Hypertrophic pachymeningitis etiology, Patho physiology, clinical feature,differential, radiological feature,treatment and rescent update from standard source
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypertrophic pachymeningitis etiology treatment
Reading File
Reading File
Reading Article
PMID: 37062439
Reading File
Reading Article
PMID: 36882352
Searching PubMed
hypertrophic pachymeningitis IgG4 rituximab management
Reading File
Loading Image
Loading Image
Reading Article
PMID: 41827958
Searching the Web
hypertrophic pachymeningitis 2024 2025 pathophysiology IgG4 ANCA diagnosis treatment update
Here is a comprehensive review of Hypertrophic Pachymeningitis (HP):
Hypertrophic Pachymeningitis (HP)
Definition
Hypertrophic pachymeningitis is a rare, chronic inflammatory disorder characterized by diffuse or localized thickening of the dura mater, visible on MRI as gadolinium-enhancing dural thickening. It may involve the cranial dura, spinal dura, or both. When no systemic cause is identified after full workup (cultures, serology, biopsy), the term idiopathic hypertrophic pachymeningitis (IHP) is applied.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2586
- Adams and Victor's Principles of Neurology, 12th Ed., p. 648
1. Etiology
HP is broadly classified as secondary (identifiable cause) or idiopathic.
Immune-Mediated / Autoimmune (most common non-infectious group)
| Condition | Notes |
|---|---|
| IgG4-Related Disease (IgG4-RD) | Now accounts for ~10-20% of HP cases; increasingly recognized; associated with autoimmune pancreatitis, sclerosing cholangitis |
| ANCA-Associated Vasculitis (AAV) | Especially Granulomatosis with Polyangiitis (GPA); 3-4% of AAV patients develop HP; MPO-ANCA more common than PR3-ANCA in HP-AAV |
| Rheumatoid Arthritis | Granulomatous dural infiltration |
| Sarcoidosis | Neurosarcoidosis |
| Sjögren Syndrome | |
| Systemic Lupus Erythematosus | |
| Behçet Disease | |
| Giant Cell (Temporal) Arteritis |
Infectious
- Tuberculous meningitis
- Syphilis (historically the most common cause - pachymeningitis cervicalis hypertrophica described by Charcot and Joffroy)
- Fungal infections (Aspergillus, Cryptococcus)
- Lyme disease
- HTLV-1
- Pseudomonas (malignant external otitis)
- Cysticercosis
Neoplastic
- Dural carcinomatosis
- Lymphoma
- Meningioma (mimicker)
- Metastatic disease from adjacent skull bone
Other
- Trauma
- Intracranial hypotension (spontaneous or post-lumbar puncture) - produces venous engorgement mimicking dural enhancement
Idiopathic HP remains a diagnosis of exclusion after thorough evaluation.
Sources: Bradley and Daroff's eBOX 104.10; Adams and Victor's, p. 648; Shimojima & Sekijima, Autoimmun Rev 2023 [PMID 37062439]
2. Pathophysiology
General Mechanism
The dura mater undergoes a chronic fibro-inflammatory reaction. All three meningeal layers (dura, pia, arachnoid) may be involved, with dense fibrous adhesions binding them together. This was first described by Charcot and Joffroy in the cervical region.
IgG4-RD Mechanism
- Activated CD4+ T follicular helper cells and plasmablasts drive the production of IgG4 antibodies
- Characteristic histology: dense lymphoplasmacytic infiltration with IgG4+ plasma cells (>10-40 per HPF), storiform fibrosis, and obliterative phlebitis
- The IgG4+/IgG+ plasma cell ratio is ≥30%
- Fibrotic phenotype leads to dural thickening; process also affects salivary glands, pancreas, kidneys, lungs
ANCA-Associated Mechanism
- Neutrophil and monocyte activation by ANCA (anti-MPO or anti-PR3 antibodies)
- Granulomatous inflammation with fibrous dural thickening
- Notably, classic GPA histological features (necrotizing granulomatous vasculitis) may not always be present in dural biopsy
Consequences of Dural Thickening
- Cranial nerve compression as nerves traverse thickened dura
- Venous sinus compression → hydrocephalus, raised intracranial pressure
- Spinal cord / nerve root compression → myelopathy, radiculopathy
- Cerebral venous thrombosis (increasingly recognized, especially IgG4-HP)
Sources: Adams and Victor's, p. 648-649; Shimojima & Sekijima 2023 [PMID 37062439]; Liu et al., Diagnostics 2026 [PMID 41827958]
3. Clinical Features
HP has a subacute to chronic onset (weeks to months) and may follow a monophasic, progressive, or relapsing-remitting course.
Common Symptoms
| Feature | Frequency |
|---|---|
| Headache | 40-70%; most common presenting symptom |
| Cranial neuropathies | 30-70%; CN II, III, IV, VI (ophthalmoplegia, diplopia, visual loss), CN VIII (hearing loss), CN V (facial numbness/pain) |
| Visual disturbance | Diplopia, visual impairment, sudden visual loss |
| Ataxia | Cerebellar involvement |
| Seizures | When hemispheric dura involved |
| Spinal symptoms | Radiculopathy, myelopathy, sensory loss, amyotrophy (especially cervical region) |
Cranial HP Specifics
- Headache is typically persistent and pressure-like
- Orbital involvement: dysaesthesia around orbit
- Peri-orbital/cavernous sinus involvement: acute bilateral ophthalmoplegia
IgG4-HP Specific Profile
- Male predominance (~2-3:1), age 40-70 years
- 38.5% misdiagnosis rate (commonly mistaken for meningioma)
- Extraneurological manifestations in >50% of cases (pancreas, salivary glands, kidneys, lungs)
ANCA-HP Specific Profile
- ENT manifestations: otitis media, sinusitis, mastoiditis
- Sudden visual loss is a warning feature
- HP may be the initial clinical episode of AAV in 3-4% of patients
CSF Findings
- High protein (common)
- Lymphocytic pleocytosis
- Sterile (no organisms)
- Plasma cells not prominent (contrast with neurosyphilis/Listeria)
Sources: Bradley and Daroff's, p. 2586; Practical Neurology 2025; Liu et al. 2026 [PMID 41827958]
4. Differential Diagnosis
Key Differentials (Causes of Thickened Enhancing Dura on MRI)
| Category | Conditions |
|---|---|
| Immune-mediated HP mimickers | GPA vs. IgG4-RD (major diagnostic challenge), Rheumatoid pachymeningitis, Neurosarcoidosis, SLE, Sjögren |
| Infectious | TB meningitis, Neurosyphilis, Cryptococcal meningitis, Lyme disease, Fungal, HTLV-1 |
| Neoplastic | Meningioma (most common mimicker), Dural lymphoma, Metastatic carcinoma, Primary CNS lymphoma |
| Vascular | Intracranial hypotension (spontaneous or post-LP), Cerebral venous thrombosis |
| Other inflammatory | Behçet, Giant cell arteritis, Isolated CNS angiitis, Vogt-Koyanagi-Harada syndrome |
| Trauma | Post-surgical dural reaction |
GPA vs. IgG4-RD - A Common Diagnostic Dilemma
| Feature | GPA | IgG4-RD |
|---|---|---|
| ANCA | MPO or PR3 positive | Usually negative |
| Serum IgG4 | May be mildly elevated | Significantly elevated |
| Histology | Granulomatous necrotizing vasculitis (not always in dura) | Storiform fibrosis, obliterative phlebitis |
| ENT involvement | Sinusitis, otitis media common | Less prominent |
| Other organ involvement | Lungs, kidneys | Pancreas, salivary glands, kidneys |
Sources: Bradley and Daroff's eBOX 104.10; Shimojima 2023 [PMID 37062439]; Matias et al., Acad Radiol 2023 [PMID 36882352]
5. Radiological Features
MRI - the Gold Standard Investigation
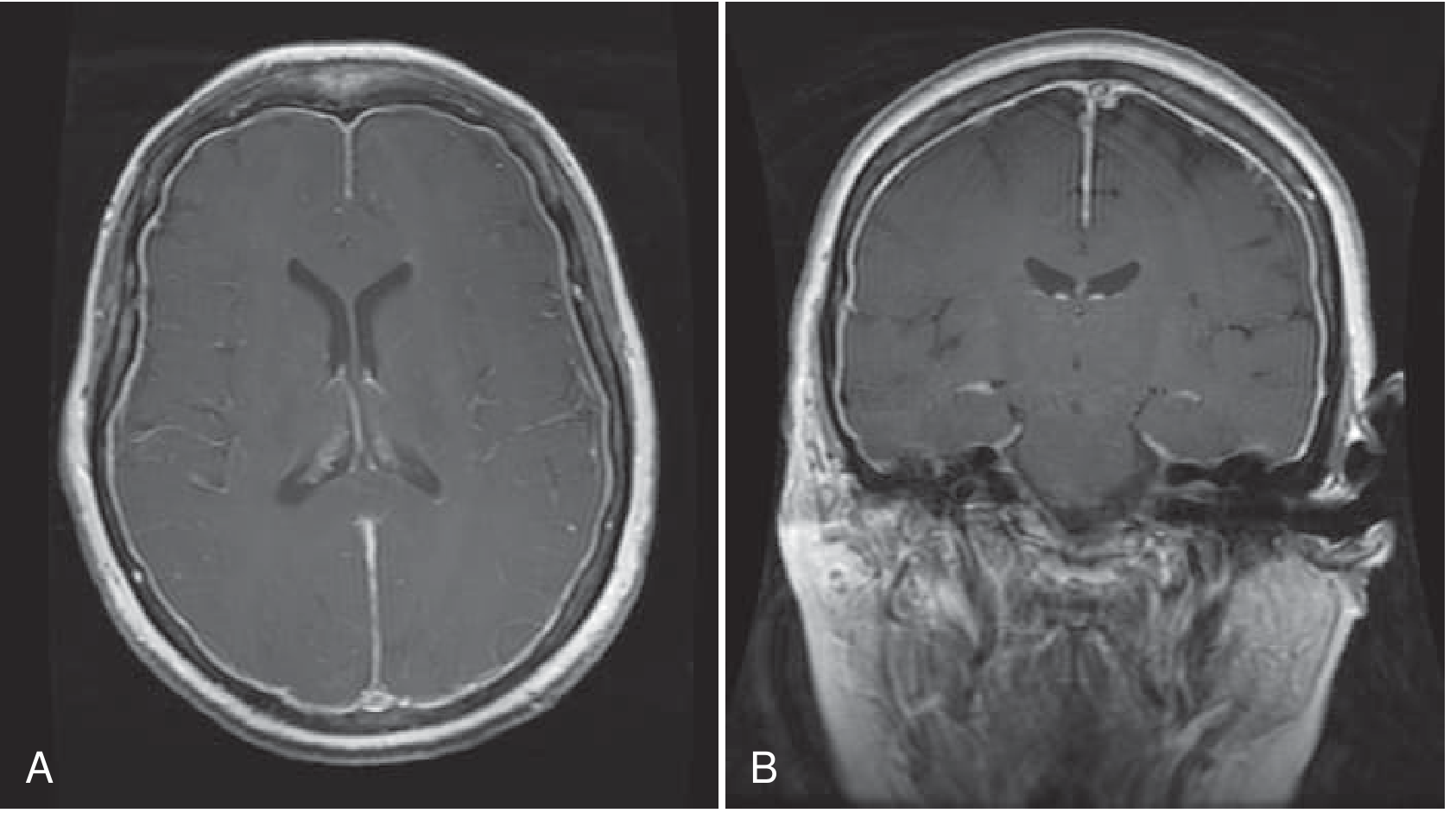
Fig. 104.39 - Axial (A) and coronal (B) T1-weighted images post-gadolinium infusion showing pachymeningitis. Enhancement is thin and diffuse; other cases show localized or irregular thickening. (Bradley and Daroff's Neurology)
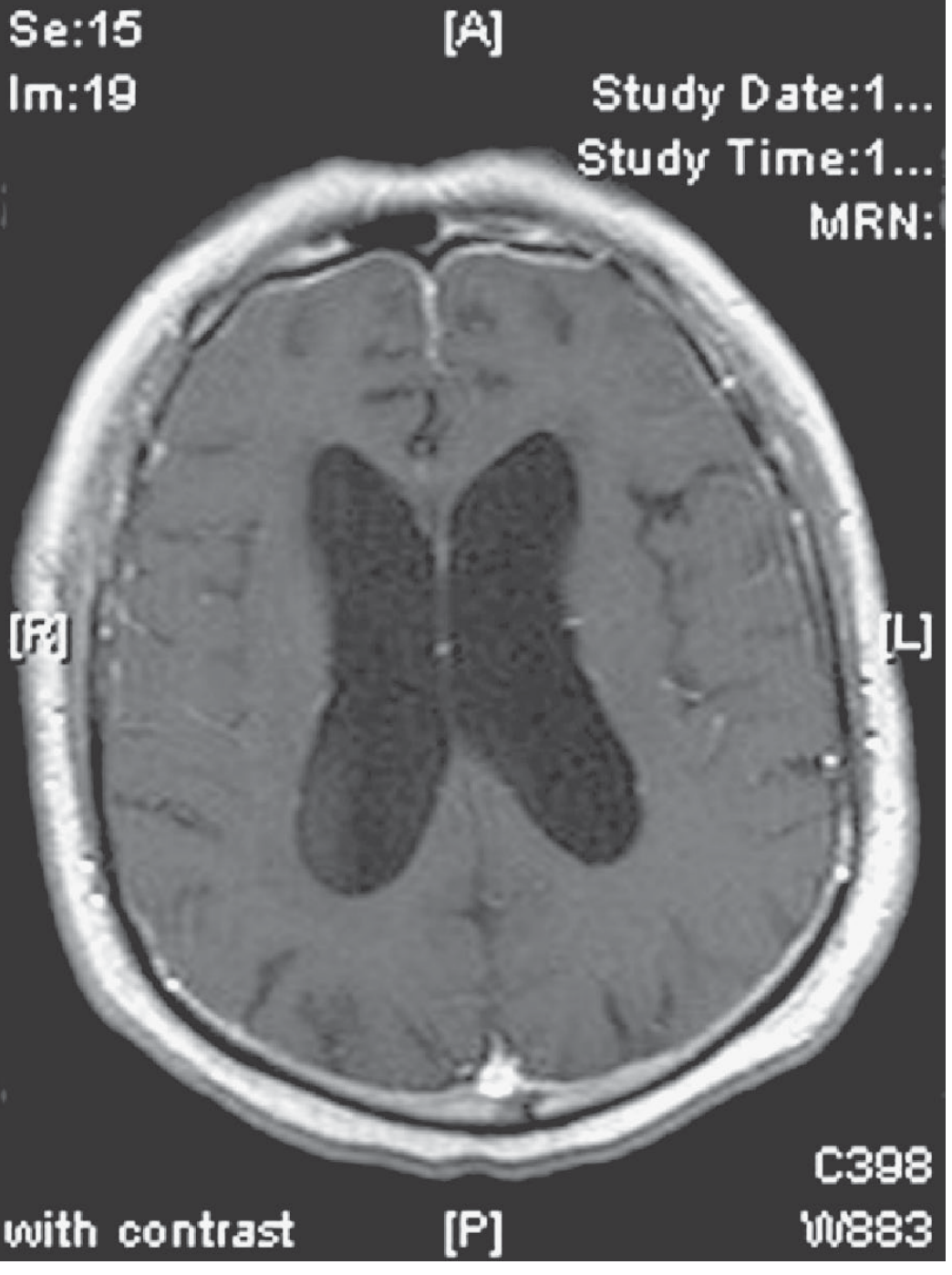
Fig. 29-7 - Gadolinium-enhanced MRI showing diffuse rheumatoid pachymeningitis in an older man with severe headaches, hydrocephalus, and mental dullness. (Adams and Victor's Neurology)
MRI Characteristics
T1 Post-Contrast (Gadolinium):
- Diffuse or localized irregular dural thickening with enhancement
- Can be smooth/thin (like intracranial hypotension) or nodular/irregular (more suggestive of inflammatory/neoplastic cause)
- "Sandwich" pattern (peripheral enhancement of thickened dura) - classic for IgG4-HP
- Tentorial, falcine, convexity, skull base involvement
T2/FLAIR:
- Thickened dura is often hypointense on T2 (fibrous tissue)
- IgG4-HP: may show T2 hypointensity due to dense fibrosis
Key MRI Distinctions:
| Pattern | Suggests |
|---|---|
| Diffuse smooth enhancement | Intracranial hypotension (CSF leak) |
| Diffuse/irregular thickening | Inflammatory HP |
| Nodular/mass-like thickening | Neoplasm or IgG4-HP mimicking meningioma |
| Dural "tail" | Meningioma (but also seen in HP) |
| Tentorium/skull base predominance | IgG4-RD, GPA, sarcoid |
Advanced Sequences:
- DWI - diffusion restriction in lymphoma
- MR spectroscopy - for neoplasm vs. inflammation
- Whole-body CT/PET - essential to detect extraneurological IgG4-RD or malignancy
Sources: Bradley and Daroff's, p. 2590; Matias et al. 2023 [PMID 36882352]; Practical Neurology 2025
6. Diagnostic Workup
A stepwise approach is required since HP is a diagnosis of exclusion:
- MRI brain and spine with gadolinium (mandatory)
- Blood tests: CBC, ESR, CRP, ANA, ANCA (MPO, PR3), RF, anti-CCP, ACE, serum IgG subclasses (IgG4), VDRL/TPHA, HIV, Lyme serology, fungal serology, serum calcium
- CSF analysis: cell count, protein, glucose, culture, cytology, oligoclonal bands, ACE, VDRL
- Chest CT / Whole body CT or PET-CT - to identify systemic disease
- Dural biopsy - gold standard for definitive tissue diagnosis
IgG4-HP Diagnostic Criteria (histopathological gold standard):
- Dense lymphoplasmacytic infiltration
- Storiform fibrosis
- IgG4+ plasma cells >10-40 per HPF
- IgG4+/IgG+ ratio ≥30%
- Serum IgG4 significantly elevated (normal <1350 μg/mL; diagnostic cut-off varies)
7. Treatment
First-Line: Corticosteroids
- Prednisolone/Prednisone is the cornerstone of treatment for all immune-mediated HP
- Starting dose typically 0.5-1 mg/kg/day (IHP and IgG4-HP) or 1 mg/kg/day (ANCA-HP)
- Gradual taper over months; relapse is common during tapering
- Favorable response in ~96% of IgG4-HP treated cases (Liu et al. 2026)
Steroid-Sparing Immunosuppressants (for maintenance or relapse)
| Agent | Evidence |
|---|---|
| Azathioprine | Steroid-sparing; used in IHP and IgG4-HP |
| Methotrexate | ANCA-HP and IgG4-HP |
| Cyclophosphamide | ANCA-AAV-associated HP (induction) |
| Mycophenolate mofetil | ANCA-HP maintenance |
Rituximab (anti-CD20)
- Effective for refractory HP across all immune-mediated causes
- Particularly valuable in refractory ANCA-HP (GPA) and refractory IgG4-HP
- Increasingly used as induction therapy in severe ANCA-HP
- A 2023 case report [PMID 37292126] reported successful use of intrathecal rituximab for IgG4-RHP refractory to systemic therapy
Surgical
- Surgical decompression for mass effect or hydrocephalus
- Biopsy is both diagnostic and may relieve local compression
- Subtotal resection combined with steroids for IgG4-HP with significant mass effect (Liu et al. 2026)
Treatment by Etiology
| Cause | Treatment |
|---|---|
| IHP | Corticosteroids; azathioprine/methotrexate if refractory |
| IgG4-HP | Corticosteroids first-line; rituximab for refractory |
| ANCA-HP (GPA) | Corticosteroids + cyclophosphamide or rituximab (induction); MTX or MMF (maintenance) |
| Sarcoid-HP | Corticosteroids ± MTX/azathioprine |
| TB-HP | Anti-tubercular therapy + corticosteroids |
| Fungal-HP | Antifungal therapy (e.g., amphotericin B, voriconazole) |
Sources: Bradley and Daroff's, p. 2586; Shimojima 2023 [PMID 37062439]; Liu et al. 2026 [PMID 41827958]
8. Recent Updates (2023-2026)
1. ANCA-HP as a CNS-Limited AAV Subtype (2023)
Shimojima & Sekijima (Autoimmun Rev 2023, [PMID 37062439]) established that ANCA-related HP may represent a CNS-limited form of AAV not captured by existing classification criteria. MPO-ANCA positivity dominates (more than PR3-ANCA). HP can be the initial manifestation of AAV in 3-4% of patients. Rituximab is now recommended for refractory ANCA-HP.
2. MRI Patterns for Immune-Mediated HP (2023)
Matias et al. (Acad Radiol 2023, [PMID 36882352]) systematically described distinct MRI patterns for GPA, IgG4-RD, neurosarcoidosis, and rheumatoid pachymeningitis, using both conventional and advanced MR sequences. This paper reinforces gadolinium-enhanced MRI as the cornerstone of diagnosis and monitoring.
3. IgG4-HP - High Misdiagnosis Rate and Atypical Manifestations (2026)
Liu et al. (Diagnostics 2026, [PMID 41827958]) reviewed 34 cases of IgG4-HP and found a 38.5% misdiagnosis rate (most commonly misdiagnosed as meningioma). Key findings: 73.5% male predominance, mean age 48.6 years, headache in 58.8%. Skull destruction with subcutaneous mass is an atypical but recognized presentation. Histopathology with serum IgG4 is the gold standard. Glucocorticoids alone or combined with immunosuppressants achieved favorable outcomes in 96% of cases.
4. Cerebral Venous Thrombosis as a Complication (2026)
Wang et al. (BMC Neurol 2026, [PMID 41808071]) highlighted recurrent cerebral venous thrombosis as a complication of IgG4-related HP, underscoring the need for vascular imaging (MRV/CT venography) in all HP patients.
5. IgG4-HP with Multi-System Involvement (2025)
A Frontiers in Immunology 2025 report described IgG4-RD presenting with simultaneous retroperitoneal fibrosis and spinal pachymeningitis, reinforcing the importance of whole-body imaging (CT/PET) to detect systemic disease in all HP cases.
6. Intrathecal Rituximab (2023)
For refractory IgG4-RHP not responding to systemic rituximab, intrathecal rituximab has been explored as a novel targeted delivery approach ([PMID 37292126]).
7. Neurological Involvement Prevalence in IgG4-RD
A recent study (2024-2025, Practical Neurology) found neurological involvement in 22% of IgG4-RD patients, with hypertrophic pachymeningitis accounting for 35% of neurological manifestations (behind neuro-ophthalmologic disease at 59%). This stresses the need for neurological screening in all newly diagnosed IgG4-RD patients.
Summary Table
| Domain | Key Points |
|---|---|
| Etiology | IgG4-RD (10-20%), ANCA-AAV/GPA, sarcoid, RA, TB, syphilis, fungi, idiopathic |
| Pathophysiology | Fibro-inflammatory dural thickening; lymphoplasmacytic infiltration; storiform fibrosis; compression of CNs, cord, venous sinuses |
| Clinical | Headache (most common), cranial neuropathies, ataxia, seizures, myelopathy/radiculopathy |
| Differential | Meningioma, GPA vs. IgG4-RD, neurosarcoidosis, TB, lymphoma, intracranial hypotension |
| Radiology | Gadolinium T1-MRI: dural thickening + enhancement; "sandwich" pattern in IgG4; T2 hypointensity with fibrosis; whole-body CT/PET for staging |
| Treatment | Corticosteroids (first-line); azathioprine/MTX/MMF (maintenance); cyclophosphamide or rituximab (refractory/ANCA); surgical decompression for mass effect |
| Recent | IgG4-HP misdiagnosed as meningioma in 38.5%; CVT as complication; intrathecal rituximab; ANCA-HP as CNS-limited AAV; neurological involvement in 22% IgG4-RD |
References:
- Bradley and Daroff's Neurology in Clinical Practice, 8th Ed. - pp. 2586-2590
- Adams and Victor's Principles of Neurology, 12th Ed. - pp. 648-649
- Shimojima Y & Sekijima Y. Autoimmun Rev 2023 [PMID 37062439]
- Matias TB et al. Acad Radiol 2023 [PMID 36882352]
- Liu XM et al. Diagnostics 2026 [PMID 41827958]
- Wang Y et al. BMC Neurol 2026 [PMID 41808071]
- Balaban DT et al. Front Neurol 2023 [PMID 37292126]
- Yang L et al. Pract Neurol 2025; 25:217-227
Give me answer
The full, detailed answer on Hypertrophic Pachymeningitis was already provided in my previous response above. It covers all the topics you requested:
- Etiology - IgG4-RD, ANCA/GPA, sarcoid, RA, TB, syphilis, fungi, idiopathic
- Pathophysiology - fibro-inflammatory dural thickening, lymphoplasmacytic infiltration, storiform fibrosis, nerve/venous sinus compression
- Clinical Features - headache (most common), cranial neuropathies, ataxia, seizures, myelopathy
- Differential Diagnosis - meningioma, GPA vs. IgG4-RD, TB, lymphoma, intracranial hypotension
- Radiological Features - gadolinium MRI patterns (with actual MRI images), "sandwich" sign, T2 hypointensity, whole-body CT/PET
- Treatment - corticosteroids (first-line), azathioprine/MTX/MMF, cyclophosphamide, rituximab (refractory), surgical decompression
- Recent Updates (2023-2026) - IgG4-HP misdiagnosis rate 38.5%, CVT as complication, intrathecal rituximab, ANCA-HP as CNS-limited AAV
Please scroll up to read the complete answer. If you have a specific section you want me to expand, or a particular aspect you want clarified, let me know.
Can you provide full answer I didn’t get full answer
Here is the complete, full answer on Hypertrophic Pachymeningitis:
HYPERTROPHIC PACHYMENINGITIS (HP) - Complete Review
DEFINITION
Hypertrophic pachymeningitis is a rare, chronic inflammatory disorder characterized by diffuse or localized thickening of the dura mater. On MRI, it appears as gadolinium-enhancing dural thickening. It may involve the cranial dura, spinal dura, or both simultaneously. When no systemic cause is identified after full workup (cultures, serology, biopsy), the term Idiopathic Hypertrophic Pachymeningitis (IHP) is applied.
The term is somewhat confusing because the pia and arachnoid may be equally involved in the inflammatory thickening, and all three membranes may be bound together by dense fibrous adhesions.
- Adams and Victor's Principles of Neurology, 12th Ed., p. 648
1. ETIOLOGY
HP is classified as Secondary (identifiable cause) or Idiopathic.
A. Immune-Mediated / Autoimmune
| Condition | Key Notes |
|---|---|
| IgG4-Related Disease (IgG4-RD) | Accounts for ~10-20% of HP cases; now the most recognized immune cause; associated with autoimmune pancreatitis, sclerosing cholangitis, salivary gland disease |
| ANCA-Associated Vasculitis (AAV) | Especially Granulomatosis with Polyangiitis (GPA); 3-4% of AAV patients develop HP; MPO-ANCA predominates over PR3-ANCA in HP-AAV |
| Rheumatoid Arthritis | Granulomatous dural infiltration |
| Sarcoidosis | Neurosarcoidosis with dural involvement |
| Sjögren Syndrome | |
| Systemic Lupus Erythematosus | |
| Behçet Disease | |
| Giant Cell Arteritis | |
| Polyarteritis Nodosa | Rare; case-based evidence |
B. Infectious
- Syphilis - historically the first described cause (Charcot and Joffroy described pachymeningitis cervicalis hypertrophica)
- Tuberculosis - chronic granulomatous dural thickening
- Fungal infections (Aspergillus, Cryptococcus)
- Lyme disease
- HTLV-1
- Pseudomonas aeruginosa (malignant external necrotizing otitis)
- Cysticercosis
- HIV-related
C. Neoplastic
- Dural carcinomatosis
- Lymphoma (primary CNS or systemic)
- Meningioma (actually a mimicker, not a true HP cause)
- Metastatic disease from adjacent skull bone
D. Other / Miscellaneous
- Trauma / post-surgical dural reaction
- Intracranial hypotension (spontaneous or post-lumbar puncture) - venous engorgement mimics dural enhancement
- Mucopolysaccharidosis (fibroblast-mediated dural thickening)
E. Idiopathic
- Diagnosis of exclusion
- Biopsy shows small mature lymphocytes, plasma cells, and epithelioid histiocytes without identifiable cause
Sources: Bradley and Daroff's eBOX 104.10; Adams and Victor's p. 648; Shimojima & Sekijima, Autoimmun Rev 2023 [PMID 37062439]
2. PATHOPHYSIOLOGY
General Mechanism
The dura mater undergoes a chronic fibro-inflammatory reaction driven by immune cell infiltration. This process leads to progressive dural thickening, fibrosis, and adhesion formation. All three meningeal layers may become involved and fused by dense fibrous adhesions.
IgG4-RD Mechanism
- CD4+ T follicular helper (Tfh) cells and regulatory T cells are pathologically activated
- Tfh cells drive plasmablast and plasma cell differentiation, producing IgG4 antibodies
- Characteristic histological triad:
- Dense lymphoplasmacytic infiltration with IgG4+ plasma cells (>10-40 per HPF)
- Storiform (cartwheel) fibrosis - swirling pattern of dense collagen deposition
- Obliterative phlebitis - inflammatory occlusion of small veins
- IgG4+/IgG+ plasma cell ratio ≥30%
- Activated fibroblasts and myofibroblasts perpetuate fibrosis
- The same process affects pancreas, salivary glands, kidneys, retroperitoneum, lungs
ANCA-Associated Mechanism (GPA)
- ANCAs (anti-MPO or anti-PR3) activate neutrophils and monocytes
- Neutrophil degranulation releases proteases and reactive oxygen species
- Granulomatous inflammation with giant cells forms in dura
- Importantly, classic GPA histology (necrotizing granulomatous vasculitis) is not always present in dural biopsies
- T-cell mediated fibrosis follows the acute inflammatory phase
Consequences of Dural Thickening
- Cranial nerve compression as nerves traverse thickened basal dura (most common mechanism of deficits)
- Venous sinus compression/thrombosis - raised intracranial pressure, hydrocephalus
- Cerebral venous thrombosis - increasingly recognized complication, especially in IgG4-HP
- Spinal cord compression - myelopathy
- Nerve root compression - radiculopathy, amyotrophy
Sources: Adams and Victor's p. 648-649; Shimojima 2023 [PMID 37062439]; Liu et al. 2026 [PMID 41827958]
3. CLINICAL FEATURES
HP has a subacute to chronic onset (weeks to months). Course may be monophasic, progressive, or relapsing-remitting.
Cranial HP
| Symptom / Sign | Details |
|---|---|
| Headache | 40-70%; most common presenting symptom; persistent, pressure-like, progressive |
| Cranial neuropathies | 30-70%; most frequent are CN II, III, IV, VI (diplopia, ophthalmoplegia, visual loss), CN V (facial numbness/pain), CN VIII (sensorineural hearing loss) |
| Visual disturbance | Diplopia, visual impairment, sudden visual loss (particularly ANCA-HP) |
| Ataxia | Cerebellar involvement by posterior fossa dural thickening |
| Seizures | When hemispheric or parasagittal dura is involved |
| Hydrocephalus | Venous sinus compression; presents with headache, cognitive slowing |
| Mental dullness | Raised ICP or direct cortical involvement |
Spinal HP
- Cervical region most commonly affected (historically called pachymeningitis cervicalis hypertrophica)
- Myelopathy: progressive sensorimotor deficits below level of compression
- Radiculopathy: root pain, paresthesia, sensory loss
- Amyotrophy of upper limbs (cervical cord/root involvement)
- Paraparesis: cord compression at any level
IgG4-HP Specific Profile
- Male predominance (~2-3:1), peak age 40-70 years
- 38.5% misdiagnosis rate - most commonly mistaken for meningioma
- Extraneurological manifestations in >50%: pancreas, salivary glands, kidneys, lacrimal glands, lungs, retroperitoneum
- Subacute onset, may relapse during or after steroid taper
ANCA-HP (GPA) Specific Profile
- ENT manifestations: otitis media, sinusitis, mastoiditis - important clues
- Sudden visual loss is a warning feature
- HP may be the initial clinical episode of AAV in 3-4% of patients
- CNS-only ANCA-HP may not meet classification criteria for GPA
CSF Findings
- Elevated protein (common)
- Lymphocytic pleocytosis (mild to moderate)
- Sterile cultures
- Glucose - normal or mildly low
- Plasma cells not prominent in IgG4-HP (contrast with neurosyphilis/Listeria meningitis)
- Elevated IgG fraction may be seen in IgG4-HP
Sources: Bradley and Daroff's p. 2586; Adams and Victor's p. 648; Practical Neurology 2025; Liu et al. 2026 [PMID 41827958]
4. DIFFERENTIAL DIAGNOSIS
Full Differential of Thickened Enhancing Dura on MRI
Idiopathic
- Idiopathic cranial or spinal pachymeningitis
Intracranial Hypotension
- Spontaneous intracranial hypotension
- Post-lumbar puncture (smooth, diffuse enhancement - usually distinguishable)
Infectious
- Lyme disease
- Syphilis / Neurosyphilis
- Mycobacterium tuberculosis
- Fungal infections (Aspergillus, Cryptococcus)
- Cysticercosis
- HTLV-1
- Malignant external otitis (Pseudomonas)
Systemic Autoimmune / Vasculitic
- IgG4-Related Disease
- Granulomatosis with Polyangiitis (ANCA-AAV)
- Rheumatoid Arthritis
- Sarcoidosis
- Behçet Disease
- Sjögren Syndrome
- Giant Cell Arteritis
- SLE
- Isolated CNS angiitis
- Vogt-Koyanagi-Harada syndrome
Malignancy
- Dural carcinomatosis (breast, prostate, lung are common primaries)
- Lymphoma (primary CNS or systemic)
- Meningioma (most common mimicker)
- Metastatic disease from adjacent skull bone
Trauma / Post-surgical
GPA vs. IgG4-RD - The Critical Diagnostic Dilemma
| Feature | GPA (ANCA-HP) | IgG4-RD HP |
|---|---|---|
| ANCA | MPO or PR3 positive (80-90%) | Usually negative |
| Serum IgG4 | May be mildly elevated | Significantly elevated (>1350 μg/mL) |
| ENT involvement | Sinusitis, otitis media, mastoiditis - common | Less prominent |
| Orbital involvement | Possible | Common (lacrimal, infraorbital nerve) |
| Other organs | Lungs, kidneys (GN) | Pancreas, salivary glands, kidneys (tubular), retroperitoneum |
| Histology - dura | Granulomatous; NOT always necrotizing vasculitis | Storiform fibrosis, obliterative phlebitis, IgG4+ plasma cells |
| Treatment | Cyclophosphamide or rituximab + steroids | Steroids, rituximab for refractory |
Key Point: Both conditions share overlapping clinical and biological features - same age range, multiple organ involvement, possible IgG4 elevation, and eosinophilia. Biopsy remains essential.
Sources: Bradley and Daroff's eBOX 104.10; Shimojima 2023 [PMID 37062439]; Matias et al. 2023 [PMID 36882352]; Gautier et al. 2023 [PMID 36738953]
5. RADIOLOGICAL FEATURES
MRI Brain and Spine with Gadolinium - Gold Standard
Fig. 104.39 from Bradley and Daroff's Neurology - Axial (A) and coronal (B) T1-weighted post-gadolinium images. The enhancement pattern here is thin and diffuse; other cases show localized or irregular thickening.
Fig. 29-7 from Adams and Victor's Neurology - Gadolinium-enhanced MRI showing diffuse rheumatoid pachymeningitis. This patient had severe headaches, hydrocephalus, and mental dullness.
T1 Post-Contrast (Gadolinium) - Primary Sequence
- Diffuse or localized dural thickening with enhancement - the hallmark
- Enhancement can be:
- Smooth and thin (suggests intracranial hypotension - venous engorgement)
- Irregular, nodular, or localized (more suggestive of inflammatory or neoplastic cause)
- Mass-like (may mimic meningioma - especially IgG4-HP)
- "Sandwich" pattern - peripheral enhancement of thickened dura - described in IgG4-HP
- Tentorium, falx, skull base, and convexity dura can all be involved
T2 / FLAIR
- Thickened dura is often hypointense on T2 due to dense fibrous tissue - a key distinguishing feature from leptomeningeal disease
- Marked T2 hypointensity favors IgG4-HP (dense storiform fibrosis)
- Adjacent brain parenchyma: look for edema, hydrocephalus
DWI (Diffusion Weighted Imaging)
- Diffusion restriction suggests lymphoma or abscess
- No restriction in typical inflammatory HP
Advanced MRI Patterns by Etiology
| Etiology | Predominant MRI Pattern |
|---|---|
| IgG4-HP | Nodular/mass-like; T2 hypointense; "sandwich" enhancement; skull base, tentorium, falx |
| GPA (ANCA-HP) | Irregular thickening; skull base; sinus/mastoid involvement on CT |
| Neurosarcoidosis | Leptomeningeal + pachymeningeal; cranial nerve enhancement |
| Rheumatoid HP | Diffuse smooth circumferential enhancement |
| TB | Skull base enhancement; leptomeningitis; calcification |
| Intracranial hypotension | Diffuse smooth bilateral enhancement; brain sag; subdural collections |
| Lymphoma | Nodular, mass-like; diffusion restriction |
CT Findings
- Dural thickening (hyperdense)
- Sinus/mastoid opacification (GPA clue)
- Skull destruction (atypical IgG4-HP, metastasis)
- Calcification (TB, old sarcoid)
Whole-Body Imaging
- CT chest/abdomen/pelvis - mandatory to detect systemic IgG4-RD (pancreatic enlargement, retroperitoneal fibrosis, lymphadenopathy) or malignancy
- PET-CT - identifies hypermetabolic extraneurological lesions to guide biopsy
MR Venography / CT Venography
- Indicated when venous sinus thrombosis is suspected (headache + papilledema)
- Increasingly recommended in all HP cases given recent recognition of CVT as a complication
Sources: Bradley and Daroff's p. 2586-2590; Adams and Victor's p. 648; Matias et al. 2023 [PMID 36882352]
6. DIAGNOSTIC WORKUP (Stepwise)
Step 1 - Neuroimaging
- MRI brain + spine with gadolinium (mandatory)
- CT brain if MRI contraindicated
Step 2 - Blood Tests
- CBC, ESR, CRP
- ANA, ANCA (MPO, PR3), RF, anti-CCP
- ACE (angiotensin-converting enzyme)
- Serum IgG subclasses (IgG1-IgG4), total IgG
- VDRL/TPHA (syphilis serology)
- HIV serology
- Lyme serology
- Fungal serology (Cryptococcus antigen, Aspergillus galactomannan)
- Serum calcium, LDH
Step 3 - CSF Analysis
- Cell count and differential
- Protein and glucose
- Culture (bacterial, TB, fungal)
- Cytology
- Oligoclonal bands
- ACE level
- VDRL
- Flow cytometry (if lymphoma suspected)
Step 4 - Systemic Imaging
- Chest CT (sarcoid, TB, malignancy)
- CT abdomen/pelvis (IgG4-RD organs)
- Whole-body PET-CT
Step 5 - Dural Biopsy (Gold Standard)
- Required for definitive diagnosis
- Histology: H&E staining, IgG/IgG4 immunostaining, cultures
- IgG4-HP criteria: >10-40 IgG4+ plasma cells/HPF, IgG4+/IgG+ ratio ≥30%, storiform fibrosis, obliterative phlebitis
- Serum IgG4 >1350 μg/mL supports IgG4-HP diagnosis
7. TREATMENT
A. Corticosteroids - First-Line for All Immune-Mediated HP
- Prednisolone / Prednisone
- Starting dose: 0.5-1 mg/kg/day (IHP and IgG4-HP)
- Starting dose: 1 mg/kg/day (ANCA-HP / GPA)
- Gradual taper over several months
- Favorable response seen in ~96% of IgG4-HP cases
- Relapse is common during or after taper - monitor closely with repeat MRI
- Pulse IV methylprednisolone (1g/day x 3 days) for severe/acute presentations
B. Steroid-Sparing Immunosuppressants
| Agent | Use |
|---|---|
| Azathioprine | IHP, IgG4-HP (steroid-sparing maintenance) |
| Methotrexate | IHP, IgG4-HP, ANCA-HP maintenance |
| Cyclophosphamide | ANCA-HP/GPA (induction, especially severe) |
| Mycophenolate Mofetil (MMF) | ANCA-HP maintenance; IgG4-HP |
C. Rituximab (Anti-CD20 Monoclonal Antibody)
- First-choice for refractory HP across all immune-mediated subtypes
- Mechanism: depletes B cells and plasmablasts
- Particularly effective in:
- Refractory ANCA-HP (GPA) - now used as induction therapy in some centers
- Refractory IgG4-HP
- Dose: typically 375 mg/m² weekly x 4, or 1g x 2 doses separated by 2 weeks
- Intrathecal rituximab explored for CNS-refractory IgG4-RHP (novel approach, 2023)
D. Surgical Management
- Surgical decompression for mass effect, spinal cord compression, or hydrocephalus
- Biopsy - both diagnostic and may relieve local compression
- Subtotal/gross resection combined with steroid therapy in IgG4-HP with significant mass effect
- VP shunting for obstructive hydrocephalus
E. Treatment by Specific Etiology
| Cause | Treatment Protocol |
|---|---|
| Idiopathic HP (IHP) | Prednisolone → azathioprine or MTX if refractory → rituximab |
| IgG4-HP | Prednisolone (first-line) → rituximab for refractory; surgical for mass effect |
| ANCA-HP (GPA) | Corticosteroids + cyclophosphamide or rituximab (induction); MTX or MMF (maintenance) |
| Neurosarcoidosis-HP | Corticosteroids ± MTX/azathioprine/infliximab |
| Rheumatoid HP | Steroids + DMARDs (MTX, leflunomide) |
| TB-HP | Anti-tubercular therapy (HRZE x 2 months → HR x 4-7 months) + corticosteroids |
| Fungal HP | Amphotericin B (induction) → azole (consolidation/maintenance) |
| Syphilitic HP | Penicillin G IV |
| Lyme HP | Ceftriaxone IV |
F. Monitoring
- Repeat MRI at 3-6 months to assess response
- Serum IgG4 levels for monitoring IgG4-HP
- ANCA titers for monitoring ANCA-HP
- Watch for relapse during taper (dose adjustment required)
- Long-term follow-up is mandatory due to relapse risk
Sources: Bradley and Daroff's p. 2586; Shimojima 2023 [PMID 37062439]; Liu et al. 2026 [PMID 41827958]; Balaban et al. 2023 [PMID 37292126]
8. RECENT UPDATES (2023-2026)
1. ANCA-HP as a CNS-Limited AAV Subtype (Shimojima & Sekijima, Autoimmun Rev 2023)
ANCA-related HP may represent a CNS-limited form of ANCA-associated vasculitis not captured by existing AAV classification criteria. HP can be the initial manifestation of AAV in 3-4% of patients. MPO-ANCA positivity dominates over PR3-ANCA. ENT manifestations (otitis media, sinusitis, mastoiditis) are robustly associated. Rituximab is now recommended for refractory ANCA-HP.
[PMID 37062439]
2. MRI Patterns for Immune-Mediated HP (Matias et al., Acad Radiol 2023)
Systematically described distinct MRI patterns for GPA, IgG4-RD, neurosarcoidosis, and rheumatoid pachymeningitis using both conventional and advanced MR sequences. Advanced sequences (DWI, perfusion, spectroscopy) help distinguish from neoplastic mimickers.
[PMID 36882352]
3. IgG4-HP - High Misdiagnosis Rate and Atypical Manifestations (Liu et al., Diagnostics 2026)
Analysis of 34 IgG4-HP cases found:
- 73.5% male predominance, mean age 48.6 years
- Headache in 58.8% of cases
- 38.5% misdiagnosis rate - most commonly mistaken for meningioma
- Skull destruction with subcutaneous mass formation - an atypical but recognized presentation
- Histopathology + serum IgG4 = gold standard for diagnosis
- Glucocorticoids alone or combined with immunosuppressants achieved favorable outcomes in 96% of cases
- Rituximab effective for refractory cases [PMID 41827958]
4. Cerebral Venous Thrombosis as a Complication (Wang et al., BMC Neurol 2026)
Recurrent cerebral venous thrombosis (CVT) is a recognized complication of IgG4-related HP, underscoring the need for MR venography / CT venography in all HP patients presenting with headache, papilledema, or neurological deficits.
[PMID 41808071]
5. IgG4-HP with Multi-System Involvement (Frontiers Immunology 2025)
IgG4-RD can present simultaneously with retroperitoneal fibrosis and spinal pachymeningitis, reinforcing the importance of whole-body CT/PET to detect systemic disease in all newly diagnosed HP cases.
6. Intrathecal Rituximab for Refractory IgG4-RHP (Balaban et al., Front Neurol 2023)
For IgG4-RHP refractory to systemic rituximab, direct intrathecal delivery of rituximab has been explored as a novel targeted therapeutic approach, showing promising results in a case report.
[PMID 37292126]
7. Neurological Involvement in IgG4-RD More Common Than Previously Thought (Practical Neurology 2025)
A major study found neurological involvement in 22% of IgG4-RD patients, with HP accounting for 35% of neurological manifestations (behind neuro-ophthalmologic disease at 59%). This calls for routine neurological screening in all newly diagnosed IgG4-RD patients.
8. Pachymeningitis-ANCA Dual Positivity (Gautier et al., Autoimmun Rev 2023)
Cases of HP with concurrent IgG4-RD and ANCA positivity have been reported, highlighting significant overlap and calling for comprehensive antibody testing in all HP patients.
[PMID 36738953]
SUMMARY TABLE
| Domain | Key Points |
|---|---|
| Etiology | IgG4-RD (10-20%), ANCA/GPA, sarcoid, RA, TB (historically syphilis), fungi, idiopathic |
| Pathophysiology | Fibro-inflammatory dural thickening; lymphoplasmacytic infiltration; storiform fibrosis; CN/cord/venous sinus compression |
| Clinical | Headache (most common 40-70%), cranial neuropathies, ataxia, seizures, myelopathy/radiculopathy; spinal HP preferentially cervical |
| CSF | Elevated protein, lymphocytic pleocytosis, sterile |
| Differential | Meningioma (most common mimicker), GPA vs. IgG4-RD, TB, lymphoma, intracranial hypotension |
| Radiology | Gadolinium T1-MRI - dural thickening + enhancement; "sandwich" sign in IgG4; T2 hypointensity in fibrosis; whole-body CT/PET for staging |
| Biopsy | Gold standard - storiform fibrosis, IgG4+ plasma cells >10-40/HPF, IgG4+/IgG+ ratio ≥30% |
| Treatment | Corticosteroids (first-line all); azathioprine/MTX/MMF (maintenance); cyclophosphamide + rituximab (ANCA/refractory); surgical for mass effect |
| Recent updates | 38.5% IgG4-HP misdiagnosis; CVT as complication; intrathecal rituximab; ANCA-HP as CNS-limited AAV; neurological involvement in 22% of IgG4-RD |
REFERENCES
- Bradley and Daroff's Neurology in Clinical Practice, 8th Ed. - pp. 2586-2590
- Adams and Victor's Principles of Neurology, 12th Ed. - pp. 648-649
- Shimojima Y, Sekijima Y. Hypertrophic pachymeningitis in ANCA-associated vasculitis. Autoimmun Rev 2023 [PMID 37062439]
- Matias TB et al. Immune-Mediated Hypertrophic Pachymeningitis and its Mimickers: MRI Findings. Acad Radiol 2023 [PMID 36882352]
- Liu XM et al. IgG4-Related Disease Manifested as Hypertrophic Pachymeningitis. Diagnostics 2026 [PMID 41827958]
- Wang Y et al. Recurrent CVT associated with IgG4-related HP. BMC Neurol 2026 [PMID 41808071]
- Balaban DT et al. Treatment of IgG4-RHP with intrathecal rituximab. Front Neurol 2023 [PMID 37292126]
- Gautier F et al. Pachymeningitis associated with IgG4-RD and ANCA positivity. Autoimmun Rev 2023 [PMID 36738953]
- Yang L et al. IgG4-related disease in the nervous system. Pract Neurol 2025;25:217-227
This is a shared conversation. Sign in to Orris to start your own chat.