACU |
| Acquisition | All four standard views (+ thoracic if E-FAST) |
| Interpretation | Anechoic free fluid in any view = positive |
| Management | Positive + unstable → OR; positive + stable → CT; negative + high suspicion → CT |
9. FAST vs. Competing Modalities
| Parameter | FAST | CT Abdomen | DPL |
|---|---|---|---|
| Speed | <5 minutes | 15-30 min | 15-20 min |
| Invasive | No | No | Yes |
| Radiation | None | High | None |
| Sensitivity (haemoperitoneum) | 74-100% | >95% | >95% |
| Retroperitoneum | No | Yes | No |
| Bedside | Yes | No | Yes |
| Repeatable | Yes | Limited | No |
10. Special Considerations
- Paediatrics: Less reliable; CT remains gold standard for stable paediatric trauma (JAMA 2017)
- Pregnancy: FAST is safe (no radiation); evaluates peritoneum and pericardium; uterus displaces other organs - technical modifications needed
- Penetrating thoracic trauma: Subxiphoid pericardial view is particularly valuable to rule out haemopericardium before proceeding to OR
- Training: FAST is rapidly learnable - skill acquisition demonstrated with a small number of supervised exams; reflects rapidly along a learning curve
Summary
FAST is an indispensable bedside diagnostic tool for the anaesthesiologist managing trauma, haemodynamically unstable, or critically ill patients. Its speed, repeatability, non-invasiveness, and ability to diagnose life-threatening conditions (haemoperitoneum, haemopericardium, pneumothorax, haemothorax) at the bedside during active resuscitation make it superior to DPL and complementary to CT. E-FAST extends its diagnostic reach to the thoracic cavity. With the ABA now mandating PoCUS competency including FAST, every anaesthesiologist must be proficient in its acquisition and interpretation.
References:
- Barash, Cullen and Stoelting's Clinical Anaesthesia, 9th ed., Chapter 53 - Point-of-Care Ultrasound
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - FAST, E-FAST and RUSH Exams
- Manson WC et al. FAST for the regional anaesthesiologist and pain specialist. Reg Anesth Pain Med 2019;44:540-548
- ATLS 10th Edition, American College of Surgeons
This is a shared conversation. Sign in to Orris to start your own chat.