Please elaborate about diagnosis and management of infertility due to hydrosalpinx and chronic endometritis
Reading File
Finding Sources
Finding Sources
Searching PubMed
hydrosalpinx infertility IVF management
Searching PubMed
chronic endometritis infertility diagnosis treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading Article
PMID: 38764191
Reading Article
PMID: 41684313
Searching the Web
hydrosalpinx salpingectomy proximal occlusion IVF outcomes 2024 2025 guidelines
I now have comprehensive information from multiple textbooks and recent systematic reviews. Let me compile the full, detailed response.
Infertility Due to Hydrosalpinx and Chronic Endometritis: Diagnosis and Management
PART 1: HYDROSALPINX
Pathophysiology and Impact on Fertility
A hydrosalpinx results from distal tubal occlusion, causing fluid accumulation within the fallopian tube lumen. The fluid is not merely a passive obstruction - it actively impedes embryo development and implantation through several mechanisms:
- Mechanical reflux: Hydrosalpinx fluid can reflux into the uterine cavity, directly washing out embryos or altering the endometrial environment
- Toxic effect: The fluid contains cytokines, prostaglandins, and reactive oxygen species that are embryotoxic
- Endometrial receptivity: Hydrosalpinx fluid impairs expression of endometrial adhesion molecules (e.g., integrins, leukemia inhibitory factor) that are necessary for implantation
- Altered uterine contractility: The fluid may alter myometrial peristalsis
The clinical significance is substantial: a meta-analysis of 14 studies (1,004 patients) confirmed that IVF pregnancy rates are significantly lower in the presence of hydrosalpinges compared to tubal-factor infertility without hydrosalpinx. - Berek & Novak's Gynecology
Etiology
Hydrosalpinx is most commonly a consequence of:
- Pelvic inflammatory disease (PID), particularly Chlamydia trachomatis and Neisseria gonorrhoeae
- Endometriosis
- Prior pelvic or abdominal surgery
- Appendicitis with peritonitis
Diagnosis
1. Transvaginal Ultrasound (TVUS)
- The primary screening tool
- Shows a fluid-filled, elongated, folded adnexal structure with characteristic "incomplete septa" (cogwheel sign on cross-section)
- Sensitivity ~95% for detecting hydrosalpinx
2. Hysterosalpingography (HSG)
- Demonstrates the dilated tube and confirms distal occlusion
- Useful for evaluating bilateral disease and proximal patency simultaneously
3. Diagnostic Laparoscopy
- The gold standard for tubal assessment
- Provides direct visualization and allows chromopertubation
- Also permits concurrent surgical intervention
4. Sonohysterography / Saline Infusion Sonography
- Can sometimes show retrograde flow of saline into the tube
5. MRI
- Reserved for complex cases when ultrasound is inconclusive; provides excellent soft-tissue detail
Management
The management goal is removal or functional blockage of the hydrosalpinx before ART, as the fluid's toxic and mechanical effects substantially reduce IVF success rates.
Surgical Options
1. Salpingectomy (preferred)
Salpingectomy prior to IVF significantly improves both pregnancy and live birth rates compared to IVF performed with the fallopian tubes in situ. It is the most definitive treatment because it eliminates the source of toxic fluid entirely.
A 2025 network meta-analysis (Pérez-Milán et al., Ultrasound Obstet Gynecol, PMID 38764191) including 9 RCTs found:
- Salpingectomy and laparoscopic tubal occlusion (LTO) significantly increased clinical pregnancy rates vs. no treatment (OR 2.24 and 2.55 respectively)
- Salpingectomy and ultrasound-guided aspiration significantly increased ongoing pregnancy rates vs. no treatment
- LTO achieved the highest SUCRA ranking for live birth rate
- No intervention showed significant differences in live birth rate between active treatments, though all active treatments outperformed expectant management
2. Laparoscopic Proximal Tubal Occlusion (LTO)
- Clips or bipolar coagulation of the proximal tube prevents fluid from reaching the uterine cavity
- A reasonable alternative when salpingectomy is technically difficult (e.g., dense adhesions, poor ovarian reserve concerns)
- Preserves the possibility of future tubal surgery, though this is rarely relevant in IVF-bound patients
- The 2025 NMA ranked LTO as highly effective and potentially safer with regard to ovarian reserve impact than salpingectomy
3. Hysteroscopic Proximal Tubal Occlusion (Essure/intratubal device)
- Can be performed under hysteroscopic guidance
- Useful when laparoscopy carries high surgical risk
- Less outcome data available compared to laparoscopic approaches
4. Ultrasound-Guided Transvaginal Aspiration
- Minimally invasive; done at time of egg retrieval or shortly before
- Significantly improves ongoing pregnancy rates vs. no treatment per 2025 NMA
- High recurrence rate (fluid re-accumulates) is the main drawback
- Reserved for patients who decline surgery or are poor surgical candidates
5. Sclerotherapy
- Ultrasound-guided aspiration followed by instillation of a sclerosing agent (e.g., tetracycline, ethanol)
- The 2025 NMA found sclerotherapy significantly increased live birth rate vs. no treatment in observational data, and was ranked safer regarding ovarian stimulation response
- Limited RCT data; not yet first-line
6. Salpingostomy
- Creation of a new tubal opening - can be considered in younger patients (<35 years) with mild distal disease, intact tubal mucosa, and absent or minimal adhesions
- Pregnancy rates: 30-34.6% following salpingostomy in well-selected patients
- Associated with ~7.9% ectopic pregnancy rate
- Should be followed by IVF if pregnancy does not occur within 12-18 months
- Not recommended as a hydrosalpinx treatment when IVF is the primary plan
Decision Framework
| Clinical Scenario | Preferred Approach |
|---|---|
| Accessible tube, planning IVF | Salpingectomy (laparoscopic) |
| Dense peritubal adhesions, high surgical risk | Laparoscopic proximal occlusion |
| Poor surgical candidate, unilateral | Aspiration ± sclerotherapy |
| Young patient (<35), excellent tubal mucosa, not planning IVF yet | Salpingostomy ± fimbrioplasty |
| Bilateral involvement, IVF planned | Bilateral salpingectomy |
Key point: Any active treatment is superior to expectant management before IVF. The choice between salpingectomy and LTO depends on surgical access, tube viability, and ovarian reserve concerns (as salpingectomy near the ovary could theoretically reduce ovarian reserve if the blood supply is compromised). - Berek & Novak's Gynecology, p. 2061
PART 2: CHRONIC ENDOMETRITIS (CE)
Definition and Prevalence
Chronic endometritis is a low-grade, persistent inflammation of the endometrial lining, distinct from acute endometritis. It is defined histopathologically by the presence of plasma cells in the endometrial stroma - a finding not seen in normal endometrium.
Prevalence in the context of infertility/ART:
- ~2.8% in the general infertile population
- 7-14% in patients with recurrent pregnancy loss (RPL)
- Up to 56% in patients with documented recurrent pregnancy loss in some series
- 14-67% in patients with recurrent implantation failure (RIF) undergoing IVF
Etiology and Associated Conditions
CE occurs in association with:
- Chronic pelvic inflammatory disease - most common
- Retained gestational tissue - post-partum or post-abortion
- Intrauterine contraceptive devices
- Tuberculosis - from miliary spread or tuberculous salpingitis (important in endemic regions; always consider in recent emigrants)
- STIs - Chlamydia trachomatis is particularly important; may be associated with both acute and chronic infiltrates; the organism may not be detected by culture
- Non-specific (idiopathic) - ~15% of cases have no identifiable cause
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 928
- Robbins & Kumar Basic Pathology
Mechanisms Linking CE to Infertility
CE impairs fertility through multiple mechanisms:
- Altered uterine receptivity: Inflammation dysregulates expression of adhesion molecules (integrins, L-selectin ligand, HOXA-10) and cytokines required for embryo implantation
- Endometrial microbiome disruption: Pathological bacteria (particularly Gardnerella, Streptococcus, Enterococcus, Escherichia coli) may outcompete the protective Lactobacillus-dominant microbiome
- Altered NK cell activity: Uterine natural killer (uNK) cells are critical for successful trophoblast invasion; CE alters their number and function
- Altered secretory transformation: The inflammatory milieu impairs normal secretory phase maturation of the endometrium, reducing the implantation window
Diagnosis
1. Endometrial Biopsy - Histopathology (Gold Standard)
- Performed in the mid-luteal phase (days 20-24 of the cycle)
- The hallmark finding is plasma cells in the endometrial stroma (Fig. 22.20D above)
- Standard H&E may miss plasma cells in the late secretory phase (when the stroma is decidualized and plasma cells are harder to distinguish)
- Immunohistochemistry for CD138 (syndecan-1) - the current gold standard technique; CD138 is a plasma cell surface marker that allows unambiguous identification even when H&E is equivocal
- The diagnosis of CE requires CD138-staining for reliability - Creasy & Resnik's Maternal-Fetal Medicine
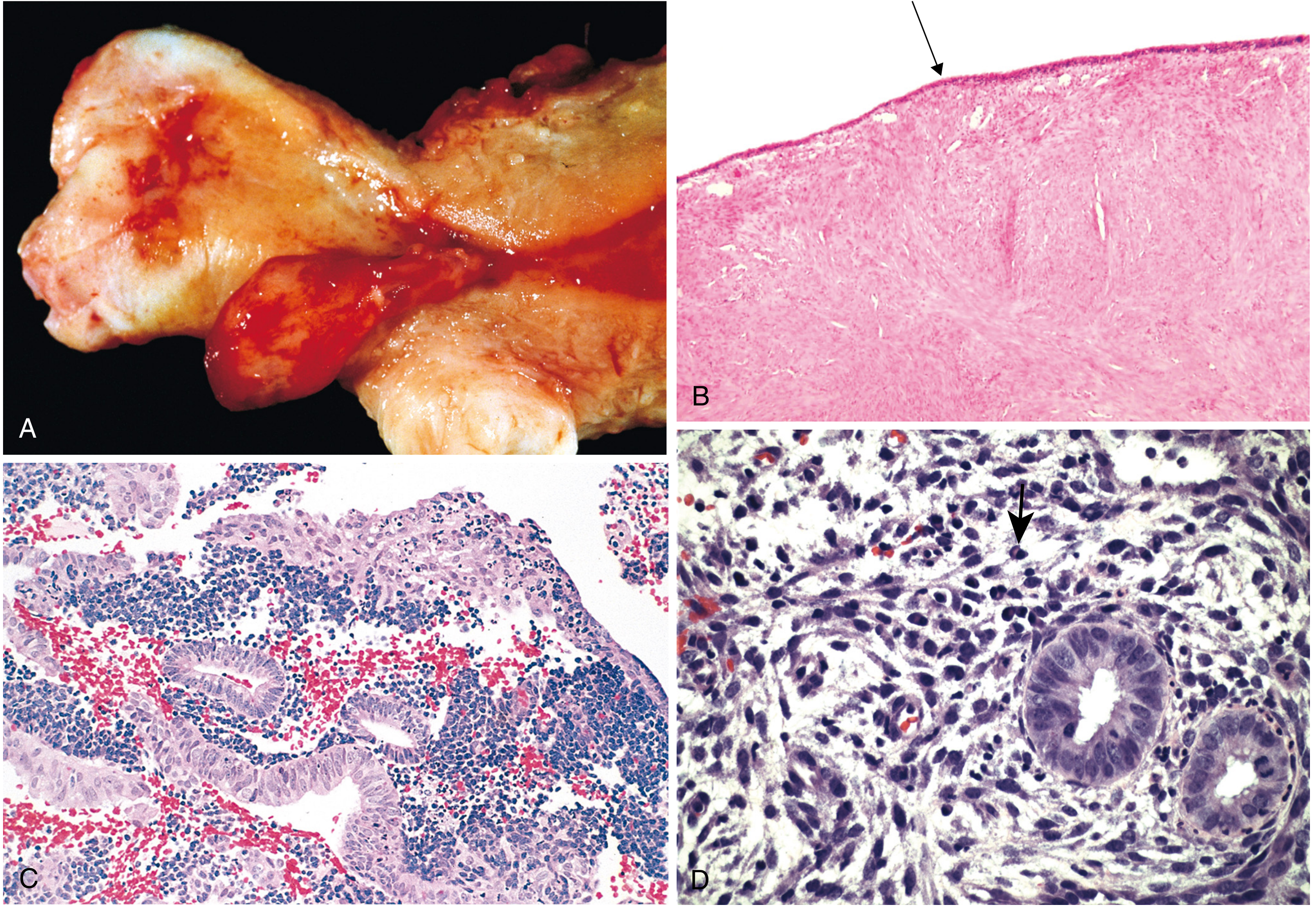
Fig 22.20D: Chronic endometritis with plasma cells (arrow). Note the characteristic plasma cells in the stroma, which are not found in normal endometrium. - Robbins, Cotran & Kumar
2. Hysteroscopy
- Provides direct visualization of the endometrial cavity
- Hysteroscopic findings suggestive of CE:
- Stromal edema (the most common finding)
- Micropolyps (small polypoid projections <1 mm, particularly at the endometrial surface near the tubal ostia)
- Focal or diffuse hyperemia (strawberry pattern)
- The absence of endometrial hyperemia and edema on fluid hysteroscopy has a high negative predictive value of 98.8% - making normal hysteroscopy very useful for ruling out CE
- Hysteroscopy is less specific than CD138-stained biopsy but provides additional information about the cavity - Creasy & Resnik's MFM
3. Microbiological Culture / PCR
- Endometrial culture or endometrial fluid PCR can identify causative organisms
- However, culture is frequently negative even in histologically confirmed CE (organisms may not grow)
- 16S rRNA sequencing or next-generation sequencing of the endometrial microbiome is increasingly used in research settings and emerging clinical practice
- If infection is suspected clinically, antibiotic therapy is indicated even with negative cultures - Robbins & Kumar
Diagnostic Algorithm
Infertility workup (especially RIF or RPL)
↓
Hysteroscopy (screening: micropolyps, hyperemia, edema?)
↓
Endometrial biopsy with H&E + CD138 immunostaining
↓
Positive (plasma cells in stroma) → Confirm CE
↓
Endometrial culture / PCR for pathogens
↓
Treat empirically or targeted antibiotic therapy
↓
Repeat biopsy 4-6 weeks post-treatment to confirm resolution
Management
Antibiotic Therapy (First-Line)
Treatment aims to eradicate causative organisms and allow endometrial healing before embryo transfer:
Standard first-line regimen:
- Doxycycline 100 mg twice daily × 14 days (most widely used; covers Chlamydia, Mycoplasma, and many gram-positives)
Alternative/combined regimens (used when initial doxycycline fails or when culture suggests resistant organisms):
- Metronidazole 500 mg twice daily × 14 days (for anaerobes, Gardnerella)
- Ciprofloxacin 500 mg twice daily × 14 days (for gram-negative organisms)
- Some centers use a combination (doxycycline + metronidazole or amoxicillin-clavulanate)
- For tuberculous endometritis: standard ATT (4-drug regimen for 6 months) is required
Confirming resolution:
- A repeat endometrial biopsy with CD138 staining 4-6 weeks after completing antibiotics is recommended before proceeding with embryo transfer
- Persistent CE after first-line antibiotics may require a second course with a different agent
Emerging / Adjunctive Therapies
A 2026 systematic review (Doroftei et al., Acta Obstet Gynecol Scand, PMID 41684313) evaluated microbiota-targeted therapies for CE-associated RIF:
- Clinical pregnancy rate of 50.5%, ongoing pregnancy rate 40.1%, and live birth rate 41.2% across antibiotic, probiotic, and nutraceutical interventions
- Probiotics (Lactobacillus-based preparations) may support restoration of a Lactobacillus-dominant endometrial microbiome after antibiotics
- The evidence base is limited with significant heterogeneity; standardized diagnostic criteria and larger RCTs are needed
Effect of Treatment on IVF Outcomes
Studies show that successful treatment of CE (confirmed by negative repeat biopsy) significantly improves IVF outcomes in patients with RIF:
- Higher implantation rates
- Higher clinical pregnancy rates
- Reduced miscarriage rates
- Most studies recommend deferring embryo transfer until resolution is confirmed histologically
However, major guidelines (including ASRM) do not currently recommend routine screening for CE in all infertility patients; the evidence is strongest for patients with RIF (≥3 failed implantations with good-quality embryos) and RPL.
SUMMARY TABLE
| Feature | Hydrosalpinx | Chronic Endometritis |
|---|---|---|
| Primary mechanism of infertility | Embryotoxic fluid, impaired receptivity, mechanical | Impaired implantation window, altered uterine immune environment |
| Diagnostic gold standard | Laparoscopy + chromopertubation | Endometrial biopsy + CD138 IHC |
| Primary investigation | TVUS (screening), HSG | Hysteroscopy + biopsy |
| Hallmark finding | Dilated fluid-filled adnexal structure | Plasma cells in endometrial stroma |
| Treatment of choice | Salpingectomy before IVF | Doxycycline 100 mg BD × 14 days |
| Alternative treatment | Laparoscopic proximal tubal occlusion | Metronidazole ± ciprofloxacin |
| Confirm resolution before IVF? | Yes - post-operative evaluation | Yes - repeat biopsy with CD138 |
| Prognosis after treatment | Significantly improved IVF live birth rates | Higher implantation/pregnancy rates in RIF |
Recent Evidence Updates
- [Systematic Review 2025, PMID 38764191] (Pérez-Milán et al.): Salpingectomy and LTO both significantly improve clinical pregnancy rates before IVF. LTO may be the preferred option for live birth rate by SUCRA ranking. Sclerotherapy appears safe regarding ovarian reserve. No treatment significantly surpasses others for live birth rate - treatment choice can be individualized.
- [Systematic Review 2026, PMID 41684313] (Doroftei et al.): Microbiota-targeted therapies (antibiotics, probiotics, nutraceuticals) show promising pregnancy outcomes in CE-associated RIF (LBR ~41%), but evidence quality is low and standardized protocols are lacking.
- [Systematic Review/Meta-Analysis 2025, PMID 39821822]: A meta-analysis explored the overlap between CE and endometriosis, suggesting shared inflammatory pathways - clinicians should screen for CE in patients with endometriosis-associated infertility.
This is a shared conversation. Sign in to Orris to start your own chat.