Compartment syndrome
Reading File
Finding Sources
Searching PubMed
"compartment syndrome" diagnosis management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full response:
Compartment Syndrome
Definition
Compartment syndrome is raised pressure within a fascial compartment to a level that compromises tissue perfusion, leading to ischemia and irreversible muscle and nerve damage from cellular anoxia. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Aetiology / Causes
| Category | Examples |
|---|---|
| Most common | Fractures (70%), soft tissue contusions (23%) |
| Vascular | Post-ischaemic reperfusion swelling, arterial/venous injury repair |
| Iatrogenic | Tight casts/dressings, extravasation of IV infusions (contrast under pressure), intraosseous (IO) needle complications |
| Haematological | Bleeding disorders, anticoagulation |
| Burns | Circumferential third-degree burns |
Note: The incidence associated with high-energy and low-energy injuries is nearly equal. Compartment syndrome can occur in open fractures - do not be falsely reassured by an open wound. - Bailey and Love's
Pathophysiology
- Injury causes bleeding/oedema within the confined fascial space
- Increased tissue pressure reduces microperfusion
- Progressive oedema elevates tissue pressure above capillary perfusion pressure, ending arterial flow
- In reperfusion injury: oxygen free radicals, lipid peroxidation, and intracellular calcium influx propagate cellular damage and oedema - forming a vicious cycle
- Result: muscle necrosis, nerve ischaemia, rhabdomyolysis
The more severe and prolonged the ischaemia (>6 hours), the more likely reperfusion compartment syndrome will develop. - Rosen's Emergency Medicine
Anatomical Compartments
The leg has 4 compartments and the forearm has 3 compartments - all susceptible:
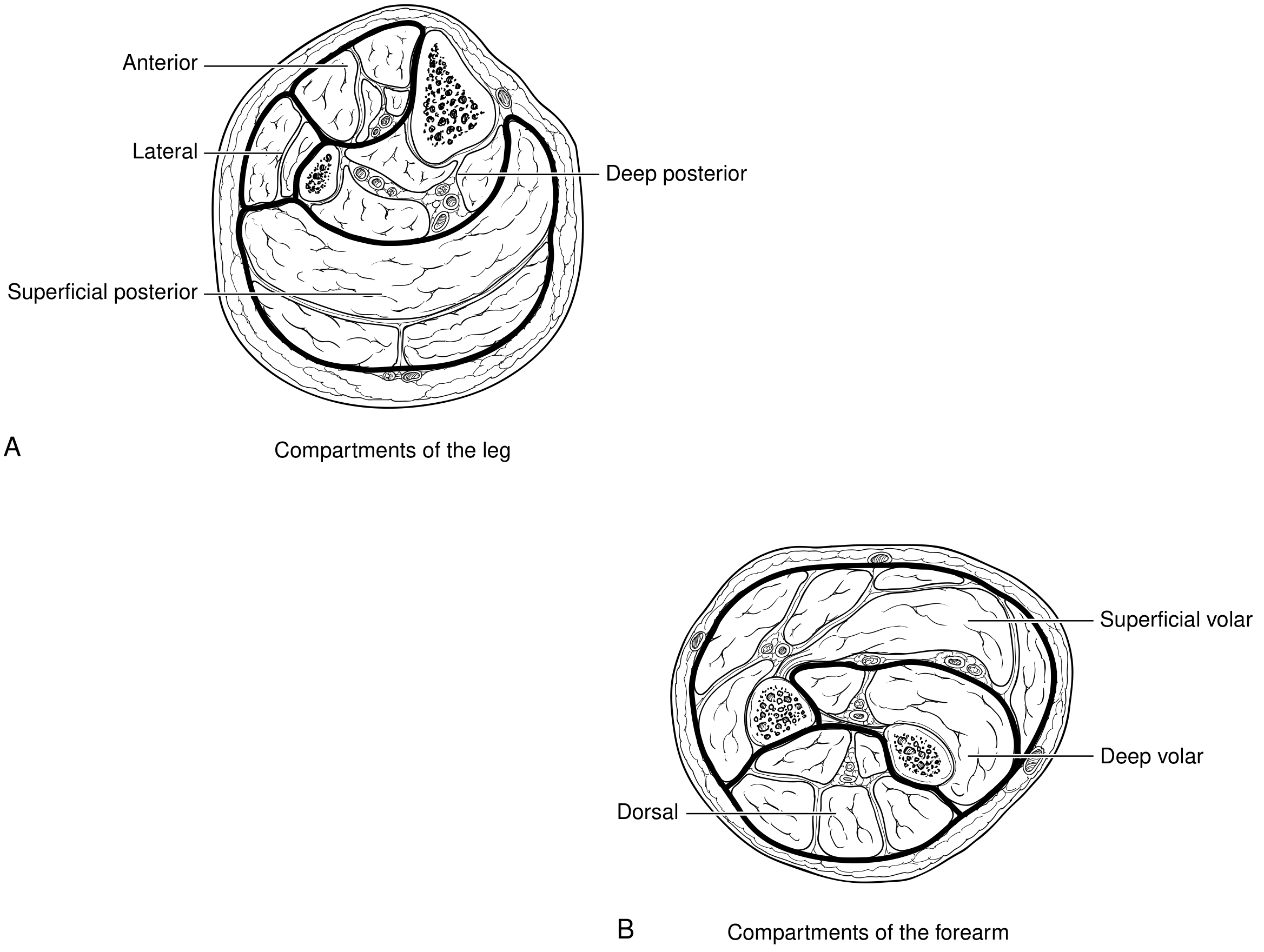
Leg:
- Anterior
- Lateral
- Superficial posterior
- Deep posterior
Forearm:
- Superficial volar
- Deep volar
- Dorsal
Thigh compartment syndrome is far less common because the large volume of the thigh requires massive bleeding before pressure exceeds capillary perfusion pressure; only 50% of thigh cases are associated with a femur fracture. - Rosen's Emergency Medicine
Clinical Features (The "6 P's")
| Sign | Significance |
|---|---|
| Pain out of proportion | Earliest and most sensitive sign |
| Pain on passive stretch | Highly characteristic - passive stretch of muscles within the compartment worsens pain |
| Paraesthesia | Early neural ischaemia |
| Pressure (tense, woody compartment) | Palpable tenseness of compartment |
| Paralysis | Late sign |
| Pallor / Pulselessness | Extremely late signs |
Key teaching point: Paralysis, numbness, pallor, and pulselessness are late signs. Pulselessness is an extremely late sign. By the time pulses are lost, significant irreversible damage has usually occurred. This is primarily a clinical diagnosis. - Bailey and Love's
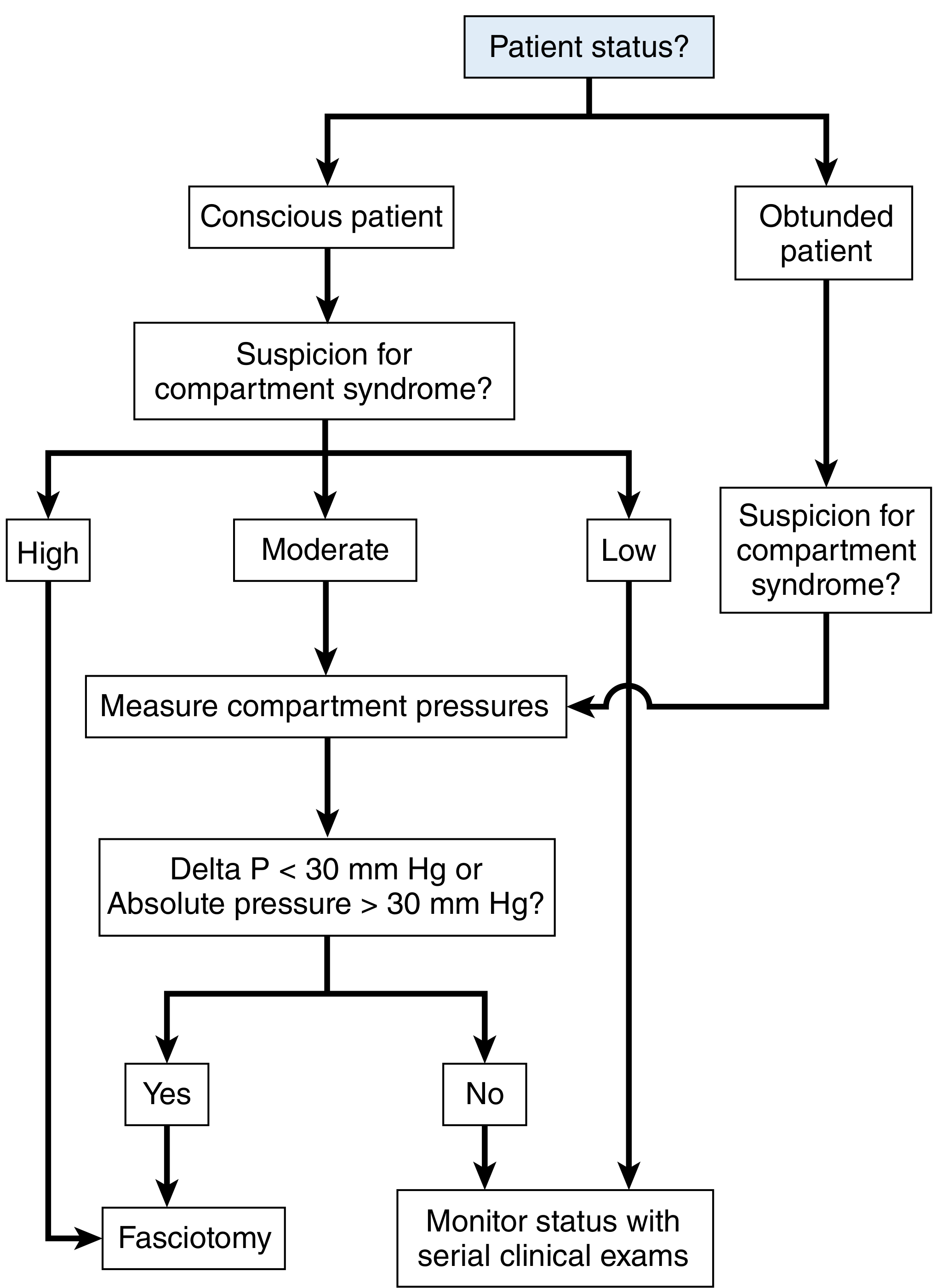
Compartment Pressure Measurement
Indicated when:
- Diagnostic uncertainty
- Altered level of consciousness (intubated patients, head injury, obtunded/sedated)
- Uncooperative patient
Technique: Measure multiple sites near (but not in) the fracture, in all compartments of the affected limb.
Thresholds for fasciotomy:
| Criterion | Threshold |
|---|---|
| Absolute compartment pressure | ≥ 30 mmHg |
| Delta P (Diastolic BP - Compartment pressure) | ≤ 30 mmHg |
| Alternative threshold (some sources) | Delta P < 10 mmHg warrants fasciotomy |
Elevated CPK and myoglobinuria are late markers of tissue destruction and should not be used to establish the diagnosis. - Current Surgical Therapy, 14e
Management Algorithm
Step 1: Immediate temporising measures
- Split all casts and dressings down to skin
- Elevate the extremity
- Seek senior/surgical input immediately
Step 2: Definitive treatment - Fasciotomy
- Fasciotomy should be performed emergently when clinical picture or pressure measurements indicate compartment syndrome
- When in doubt, release the compartment - an unnecessary fasciotomy leaves only a scar; a missed one risks limb loss
- Normal function was regained in 68% of patients when fasciotomy was performed within 12 hours of onset. - Campbell's Operative Orthopaedics, 15th Ed.
- Compartment pressure measurements are not required before fasciotomy if the clinical picture is clear
Fasciotomy techniques
Lower leg (4-compartment release):
- Performed through medial and lateral incisions
- All 4 compartments must be released
Forearm:
- Volar curvilinear incision releasing lacertus fibrosus proximally and carpal tunnel distally
- Interval between FCU and FDS for deep and superficial compartment release
- Dorsal forearm fascia released between ECRB and EDC
- If swelling extends to hand: carpal tunnel release + hand fasciotomies (hand surgery consult)
Post-fasciotomy:
- Wounds are left open
- Vacuum-assisted closure (VAC) device applied to decrease muscle oedema
- Avoid incomplete skin release or early closure - both lead to muscle necrosis
Step 3: Post-operative care
- Haemodynamic monitoring
- Serial neurovascular examinations
- Correct acidosis and electrolyte imbalances (potassium leak, hydrogen ion release)
- Rhabdomyolysis monitoring: target urine output >100 mL/hour until CPK <5,000 U/L
- IV fluid resuscitation
- Urine alkalisation with bicarbonate if significant tissue damage
Adjunctive therapy: Hyperbaric Oxygen (HBO)
- In impending compartment syndrome: HBO can improve oxygenation to hypoperfused tissues, decrease vasoconstriction and oedema, and potentially prevent progression to requiring fasciotomy
- Post-fasciotomy: HBO can prevent wound healing complications and accelerate recovery (~3-5 treatments required)
- Tintinalli's Emergency Medicine
Complications of Missed/Delayed Diagnosis
- Irreversible muscle necrosis
- Permanent nerve damage
- Rhabdomyolysis → acute tubular necrosis → renal failure
- Limb loss / amputation
- Volkmann's ischaemic contracture (forearm)
- Death (systemic effects)
"Delay in diagnosis and management of compartment syndrome has devastating consequences and can lead to both limb loss and mortality." - Current Surgical Therapy, 14e
Pitfalls to Avoid
- Falsely reassured by an open fracture - compartment syndrome still occurs
- Missing the diagnosis in obtunded or intubated patients - use pressure monitoring
- Relying on late signs (pallor, pulselessness) before acting
- Partial cast splitting that does not reach skin - ineffective decompression
- Using CPK/myoglobinuria to rule in or out compartment syndrome
- Attempting early closure of fasciotomy wounds
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed. | Rosen's Emergency Medicine | Campbell's Operative Orthopaedics, 15th Ed. | Current Surgical Therapy, 14e | Tintinalli's Emergency Medicine | Fischer's Mastery of Surgery, 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.