20 year old female with chronic cough
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic cough" young adults diagnosis management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
"chronic cough" diagnosis guidelines
I now have comprehensive content. Let me compile the full clinical answer.
Chronic Cough in a 20-Year-Old Female
Chronic cough is defined as cough lasting >8 weeks. In a young woman with no smoking history and no ACE inhibitor use, the differential is distinct from older patients and deserves a systematic approach.
Management Algorithm
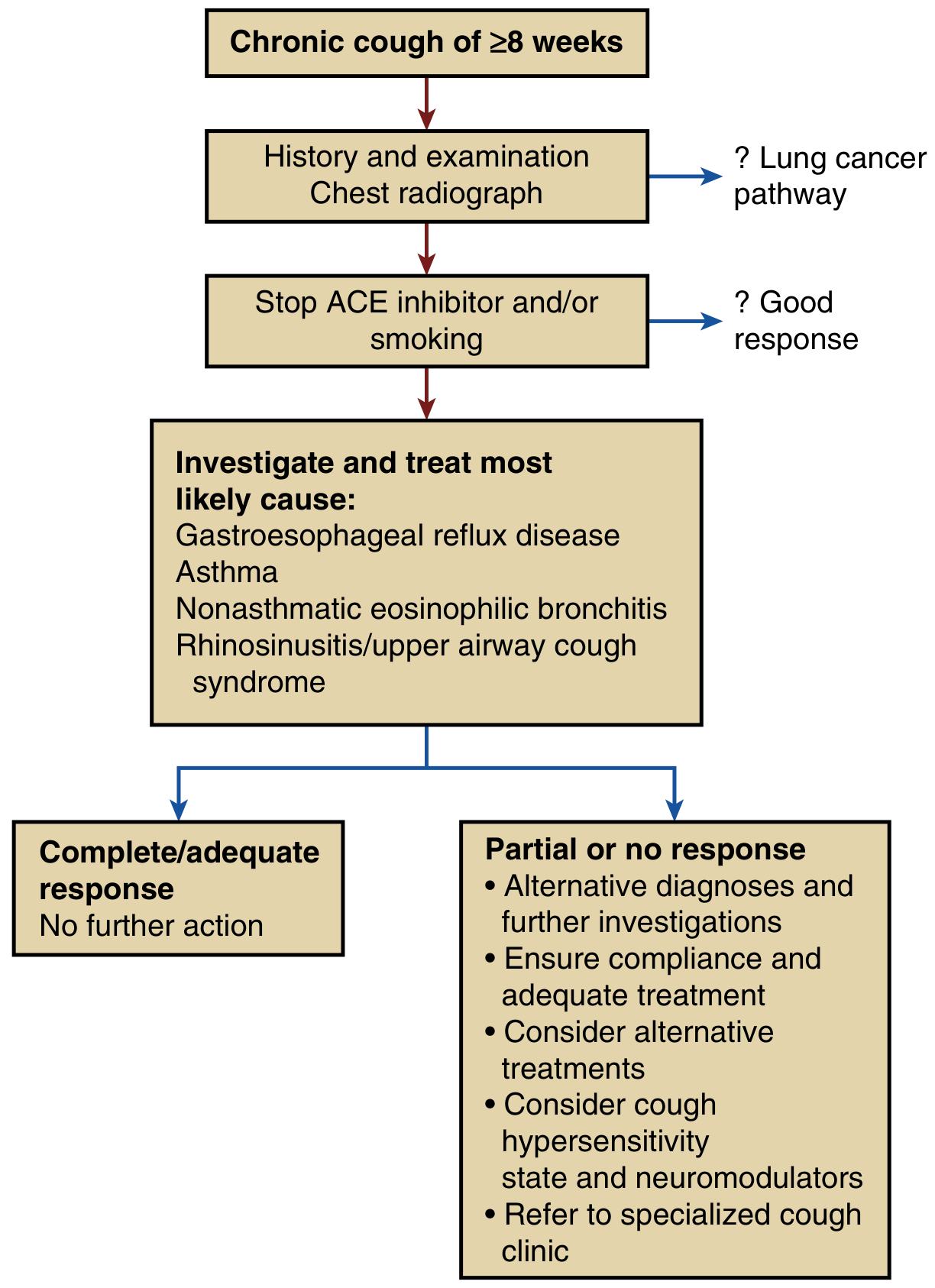
Algorithm for chronic cough management in adults (Murray & Nadel's Textbook of Respiratory Medicine)
Differential Diagnosis
Most Common Causes (account for the vast majority of cases with a normal CXR)
| Cause | Key Features |
|---|---|
| Upper Airway Cough Syndrome (UACS) / Postnasal Drip | Sensation of drip at back of throat, frequent throat clearing, cobblestoning of posterior pharynx, rhinosinusitis on CT |
| Asthma / Cough-Variant Asthma | Episodic, worse with exercise, cold air, laughing; wheeze may be absent; reversible airflow obstruction on spirometry |
| Gastroesophageal Reflux Disease (GERD) | Retrosternal burning, worse after meals or recumbency; cough may occur without typical heartburn symptoms |
| Non-Asthmatic Eosinophilic Bronchitis (NAEB) | Dry cough, normal spirometry and methacholine challenge, >3% eosinophils on induced sputum; treated with inhaled corticosteroids |
Postnasal drip, asthma, and GERD are classically described as the "big three," but clinical experience shows they do not account for all cases, and strict adherence to this triad can miss other causes. - Murray & Nadel's Textbook of Respiratory Medicine
Important Causes in Young Women Specifically
- Sarcoidosis - can present in young adults with chronic dry cough and an abnormal chest radiograph (bilateral hilar lymphadenopathy). Sarcoidosis and Hodgkin's disease are specifically flagged by Harrison's as causes of chronic cough in young adults that may produce no other symptoms but show radiographic findings.
- Pertussis (whooping cough) - consider in subacute-to-chronic cough; paroxysmal, may have posttussive vomiting or whooping quality; vaccine immunity wanes in adults.
- Postinfectious cough - common after viral URI, typically self-limiting but can last weeks to months.
- Cough Hypersensitivity Syndrome (CHS) - dry or minimally productive cough with a tickle/sensitivity in the throat; worsened by talking, laughing, exertion; more common in women than men; can persist for years; a neuropathic model (sensitized sensory nerve endings).
- Psychogenic / Habit Cough - diagnosis of exclusion; consider if cough is absent during sleep and has a honking, barking quality.
- Vocal cord dysfunction / Inducible laryngeal obstruction - episodic inspiratory stridor/cough, often misdiagnosed as asthma.
- Bronchiectasis - productive cough, recurrent infections; consider if there is a history of childhood infections, immunodeficiency, or cystic fibrosis (in a 20-year-old, CF should be on the radar).
- Cystic fibrosis - in a young woman with chronic productive cough, CF must be considered even if mild/atypical phenotype.
- Pulmonary tuberculosis - worldwide a leading cause of chronic cough; consider with relevant exposure history, weight loss, or night sweats.
Workup
Step 1 - History
- Duration, character (dry vs. productive, sputum color/amount)
- Timing (nocturnal, postprandial, seasonal, exercise-related)
- Associated: wheeze, dyspnea, heartburn, postnasal drip, throat clearing, rhinorrhea
- Triggers: cold air, laughing, perfumes, smoke
- Medications: ACE inhibitors (unlikely in a 20-year-old, but check)
- Smoking history, occupational/environmental exposures
- Family history (CF, asthma, atopy)
- Recent respiratory infections
- Features of cough hypersensitivity: tickling sensation, cough with talking, paroxysms
Step 2 - Physical Examination
- Nasal exam: mucosa edema, polyps, secretions
- Pharynx: cobblestoning (postnasal drip)
- Chest: wheeze, crackles
- Ear canals: Arnold's nerve irritation can trigger cough
- Nails: clubbing
- General: lymphadenopathy, skin changes (sarcoidosis)
Step 3 - Initial Investigations
| Investigation | Rationale |
|---|---|
| Chest X-ray | Mandatory first step; may reveal hilar lymphadenopathy (sarcoid/lymphoma), infiltrates (TB, pneumonia), bronchiectasis |
| Spirometry with bronchodilator reversibility | Diagnose asthma/COPD |
| Methacholine challenge test | If spirometry normal but asthma suspected; high sensitivity for asthma |
| Skin prick testing / specific IgE | Allergic rhinitis assessment |
| Sinus CT | If rhinosinusitis suspected and not responding to empiric treatment |
| Induced sputum for eosinophils | Diagnose eosinophilic bronchitis (>3% eosinophils, normal methacholine) |
| 24-hr esophageal pH monitoring | Gold standard for GERD; indicated if symptoms suggest reflux or empiric PPI trial fails |
Step 4 - Further Investigations (if initial workup unrevealing)
- HRCT chest - bronchiectasis, interstitial disease, sarcoidosis
- Fiberoptic bronchoscopy - small central tumors, mucosal biopsy (sarcoid, eosinophilic infiltration), culture
- Sweat chloride / CFTR genotyping - if CF suspected
- Laryngoscopy - vocal cord dysfunction, laryngopharyngeal reflux
- Pertussis serology (IgA/IgG) - if subacute/chronic and no other explanation
Empiric Treatment Approach
Treat the most likely diagnosis based on history and examination while investigations are pending:
| Suspected Cause | First-Line Treatment |
|---|---|
| UACS / Allergic rhinitis | Intranasal corticosteroid + antihistamine; add ipratropium for excessive secretions |
| Asthma / Cough-variant asthma | Inhaled corticosteroid (ICS) + short-acting bronchodilator as needed |
| GERD | PPI once daily for 8 weeks; lifestyle measures (elevate head of bed, weight loss if applicable); note: empiric PPI has low specificity |
| Eosinophilic bronchitis | Inhaled corticosteroids |
| Postinfectious | Reassurance; consider short course of intranasal steroids if nasal symptoms present |
Refractory / Unexplained Cough
If cough persists despite treating identified causes:
- Reassess compliance with therapy
- Consider cough hypersensitivity syndrome as the primary or contributing mechanism
- Pharmacologic neuromodulation: low-dose gabapentin (300-1800 mg/day) or pregabalin have evidence for refractory chronic cough; amitriptyline (low dose) is also used
- Speech pathology / cough suppression therapy: breathing exercises, cough suppression techniques, laryngeal hygiene - particularly effective in women with concurrent vocal cord dysfunction or muscle tension dysphonia
- Refer to specialist cough clinic
Cough hypersensitivity syndrome is more common in women and presents as a dry cough with a tickle or sensitivity in the throat, worsened by talking, laughing, or exertion. It can last for years and is a diagnosis of exclusion. - Harrison's Principles of Internal Medicine 22E
Red Flags Requiring Urgent Workup
- Hemoptysis
- Weight loss, night sweats
- Clubbing
- Abnormal chest X-ray
- Stridor or signs of airway obstruction
- Immunosuppression or TB exposure
Summary Approach for This Patient
A 20-year-old female with chronic cough and no obvious red flags should have:
- Thorough history and physical examination
- Chest X-ray (exclude sarcoidosis, TB, lymphoma in this age group)
- Spirometry with reversibility testing
- Empiric treatment targeting the most likely cause identified clinically (usually UACS, asthma, or GERD)
- Stepwise investigation if initial workup and treatment are unrevealing
- Keep CF in mind if productive cough and recurrent infections
Sources: Harrison's Principles of Internal Medicine 22E (2025), Murray & Nadel's Textbook of Respiratory Medicine, Goldman-Cecil Medicine
A 2025 practice guideline (PMID: 41385480) reaffirms this stepwise algorithm for adult cough diagnosis and treatment.
20 year old female with chronic cough since 21 days and had a history of smoking
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
"pertussis" adults cough diagnosis
I now have comprehensive material. Let me compose the full clinical answer.
Subacute Cough in a 20-Year-Old Female Smoker
Critical Clarification: This is Subacute Cough, Not Chronic
| Duration | Classification |
|---|---|
| < 3 weeks | Acute |
| 3 - 8 weeks | Subacute |
| > 8 weeks | Chronic |
At 21 days, this patient is at the boundary of acute and subacute cough. The diagnostic approach differs meaningfully from chronic cough. However, given her smoking history, certain chronic causes must still be considered even at this early stage.
Differential Diagnosis
Most Likely Causes
1. Postinfectious Cough (Most Common Cause of Subacute Cough)
The #1 cause of subacute cough overall. Mechanisms include:
- Postviral airway inflammation with bronchial hyperresponsiveness
- Mucus hypersecretion
- Upper airway cough syndrome (postnasal discharge)
- Unmasking of underlying asthma
Look for a history of preceding URI (runny nose, sore throat, fever) 1-3 weeks prior. Chest X-ray is typically normal.
"Postinfectious cough is the most likely cause of subacute cough. The mechanisms include postviral airway inflammation with bronchial hyperresponsiveness, mucus hypersecretion, upper airway cough syndrome (postnasal discharge), or asthma." - Tintinalli's Emergency Medicine
2. Pertussis (Bordetella pertussis) - Must Not Miss
Particularly important in a 20-year-old as vaccine immunity wanes by early adulthood.
Classic features:
- Paroxysmal coughing fits followed by an inspiratory whoop (may be absent in adults)
- Posttussive vomiting
- Cough worsens over the first 1-2 weeks (catarrhal → paroxysmal phase)
- Absence of fever between episodes
- Can last 6-10 weeks ("100-day cough")
Diagnosis: PCR nasopharyngeal swab (best sensitivity in first 3 weeks - this patient is still in window). Serology (IgA/IgG) if >3 weeks.
"The observed increased incidence of pertussis in adolescents and young adults is likely due to waning vaccine immunity with increasing age." - Tintinalli's Emergency Medicine
Note: A 2025 clinical review (PMID: 40387798) reaffirms that pertussis is underdiagnosed in adults and should be considered in any subacute cough.
3. Smoking-Related Airway Irritation / Acute Bronchitis
Cigarette smoking directly irritates airways and impairs mucociliary clearance, making smokers prone to:
- Prolonged cough after any respiratory infection
- Acute bronchitis with productive cough
- Early features of chronic bronchitis if smoking is ongoing
Smoking-induced coughing is usually worse in the morning and, with chronic bronchitis, usually productive. - Tintinalli's Emergency Medicine
Cessation of cigarette smoking is usually accompanied by a reduction in cough, most often within 4 to 5 weeks. - Murray & Nadel's Textbook of Respiratory Medicine
4. Asthma / Cough-Variant Asthma
Smoking is a known asthma trigger. Subacute cough following a URI can unmask previously undiagnosed asthma or represent a flare of known asthma.
- Cough worse at night, with exercise, cold air, laughing
- Episodic wheeze or dyspnea
- Spirometry may show reversible airflow obstruction; methacholine challenge if spirometry normal
5. Upper Airway Cough Syndrome (UACS) / Postnasal Drip
- Sensation of secretions dripping down the back of the throat
- Frequent throat clearing
- Can be allergic or non-allergic rhinitis/sinusitis
- Smoking worsens nasal mucosal inflammation
6. Atypical Pneumonia (Mycoplasma, Chlamydophila)
In a young adult with cough of 3 weeks, atypical organisms must be considered:
- Mycoplasma pneumoniae: dry/hacking cough, low-grade fever, "walking pneumonia"
- Chlamydophila pneumoniae: similar presentation
- Chest X-ray may show patchy infiltrates disproportionate to clinical severity
"Subacute cough caused by Bordetella pertussis, Mycoplasma pneumoniae, and Chlamydophila pneumoniae should prompt a chest radiograph, molecular testing, and appropriate antibiotic treatment." - Goldman-Cecil Medicine
7. Acute Exacerbation of Underlying Airway Disease
In a smoker, even at 20 years old, consider that she may have undiagnosed early airway disease (chronic bronchitis, mild COPD phenotype) that is now manifesting.
Less Likely But Important to Consider
| Diagnosis | Why Consider |
|---|---|
| Pneumonia | Smokers have impaired airway defenses; fever, productive cough, CXR changes |
| Pulmonary tuberculosis | If relevant exposure, weight loss, night sweats |
| GERD | Can trigger or worsen cough |
| Foreign body aspiration | Sudden onset cough without preceding illness |
| Smoking cessation (if recently quit) | Paradoxical increase in cough for 1-4 weeks as mucociliary function recovers |
Workup
Step 1 - Focused History
| Question | Significance |
|---|---|
| Preceding URI/fever? | Postinfectious cough |
| Paroxysmal fits + posttussive vomiting? | Pertussis |
| Wheeze, nocturnal cough, atopy? | Asthma |
| Heartburn, worse lying down? | GERD |
| Postnasal drip, throat clearing, rhinorrhea? | UACS |
| Productive sputum - color? | Bacterial infection, bronchitis |
| Current smoker or recently quit? | Quantity (pack-years), quitting status |
| Vaccinations: Tdap booster? | Pertussis vaccination status |
| Weight loss, night sweats, contacts? | TB |
Step 2 - Physical Examination
- Temperature, SpO₂, RR - rule out acute illness
- Nasal exam: polyps, secretions, mucosal edema
- Pharynx: cobblestoning, postnasal secretions
- Chest auscultation: wheeze, crackles, reduced breath sounds
- Lymphadenopathy
Step 3 - Investigations
| Test | Indication |
|---|---|
| Chest X-ray | Mandatory - pneumonia, TB, atypical features |
| Nasopharyngeal PCR for B. pertussis | Still in window at 21 days - order now or you'll miss it |
| Spirometry | If asthma or airflow obstruction suspected |
| Sputum culture (if productive) | Bacterial pathogens, AFB if TB considered |
| Mycoplasma/Chlamydophila serology or PCR | If walking pneumonia presentation |
| Peak flow variability | If cough-variant asthma suspected |
Note: "PCR and culture have decreasing sensitivity after the third week of coughing" for pertussis - this patient is at exactly that threshold. Act quickly. - Tintinalli's Emergency Medicine
Management
If Postinfectious (No Specific Pathogen Identified)
- Reassurance: most resolve within 3-8 weeks
- Treat any identified component (postnasal drip → intranasal steroid; bronchospasm → short-acting bronchodilator)
- Smoking cessation - single most important intervention; reduces cough within 4-5 weeks
- Honey + warm fluids for symptomatic relief
- Short course of inhaled bronchodilator if bronchial hyperresponsiveness suspected
If Pertussis Confirmed / Strongly Suspected
- Azithromycin 500 mg day 1, then 250 mg days 2-5 (macrolide of choice)
- Alternatively: clarithromycin or TMP-SMX
- Reduces transmission even if started late; may shorten illness if started in first 3 weeks
- Contact tracing and post-exposure prophylaxis for close contacts
- Advise Tdap booster for patient and household contacts
If Cough-Variant Asthma
- Inhaled corticosteroid (ICS) + short-acting bronchodilator
- Smoking cessation is mandatory
If Atypical Pneumonia
- Azithromycin or doxycycline for Mycoplasma or Chlamydophila
Smoking Cessation - Priority Regardless of Cause
Smoking is a direct cause and amplifier of cough at any age. At 20 years old, cessation now prevents progression to chronic bronchitis, COPD, and lung cancer. Offer:
- Brief counseling ("5 A's")
- Nicotine replacement therapy (NRT) - patch, gum, or lozenge
- Varenicline (most effective pharmacotherapy) or bupropion
Summary for This Patient
| Priority | Action |
|---|---|
| 1 | Chest X-ray |
| 2 | Nasopharyngeal PCR for pertussis (time-sensitive - within window) |
| 3 | Assess for and address smoking cessation |
| 4 | Empiric treatment targeting most likely cause (postinfectious/bronchospasm) |
| 5 | Spirometry if wheeze or airflow obstruction suspected |
| 6 | Return if not improving by 8 weeks → full chronic cough workup |
"If postinfectious, then assess for transient bronchial hyperresponsiveness, asthma, pertussis, upper airway cough syndrome, pneumonia, or an acute exacerbation of chronic bronchitis. Treatment is then directed at the presumed cause. If subacute cough is not postinfectious, it is evaluated and treated in the same manner as a chronic cough." - Tintinalli's Emergency Medicine
Sources: Tintinalli's Emergency Medicine, Murray & Nadel's Textbook of Respiratory Medicine, Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E
Trarment of chronic cough
Finding Sources
Finding Sources
Searching PubMed
"chronic cough" treatment guidelines
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative content to compile the full treatment guide. Let me write it up.
Treatment of Chronic Cough
The fundamental principle is: identify and treat the cause first. Symptom-directed suppression is only used when cause-specific treatment fails or no cause is found.
Step 1 - Remove Precipitating Agents First
Before any other therapy:
| Agent | Action |
|---|---|
| ACE inhibitor | Stop immediately; switch to ARB (does not cause cough). Reassess at 1 month. |
| Smoking | Cessation reduces cough within 4-5 weeks; mandatory in smokers |
| Environmental/occupational irritants | Identify and eliminate |
"Patients with chronic cough while on ACE inhibitor therapy should discontinue such therapy, with replacement by other appropriate treatments." - Murray & Nadel's Textbook of Respiratory Medicine
Step 2 - Cause-Directed Treatment
A. Upper Airway Cough Syndrome (UACS) / Postnasal Drip
| Drug | Details |
|---|---|
| Intranasal corticosteroid (1st line) | e.g., fluticasone, mometasone - local effect, minimal systemic side effects; head-down position for drops |
| Oral/intranasal antihistamine | Combined with nasal steroid; adds benefit |
| Intranasal ipratropium bromide | Dries excessive nasal secretions; useful add-on |
| Short course oral corticosteroid | For severe symptoms initially, then taper to topical |
| Antibiotics | Only if bacterial sinusitis confirmed |
B. Asthma / Cough-Variant Asthma
| Drug | Details |
|---|---|
| Inhaled corticosteroid (ICS) | First-line; reduces airway eosinophilic inflammation |
| Short-acting β₂ agonist (SABA) | e.g., salbutamol - as needed for symptoms |
| Long-acting β₂ agonist (LABA) | Added to ICS if inadequate control |
| Leukotriene receptor antagonist | e.g., montelukast - useful adjunct, especially in allergic component |
| Smoking cessation | Smoking is a direct asthma trigger |
C. Gastroesophageal Reflux Disease (GERD)
| Treatment | Details |
|---|---|
| Lifestyle measures | Elevate head of bed, weight loss, avoid coffee/fatty foods/late meals, avoid smoking |
| Proton pump inhibitor (PPI) | e.g., omeprazole 20-40 mg daily; give for minimum 8 weeks |
| H₂ antagonist | e.g., ranitidine - less effective than PPI but an option |
| Prokinetics | Domperidone, metoclopramide - limited evidence, potential side effects |
| Antireflux surgery | Laparoscopic fundoplication for refractory GERD-related cough; evidence unclear |
Note: Evidence does not support empiric PPI for cough without reflux symptoms. PPI is most effective when abnormal esophageal acid exposure is confirmed on pH monitoring. - Murray & Nadel's Textbook of Respiratory Medicine
D. Non-Asthmatic Eosinophilic Bronchitis (NAEB)
| Drug | Details |
|---|---|
| Inhaled corticosteroid | First-line; highly effective |
| Leukotriene inhibitor | Adjunct |
E. Chronic Bronchitis / COPD
| Treatment | Details |
|---|---|
| Smoking cessation | Single most important intervention |
| Short-acting bronchodilator (SABA/SAMA) | Salbutamol or ipratropium |
| Long-acting bronchodilator (LABA/LAMA) | For persistent symptoms |
| ICS + LABA combination | For airway inflammation |
| Mucolytics | Acetylcysteine, carbocysteine - reduce exacerbation frequency, ease expectoration |
F. Bronchiectasis
| Treatment | Details |
|---|---|
| Chest physiotherapy / postural drainage | Cornerstone - improves airway clearance |
| Inhaled β₂ agonists | Improve mucociliary clearance, reverse bronchoconstriction |
| Antibiotics | Targeted to cultured pathogens during infective exacerbations |
| Long-term macrolide | e.g., azithromycin 3x/week - reduces exacerbations and improves lung function |
G. Infective Tracheobronchitis / Postinfectious
| Treatment | Details |
|---|---|
| Appropriate antibiotics | Macrolide for pertussis/Mycoplasma; doxycycline for Chlamydophila |
| Treat postnasal drip component | Intranasal steroid if present |
| Short-acting bronchodilator | If bronchial hyperresponsiveness present |
Step 3 - Symptomatic / Cough Suppression Therapy
Used when cause-directed treatment fails, is unavailable, or cough hypersensitivity syndrome is the primary mechanism.
A. Non-Pharmacologic: Speech Pathology (First-Line for Refractory)
A structured program delivered by a speech therapist or respiratory physiotherapist:
- Breathing retraining exercises
- Cough suppression techniques (urge-to-cough control)
- Vocal and laryngeal hygiene training
- Psychoeducational counseling
Proven to improve cough symptom scores, cough counts, breathing, voice, and upper airway symptoms. Particularly effective in patients with concurrent muscle tension dysphonia or vocal cord dysfunction.
"Speech pathology management... has been shown to be effective in improving cough symptom scores and cough counts." - Murray & Nadel's Textbook of Respiratory Medicine
B. Pharmacologic Antitussives
1. Narcotic Antitussives (Most Potent)
| Drug | Details |
|---|---|
| Codeine | Standard centrally acting antitussive; mixed efficacy; risk of dependence, constipation, sedation |
| Slow-release morphine | For severe chronic refractory cough; reserved for cases significantly affecting quality of life or palliative use |
| Hydrocodone | Used in some guidelines for refractory cough |
"Most potent are narcotic cough suppressants, such as codeine, hydrocodone, or morphine, which are thought to act in the 'cough center' in the brainstem. The tendency to cause drowsiness and constipation and their potential for addictive dependence limit their appeal for long-term use." - Harrison's Principles of Internal Medicine 22E
2. Non-Narcotic Antitussives
| Drug | Mechanism | Notes |
|---|---|---|
| Dextromethorphan | Central; different site from opioids | OTC; as effective as codeine for acute/chronic cough; fewer side effects; avoid with MAOIs (serotonin syndrome risk) |
| Benzonatate | Inhibits sensory nerve activity in cough reflex pathway | Generally free of side effects; variable/unpredictable efficacy |
| Levodropropizine | Peripheral inhibition of sensory cough receptors | Favorable benefit/risk vs dextromethorphan |
| Inhaled lidocaine | Blocks voltage-gated Na⁺ channels | Transient suppression; risk of aspiration due to oropharyngeal anesthesia |
3. Neuromodulators (For Cough Hypersensitivity Syndrome / Refractory Cough)
These target the sensitized sensory neural pathways underlying chronic refractory cough - treating it as a neuropathic condition.
| Drug | Evidence | Dose (typical) |
|---|---|---|
| Gabapentin | RCT: reduced cough frequency, improved Leicester Cough QoL scores | 300-1800 mg/day in divided doses; titrate up |
| Pregabalin | RCT: combined with speech therapy reduced cough severity and frequency vs speech therapy alone | 75-300 mg/day |
| Amitriptyline | Prospective RCT: superior to codeine/guaifenesin for postinfectious cough | 10-25 mg at night (low dose) |
"In a randomized controlled double-blind trial in patients with refractory cough, gabapentin was effective in reducing cough frequency and visual analogue scores while improving Leicester Cough quality-of-life scores." - Murray & Nadel's Textbook of Respiratory Medicine
Both gabapentin and amitriptyline likely act via central antinociceptive mechanisms, modulating presynaptic NMDA receptors and reducing postsynaptic excitability.
4. Expectorants and Mucolytics
| Drug | Use |
|---|---|
| Acetylcysteine / Carbocysteine | Reduce sputum viscosity in chronic bronchitis; small reduction in exacerbations |
| Bromhexine / Ambroxol | Mucolytic; facilitates expectoration |
| Menthol / Eucalyptus | Aromatic; decongestant in nose; menthol inhibits capsaicin-induced cough via TRPM8 receptor |
| Honey + warm liquids | Safe, mild symptomatic benefit; supported for acute cough; useful adjunct |
| Demulcents | Protective layer on mucosal surface; component of most proprietary cough preparations |
Step 4 - Emerging / Novel Therapies
| Drug/Class | Target | Status |
|---|---|---|
| Gefapixant | P2X2/3 ATP receptor antagonist | Phase III trials - 75% reduction in cough frequency in phase II; main side effect: dysgeusia (taste disturbance) |
| Selective P2X3 antagonists | More specific than gefapixant | Early development; may reduce taste side effects |
| NaV1.7 blockers | Voltage-gated Na⁺ channel subunit | Preclinical |
| NK-1 receptor antagonists | Neurokinin-1 in central cough pathways | Early phase II trials; improvement in cough frequency |
| TRPV1/TRPA1 antagonists | TRP channels on vagal afferents | Clinical trials failed for chronic cough |
| Alpha-7 nicotinic agonists | Central cough inhibition | In development |
"The most promising target currently is the ATP P2X2/3 receptor. A P2X2/3 antagonist, gefapixant, has shown efficacy in suppressing chronic cough in phase II clinical trials with a reduction in cough frequency of 75%." - Murray & Nadel's Textbook of Respiratory Medicine
Summary Treatment Table
(From Murray & Nadel's Textbook of Respiratory Medicine)
| Cause | Treatment |
|---|---|
| Asthma / cough-variant asthma | Bronchodilators + ICS |
| Eosinophilic bronchitis | ICS; leukotriene inhibitors |
| Allergic rhinitis / postnasal drip | Topical nasal steroids + antihistamines + ipratropium |
| GERD | Lifestyle changes + H₂ antagonist or PPI |
| ACE inhibitor | Discontinue → switch to ARB |
| Chronic bronchitis / COPD | Smoking cessation + COPD therapy |
| Bronchiectasis | Postural drainage + antibiotics + airflow therapy |
| Infective tracheobronchitis | Antibiotics + treat postnasal drip |
| Chronic cough (all) | Speech and language therapy |
| Refractory cough affecting QoL | Amitriptyline or gabapentin |
| Severe chronic refractory cough | Slow-release morphine |
When to Refer
- No response after treating identified cause(s)
- Diagnosis uncertain
- Consider: specialist cough clinic, pulmonologist, gastroenterologist (pH monitoring), ENT (laryngoscopy), speech pathologist
Sources: Murray & Nadel's Textbook of Respiratory Medicine, Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine, Goldman-Cecil Medicine
A 2025 German Respiratory Society practice guideline (PMID: 41385480) supports this stepwise, cause-directed approach with neuromodulators reserved for refractory cases.
This is a shared conversation. Sign in to Orris to start your own chat.